
Morgenstern, J. Massive hemorrhage: a very deep dive, First10EM, September 18, 2023. Available at:
https://doi.org/10.51684/FIRS.131635
Transfusion seems like the simplest intervention in medicine. The patient is losing blood, so let’s put some back in. Not much more complicated than an oil change. Sure, you need to use a specific brand, but as long as the system is topped up, everything should run just fine. Therefore, when someone (to be left unnamed) asked me to review the massive hemorrhage literature for a talk, I figured it was an easy preposition. In retrospect, hundreds of hours down the pubmed rabbit hole, perhaps this nightmare should have been obvious. With that in mind, I invite you to join me on a journey through the quagmire of massive transfusion (or massive hemorrhage if you prefer) literature. I am not sure this journey leads to any certainty, but those who embark will be better prepared for a future of trials that seem to contradict what is quickly becoming dogma.
Massive hemorrhage protocol triggers
Anyone trained in the last few decades will be familiar with the concept of restrictive transfusion strategies. These strategies are important, and evidence based, but they have a major limitation: hemoglobin based transfusion strategies are for stable patients. In resuscitation, we almost never have access to a hemoglobin, and we know that the hemoglobin does not accurately reflect early blood loss. When resuscitating hemorrhagic shock, we focus on vital signs and clinical findings, not a hemoglobin number. Focusing on a hemoglobin number can really lead you astray. (I have seen many critically ill GI bleed patients whose initial hemoglobin is reported as 90. An overly strict interpretation of the literature would tell you not to transfuse a patient with a hemoglobin of 90, but sticking with that interpretation in a critically ill patient is a good way to kill the patient.)
Massive transfusion protocols are resource intensive for hospitals, so there are clear harms to over-activation. On the other hand, preventable deaths from exsanguination are also a clear harm. We are walking a constant tight rope in the decision to activate.
Of course, evidence based medicine is always contextual. In some hospitals, the only way to get rapid access to PRBCs is by activating the massive hemorrhage protocol. In those hospitals, the protocol will have to be used much more liberally than in a hospital that can get 3 units of uncrossed blood and then reassess the patient.
There are a number of scores that sometimes get suggested for triggering massive transfusion protocols, but they all suffer from the many issues that plague our clinical decision rules. (Any time there are multiple rules for the same clinical scenario, it is a good hint that none of them work.) From an evidence based medicine standpoint, none of these rules are ready for clinical use. None have been shown to be better than clinical judgment. None have been shown to improve clinical outcomes.
The ABC score: The ABC score is a very simple score, based just on penetrating mechanism, systolic blood pressure, heart rate, and the FAST exam. A score of 2 or more is supposed to suggest the need for massive transfusion, but the entire evidence base is from retrospective chart reviews, and the sensitivity and specificity are both below 90% (and often way below 90%) even in low quality studies. (Nunez 2009; Cotton 2010; Brokamp 2012; Schroll 2018) Given that the 4 features are already aspects we are considering in a bleeding patient, I have a very hard time believing that this rule could possibly be better than clinical judgment. It clearly shouldn’t be used.
The TASH score: The TASH (or trauma associated severe hemorrhage) score is somewhat more complex than the ABC score, requiring blood work in addition to vital signs, FAST exam, and some physical exam findings. The evidence is no better, with sensitivities and specificities maximally in the mid 80%s, based on low quality retrospective studies. (Yucel 2006; Maegele 2011; Brokamp 2012) It also clearly shouldn’t be used.
The RABT score: The RABT (revised assessment of bleeding and transfusion) score includes 4 factors (penetrating injury, positive FAST, shock index over 1, and pelvic fracture), and a score of 2 or more is supposed to predict massive transfusion. Again, the score is only based on retrospective studies, has no comparison to clinical judgment, has no impact analysis, and has sensitivity and specificity less than 90%. (Hanna 2020) It shouldn’t be used.
The Shock Index: Although I teach students the shock index as a way of honing clinical judgment for sick patients, the evidence in the context of massive hemorrhage is moderate at best. For example, one retrospective study illustrated a shock index of 1 or greater only had a 68% sensitivity and 81% specificity for predicting need for massive transfusion. (Schroll 2018)
The guideline for Transfusion Ontario summarizes this reasonably well: “Despite concern that appropriate and timely activation are critical, there are no criteria with both high sensitivity and specificity for predicting the need for massive transfusion.” However, in a strange misstep of logic, they go on to make the statement that a massive hemorrhage protocol “shall have activation criteria”, which seems like a significant EBM mistake, and an indication of the general bias towards decision tools in medicine, despite their generally poor evidence. (Callum 2019)
EBM summary: The available evidence is worse than for most decision tools, which is really saying something. We don’t even have prospective validations with reasonable numbers, let alone comparisons to clinical judgment or implementation studies. There is absolutely no evidence these tools help practice.
Practical bottom line: There are no proven thresholds for massive hemorrhage protocol activation. This is a clinical decision based on the mechanism of injury, patient characteristics, vital signs, and local factors. If the patient still seems to need more blood after 2-3 units of red cells, that is my threshold to active massive transfusion.
Balanced transfusion
This topic is covered in more depth in this post. The short summary is that although you will often hear people recommend a 1:1:1 balanced transfusion strategy, there is very little evidence to support that position. In fact, the best evidence available (primarily through the PROPPR study) is that there is no difference between a 1:1:1 and a 1:1:2 strategy. (Although point estimates, and a number of disease oriented secondary outcomes look better in the 1:1:1 group). Importantly, there is no evidence that a 1:1:2 strategy is better than a much lower ratio.
In fact, although it is only a pilot study, the only RCT that compared a 1:1:1 strategy to a true control group (laboratory guided transfusion of platelets and plasma) seems to demonstrate much worse outcomes with the 1:1:1 strategy. (Nascimento 2013) Mortality was 32.5% with the 1:1:1 ratio, as compared to 14.3% in the control group, an absolute increase in mortality of 18.2% which came very close to being statistically significant (95% CI -0.4 to 36.8% absolute difference in mortality).
The RePHILL trial, discussed further below, also probably counts as a negative RCT looking at balanced transfusion, although it was only prehospital, didn’t include platelet transfusions, and ratios would have quickly caught up after hospital arrival. (Crombie 2022)
There is definitely not enough evidence to make strong conclusions in any direction, but the summary appears to be that using a higher ratio strategy results in patients getting more platelets and FFP without a clear difference in morbidity or mortality. (McQuilten 2018) When summarized that way, it sounds somewhat harmful to me.
One of the major evidence-based medicine limitations is that although massive transfusion protocols including balanced transfusion have been widely adopted in medicine, almost all of the evidence comes from the setting of trauma. Bleeding from medical conditions is often more complex (consider the baseline metabolic derangements in a cirrhotic patient bleeding from esophageal varices), and it is not clear how well this evidence extrapolates.
There is one chart review looking at all of the massive transfusion events over 4 years at a single hospital. (Mesar 2017) There were 865 events included, with 16,569 units of PRBC transfused. This hospital has clearly bought into the 1:1 strategy, as the overall ratios for all services in the hospital (trauma and not) were close to 1:1. 90% of the cohort is nontraumatic hemorrhage, so this practice has clearly been widely exported outside of the worldof trauma. There was no difference in outcomes based on FFP:PRBC ratio. The ratio was 1:1.5 for survivors and 1:1.4 for patients who died. This is despite evidence of survivorship bias, in that patients who received higher ratios of FFP also received more overall products (in other words, they were alive longer).
I think it is very important to be clear about the question we are asking when performing this research. The question isn’t whether FFP and platelets should be given at all, but whether empiric (and generally prophylactic) administration is better than laboratory guided transfusion. This is a really important distinction. In most hospitals, labs are such a lagging indicator that empiric therapy makes sense. But it is easy to imagine the introduction of rapid point of care testing, and if you can get a picture of the patient’s coagulation status in a matter of minutes, I can’t imagine that blind empiric administration of products with known side effects makes more sense than lab guided administration of only those products that are needed. Point of care testing is expensive, but so is unnecessary administration of blood products. I imagine the cost tips rapidly towards investing in testing infrastructure if your department sees more than a few of these patients a year.
I will go a little deeper into the individual evidence for both FFP and platelets below, as I think that evidence can help us understand whether empiric balanced transfusion is likely to be beneficial.
EBM summary: Some early observational data suggested potential benefit from balanced transfusions, but we need to be cautious about survivorship bias. There are physiological reasons balanced transfusions might work, but there are also important harms to consider. Thus far, the highest quality evidence has not demonstrated any benefit from balanced transfusion. My personal guess is that better evidence will tell us to use less empiric FFP and platelets in the future, not more.
Practical bottom line: You don’t want to be making this up on the fly, so you are likely to follow whatever your hospital’s protocol says. If you are designing a protocol, the best evidence is currently to use a 1:1:2 ratio of platelets to FFP to packed red cells. Empiric ratios are really only necessary in the acute phase of resuscitation. As test results become available, individual components can be tailored to lab results, or potentially viscoelastic studies (discussed below), as long as we are conscious of the lag and potential to fall behind.
Fresh frozen plasma
In emergency medicine, “balanced transfusion” has become the vogue, and it is generally thought about and assessed as a package deal. However, looking at the general evidence for the components might help us calibrate our expectations (especially considering that the only evidence that balanced transfusions might help comes from biased observational trials).
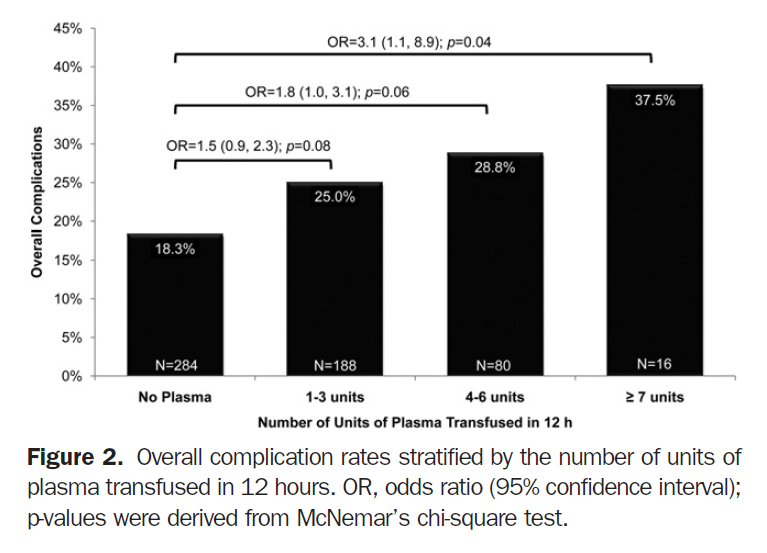
There are two big trauma trials to consider. The PAMPer trial was a pragmatic, multicentre, cluster-randomized trial that randomized prehospital adult trauma patients to either 2 units of plasma or standard crystalloid resuscitation. (Sperry 2018) The primary outcome was 30 day mortality, and was significantly lower in the plasma group (23.2% vs 33.0%; absolute difference 9.8%, 95% CI 18.8-1.0%; p=0.03). I think PAMPer might be the single strongest piece of evidence supporting the concept of balanced transfusion, but it’s not a perfect trial, as you can read in the original blog post.
Although not an exact replication, the RePHILL trial seems to contradict PAMPer. It is another prehospital open label trauma RCT, this time comparing normal saline to a combination of both plasma and packed cells. (Crombie 2022) This was a negative trial, and despite using a ridiculous composite primary outcome, there was clearly no difference in any of the important outcomes, like mortality.
Obviously, the conclusions one can draw from PAMPer and RePHILL are rather limited, because all of these patients would have received very similar treatment once they hit hospital, and those massive transfusions are likely to outweigh the tiny initial management, even if we still believe the first hour is the most important in trauma.
There is a 2012 systematic review that looks at the use of FFP both prophylactically and therapeutically in any situation. (Yang 2012) They only included RCT evidence, which resulted in a total of 80 RCTs being summarized. They conclude that there is “no consistent evidence of significant benefit for prophylactic and therapeutic use across a range of indications evaluated”. This includes no evidence of benefit in liver disease, cardiac surgery, and warfarin reversal. These trials are all small, and relatively low quality, so there is tremendous uncertainty here, but it is important to know that there is no high quality evidence of benefit from FFP transfusion in any medical condition. Lack of evidence is not evidence of absence, but when providing therapies with known harms, we really want to see evidence of benefit rather than relying purely on physiologic rationale.
Another systematic review arrives at the conclusion that plasma use in trauma is associated with a reduction in the risk of mortality. (Murad 2010) However, unlike the Yang systematic review, this review included both RCTs (of which there were none for trauma) and observational data. The study quality was low, and there was evidence of survival bias. The mortality benefit in trauma is based on 10 observational studies. The mortality in the control group in these studies was over 50%, and indicative of selection bias. The same review found no benefit from plasma in surgical patients and no benefit in patients with liver disease. For patients on warfarin, the only RCT had no deaths. There were two chart reviews, one of which demonstrated an association between FFP and improved mortality. Among all the studies, plasma transfusion was associated with a significant increase in the rate of acute lung injury.
The Cochrane review looking at FFP for cardiac or aortic surgery found no evidence of benefit in the 15 RCTs that were identified. (Desborough 2015)
There is a double blind RCT comparing FFP (10-15 ml/kg) to placebo in 90 trauma patients with traumatic CT confirmed intracranial hemorrhage, no known anticoagulation, and a GCS 8 or less. (Etemadrezaie 2007) It is an imperfect study, with imperfect allocation procedures (shuffled sealed envelopes). They report a lot of outcomes and don’t state a primary outcome. They report more patients with delayed traumatic intracerebral hematoma on repeat CT in the FFP group (17% va 0%, p=0.007). Mortality was also higher with FFP (63% vs 35%, p=0.006).
There is another small single center RCT that compared FFP to factor concentrate (primarily fibrinogen), and the trial was stopped early (100 total patients) because of a signal of harm in the FFP group. (Innerhofer 2017)
We know that plasma causes harm. This is discussed more in the section on harms below. There is an interesting propensity-matched study based on 1700 trauma patients who received less than 10 units of packed red blood cells in the first 12 hours of their resuscitation (ie, did not meet the definition of massive transfusion). The use of FFP was associated with an increase in adverse events. (Inaba 2010) There was no difference in mortality or length of stay, but there was a significant increase in adverse events, primarily driven by an increase in ARDS, in the patients who received FFP. This association was dose related. While conclusions from this retrospective data are very limited, it should serve as a caution about overzealous use of plasma, which is problematic given the difficulties in identifying which patients will require massive transfusion.
There is a prospective observational study looking at 1440 critically injured trauma patients, and they also found that early administration of FFP was associated with an increase in multiple organ failure, although confounding (in which sicker patients get earlier FFP) is likely. (Johnson 2010)
When moving beyond empiric management and into laboratory guided transfusion, an INR of 1.8 is probably the best threshold to use, as it may not be possible to get the INR below 1.8 even with large volume transfusions of FFP. (Petrosoniak 2023)
EBM summary: There is surprisingly little data to guide us, considering the prevalence of FFP transfusions in medicine. Although some people might argue that FFP falls into the “parachutes” category of therapies, with obvious benefits based purely on physiology, I think there is enough data (with no clear benefit) to demonstrate that FFP is definitely not a parachute. If we can’t see a clear benefit from FFP with over 80 RCTs done in various settings, it seems unlikely that it is going to be the silver bullet with dramatic benefit when added to massive hemorrhage protocols. Conversely, there is plenty of evidence of harm. My guess, after sorting through this data, is that we are over-using FFP in clinical practice, probably causing harm with current practice, and that future massive hemorrhage protocols will trend towards less FFP, not more.
Practical bottom line: I am cautious whenever prescribing FFP. Although I follow my institutions’ massive hemorrhage protocols, I am very cautious in activating the protocol, for fear of overuse and subsequent harm. I try to focus on PRBC transfusion over FFP throughout most of the early resuscitation.
The role of PCCs
Some have argued to either replace or supplement FFP with prothrombin complex concentrate (PCC). There are many theoretical reasons why this might be beneficial, from the practical difficulties of storing and thawing FFP, to decreased harms from transfusion related lung injury, transfusion related circulatory overload, bacterial contamination, and allergies.
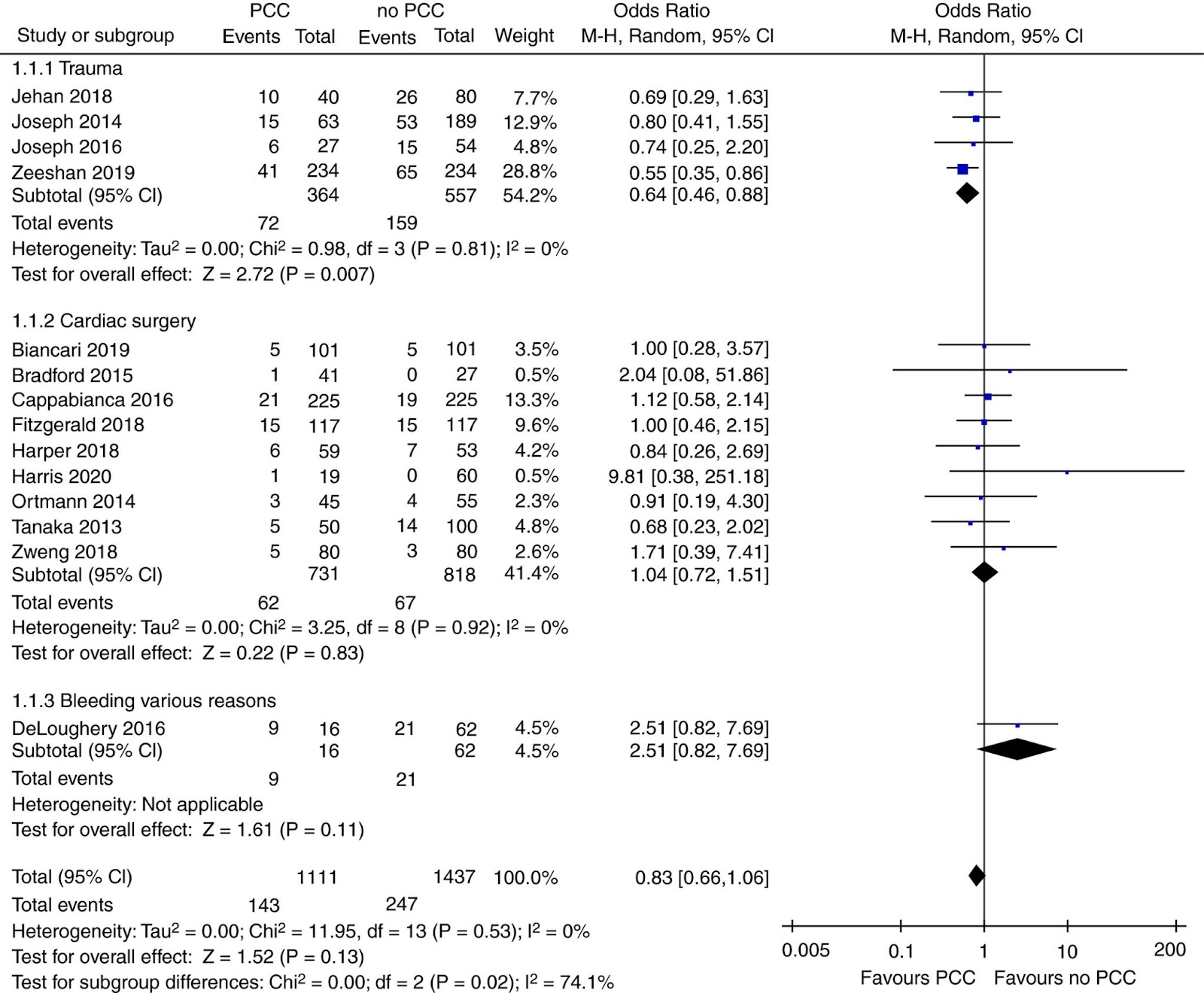
One systematic review looking at any study that compared PCC to placebo, nothing, or usual care (FFP) in bleeding adult patients found 17 studies encompassing 2030 patients, but 15 of them were retrospective. (van den Brink 2020) More than half of the studies were in the setting of cardiothoracic surgery. It was about an even split between 4 and 3 factor PCCs. Overall, there was no association between PCC use and mortality, but the odds ratio would be clinically important if it were statistically significant (OR 0.83; 95% CI 0.66‐1.06; P = 0.13). In the subgroup of trials looking at trauma, there was a statistically significant association with decreased mortality, although this was only seen when PCCs were combined with FFP. The PCC group used less blood products overall (3 fewer units of PRBC in the trauma subgroup), and there is no evidence of thrombotic adverse events. However, all of these numbers need to be taken with a giant grain of salt, considering that we are talking about small observational trials full of confounders.
There is another systematic review that you will see cited, focusing only on the trauma patients, and only on the combination of PCC plus FFP versus FFP alone. (Kao 2021) They state that there is a better survival rate with PCC, but this is based entirely on 3 retrospective studies.
There is a pilot, open-label RCT comparing PCC to FFP in patients who had coagulation factor replacement ordered during cardiac surgery. (Karkouti 2021) There was no statistical difference in this small trial, and there are numerous issues with the open-label design, but outcomes do look somewhat better in the PCC group, with the PCC group getting about 6 total units of blood products after the intervention, as compared to 10 units in the FFP group. It is certainly not enough to base practice on, but it is one of the papers you will see cited by people excited about this direction.
The one big RCT to date is the PROCOAG trial. (Bouzat 2023) This is a multicenter RCT in which 350 adult trauma patients who were at risk for massive transfusion (primarily based on the ABC score) were randomized to either 4 factor PCC or placebo. There was no difference in to primary outcome of total blood product used at 24 hours (absolute difference between groups of 0.2 units). Mortality was unchanged (26% vs 30%). However, thromboembolic events were significantly increased (35% vs 45%, p=0.03). The biggest limitation of this trial might be that only about 25% of patients met the formal definition of massive transfusion (10 units in 24 hours), so this population might be too healthy, which would limit potential benefit from PCC. (Considering that PCC should theoretically be better than FFP, it is possible this trial is another hint that we have been overzealous in our adoption of empiric balanced transfusion.)
Ontario guidelines state that at hospitals that don’t have access to FFP, PCCs are a reasonable alternative, with a suggested dose of 2000 IU. If PCCs are used, they also suggest fibrinogen replacement unless the fibrinogen is known to be greater than 1.5 g/L. (Callum 2019)
EBM summary: The theoretical rationale here is strong, and even non-inferiority might be enough reason to switch to PCC over FFP. However, the data so far is unconvincing. There are hints of potential benefit in incredibly low quality retrospective data, but that is completely over-ruled by the one large RCT to day showing possible harm. Considering that we don’t even know whether empiric FFP is a good idea, we have a long way to go before using PCCs empirically in massive hemorrhage.
Practical bottom line: This is an interesting area for future research, but for now it is not ready for regular clinical use. If FFP is not available, prothrombin complex concentrate (PCC) is a possible alternative.
Platelets
It might have helped to have a medical librarian for this search, because it seems very hard to find studies on platelet transfusion, even when I know they exist. There seems to be very limited information on the use of platelets in the context of massive hemorrhage. Most of the available evidence is from other settings, and so this section is a lot more tangential than the other sections.
Platelet count at hospital admission is inversely correlated with survival in trauma, but unlike the other components of coagulopathy, only a minority of trauma patients have a platelet level below 150 × 109/L at presentation. (Spahn 2019) Like with all blood products, there are many confounders hidden within this association, and it shouldn’t be translated to mean that transfusing platelets is necessarily helpful. Furthermore, platelet levels don’t tend to drop until later in the resuscitation, and therefore you probably have time to wait and guide resuscitation based on labs rather than treating empirically. You can expect to routinely see a platelet count below 50 when approximately two blood volumes have been replaced by fluid or red cell components. (Spahn 2019)
As far as I can tell, both through my own searches and reading through the references in guidelines, I don’t think there are any trials looking at platelet transfusions in isolation in trauma.
The evidence for using platelets prophylactically in patients with hematologic malignancies and thrombocytopenia actually seems pretty good, with 5 RCTs demonstrating a decrease in critical bleeding (OR 0.53, 95% CI 0.32-0.87). (Kumar 2015) Three of these RCTs compared prophylactic to therapeutic transfusion, and prophylactic was better, although at the cost of more total platelets transfused. There was no statistical benefit in terms of mortality, but the trials were small and potentially under-powered, and the odds ratio is on the right side (OR 0.72 95% CI 0.4-1.55).
There are 4 RCTs in the context of cancer based thrombocytopenia comparing the prophylactic transfusion thresholds of 10,000 plts/μL versus 20,000 plts/μL and no differences were seen. (Slichter 2004)
The PATCH trial is a cautionary tale. They randomized 190 patients on antiplatelet therapy with non-traumatic intracerebral hemorrhage and a GCS of at least 8 to standard care or platelet transfusion. (Baharoglu 2016) The platelet transfusion group did worse. The primary outcome was a shift towards death and disability on the modified Rankin scale, and it was worse in the treatment group (OR 1.84, 95% C.I. 1.1-3.08, p=0.02).
When I started this review, the data on performing procedures in patients with thrombocytopenia seemed to be almost entirely observational, and therefore prone to bias. (Kumar 2016) There is no clear benefit from platelet transfusions in the observational data, and the complication rate in the setting of thrombocytopenia seems low, but this data is extremely limited.
However, the PACER trial was published just a few months ago, and appears to demonstrate a benefit from prophylactic platelet transfusions in patients with platelet counts between 10,000 to 50,000 per cubic millimeter when placing central lines. (van Baarle 2023) It is an open label multicenter RCT, in which patients were randomized to receive 1 unit of platelets or no transfusion. No transfusion was “not non-inferior” to transfusion. (In fact, no transfusion was statistically inferior, but people are very bad at describing the results of their non-inferiority trials.)
Platelet levels actually take a long time to drop to dangerous levels, and platelets cause the highest rate of transfusion adverse events. (Petrosoniak 2023; Spahn 2019) Therefore, it might make sense to drop the platelets from the empiric ratio based resuscitation, and wait for lab-guided transfusion in most patients.
EBM summary: Honestly, the evidence for platelet transfusion is better than I thought, given that the only research I had really seen previously was the PATCH trial. However, almost all of the research is in the setting of hematologic malignancies or impaired platelet production, rather than looking at empiric treatment in advance of the development of dilutional coagulopathy from massive transfusion. There is nothing here to convince me that empiric, prophylactic therapy as part of a 1:1:1 balanced transfusion strategy is a great idea.
Practical bottom line: Again, I think it is important to follow institutional protocols when you have a sick patient in front of you, but I don’t feel the least bit concerned that neither of my hospitals stock platelets on site, and there will be a 2 hour delay whenever I order them.
Using whole blood
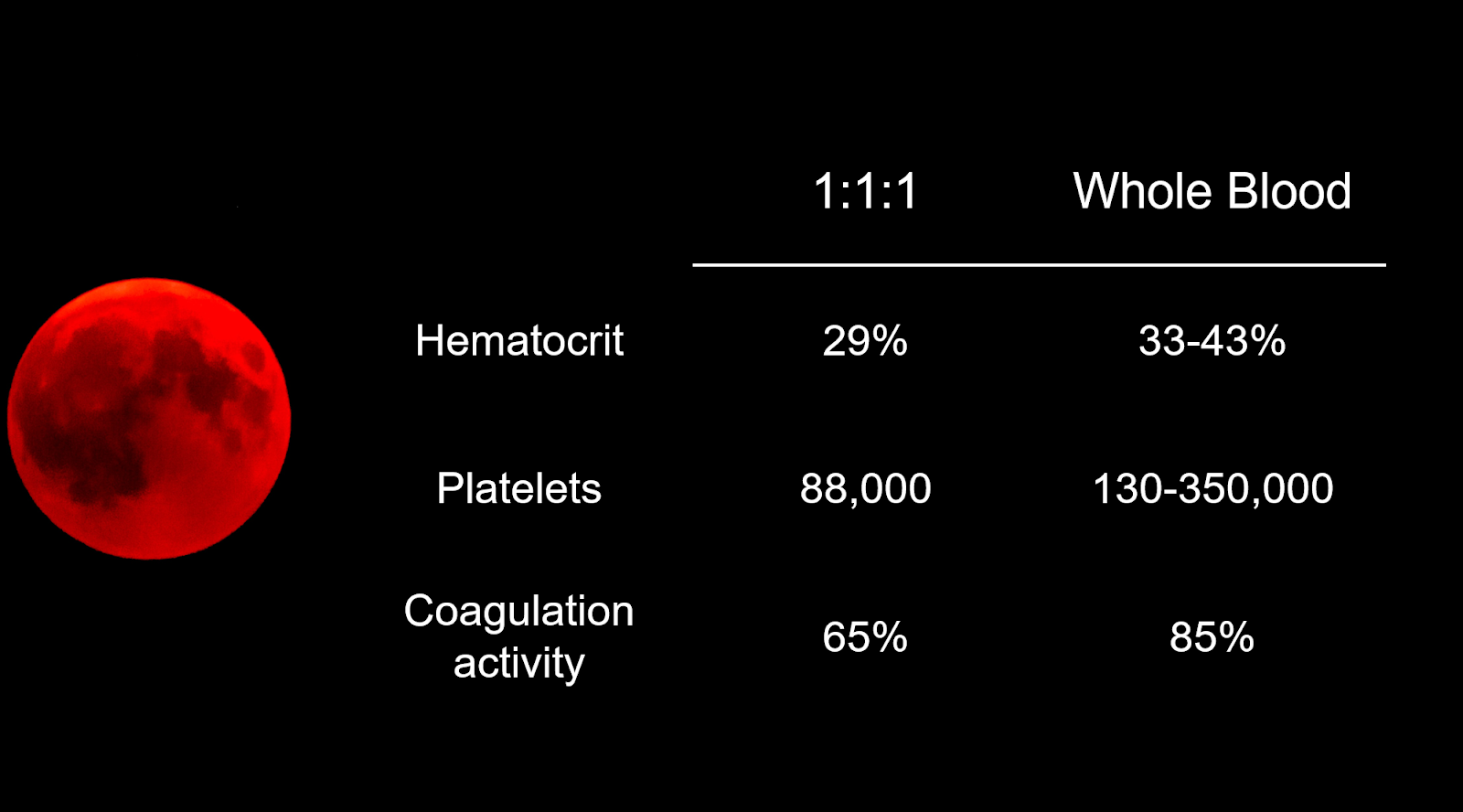
Taking the theory of balanced transfusion one step further, some have argued we should abandon component therapy altogether and just give patients whole blood. In massive transfusion patients, this makes physiologic sense, as we are just replacing what they are losing. The combination of one unit of red blood cells, platelets, and FFP as components results in a 660 mL bolus that has a hematocrit of about 29%, 88,000 platelets and 65% coagulation activity. In contrast, 500 mL of whole blood has a hematocrit of 33-43%, 130-350,000 platelets, and 86% clotting activity. (Spinella 2008) However, as we have said over and over on this blog, physiologic theory doesn’t always translate well into clinical outcomes, and there are potential harms (and added costs) with using whole blood.
In observational data from a convenience sample of military forward surgical teams operating in Afghanistan from 2005 to 2010 encompassing 488 patients, 94 were given fresh whole blood and 394 were not. (Nessen 2013) There was no difference in mortality between the groups (5.3% vs 8.8%). However, the groups were quite different at baseline. After an adjusted analysis, fresh whole blood was associated with decreased mortality. However, there are just too many confounders for this adjusted comparison to be convincing. Fundamentally, whole blood was given in completely different scenarios, and the association with mortality (which doesn’t exist in the raw data) could be the result of the many unseen confounders.
Single center observational data from an American trauma center including a total of 86 patients found no statistical difference between component therapy and whole blood in patients receiving massive transfusion for trauma. (Shea 2020) Again, there is a statistical difference in their adjusted analysis, but the need for adjustment just emphasizes how different these patients were at baseline, and how difficult it is to appropriately adjust. I also find it interesting that despite receiving massive transfusions in the setting of trauma in 2018, less than half of these patients received TXA. I don’t think data like this suggests anything other than the need for a proper trial.
A pilot single-center RCT compared whole blood to standard component therapy in 107 patients with severe trauma and evidence of active bleeding. (Cottom 2013) The primary outcome was blood product use at 24 hours, and was not different. Mortality was a secondary outcome, and also wasn’t different (11% vs 10% at 24 hours). There is a somewhat concerning trend in 30 day mortality, with a 22% mortality rate in the whole blood group and 14% in the component group (p=0.26). This is likely spurious, but certainty doesn’t favour whole blood in the absence of other evidence.
There is a quasi-randomized observational dataset from a single trauma center in which patients were supposed to receive whole blood on odd calendar days and component therapy on even calendar days. (Duchesne 2020) Unfortunately, this quasi-randomization apparently failed miserably, as 70% of patients still received component therapy. There was no statistical difference in mortality, but with only 253 patients, the study may just have been under-powered, and the difference in survival between 22% and 27% certainly would be clinically important. However, this difference is probably not real, as there are plenty of indications of confounders: the whole blood group had a massive transfusion protocol activated much less commonly (26% vs 44%) and had more penetrating trauma.
There is a systematic review and meta-analysis this year that combines 44 observational studies from both the military and civilian literature. (van der Horst 2023) They conclude that the use of whole blood is associated with a decrease in 24 hour mortality (OR 0.72, 95%CI 0.53-0.97), but there was no decrease in late mortality (OR 0.97 95%CI 0.80-1.18). For the reasons discussed above, I don’t think you can trust the association with early mortality, because the groups getting whole blood just aren’t like the control groups. However, even if there was a benefit at 24 hours, if there is no difference in survival to 1 month or hospital discharge, that is not consistent with an overall benefit. I think this hints at an important overall point: it is not good enough to just look at early survival in trauma. We do a lot of things (like transfusing blood products) that can result in significant adverse events. Just keeping a patient alive for 24 hours doesn’t automatically mean that we have done good. You need to look at longer term outcomes to be able to assess the net positives and negatives from our interventions.
One confounding factor to consider is that whole blood is often fresh (given within minutes to hours of being donated in the military setting), whereas component therapy is almost always with stored blood. (Spinella 2008) Older blood has numerous potential problems, including a decrease in oxygen carrying capacity, decrease in coagulation factors, and decrease in platelet function.
Active trials to watch: NCT05634109, NCT04431999, NCT05081063
EBM summary: The evidence is extremely weak, but thus far there is no good evidence of benefit from using whole blood over component therapy. Whole blood is theoretically better than balanced components, so a lack of benefit from whole blood would make me even more skeptical that there is any advantage from the currently suggested empiric 1:1:1 or 1:1:2 balanced transfusion strategies. That being said, this data is just too weak to push the needle very far in either direction.
Practical bottom line: There doesn’t seem to be any reason to be using whole blood outside of a research setting at this time.
Fibrinogen
There are many observational studies (mostly retrospective) that conclude that there is an association between lower fibrinogen levels and increased hemorrhage, with the most common stated thresholds being either 1.5 or 2.0 grams per liter. (Charbit 2007; Ucar 2007; Karkouti 2013; Collins 2014; Bouzat 2018) Although this association makes sense, and the finding seems consistent, the actual evidence is not all that convincing.
There is a single center RCT that compared FFP to factor concentrate (primarily fibrinogen), and the trial was stopped early (100 total patients) because of a signal of harm in the FFP group. (Innerhofer 2017) This could be interpreted as demonstrating harm in the FFP group, or benefit in the fibrinogen group. It is impossible to tell without a true control group.
One study is often cited as showing an association between a fibrinogen below 1.5 g/L and increased mortality. (Bouzat 2018) However, I think we need to be very cautious in that interpretation. First of all, it is only a tiny subset of trauma patients, retrospectively identified: the 366 out of 12,000 severe trauma patients that ultimately needed more than 10 units of PRBCs. Second, the inflection point in their graphs seems to suggest that the risk doesn’t really increase until 1.0 g/L or less, to my eye.
In the context of cardiac surgery, there is an association between fibrinogen levels below 2.0 g/L and large volume (>5 units) transfusion of PRBCs. However, it isn’t clear that this is predictive. They used a postoperative fibrinogen level, so causation could be going in the exact opposite direction – with large volume transfusions lowering fibrinogen levels, rather than low fibrinogen levels predicting or causing large volume transfusions. (Karkouti 2013)
Ultimately, an association between low fibrinogen and bleeding can only get us so far. Considering the biologic role of fibrinogen, it would have been very surprising if these associations didn’t exist. However, that doesn’t mean that giving fibrinogen concentrates will necessarily be helpful, or that the benefit will outweigh possible harms. What we really need are therapeutic trials (RCTs).
It is not an RCT, but there is a propensity matched study based on a German trauma registry that matched 294 patients who had received fibrinogen concentrate to 294 who did not. (Wafaisade 2013) These were all sick (ISS 16 or greater) trauma patients with a trauma associated hemorrhage (TASH) score of 9 or more. The results don’t look great. Some people talk about a 6 hour mortality benefit (11 vs 17%), but overall mortality was not different (28.6% with fibrinogen and 25.5% without, p=0.4). Fibrinogen was associated with a higher rate of multi-organ failure (61% vs 49%, p=0.003) and perhaps a high rate of thromboembolism (7% vs 3%, p=0.06). Of course, these are all associations, and we don’t know why some patients received fibrinogen while others did not.
There is a tiny pilot study in the setting of aortic valve surgery in which 5 patients underwent algorithm guided transfusion intraoperatively, and 10 patients received fibrinogen before starting the algorithm. (Rahe-Meyer 2009) Total blood products transfused were lower in the empiric fibrinogen group, but obviously this is a tiny pilot study that doesn’t really prove anything aside from the fact that a full scale study is warranted. This was followed up with a phase 2, prospective, randomized, double-blind, placebo-controlled in which adult patients undergoing elective aortic replacement surgery were randomized to receive either fibrinogen concentrate or placebo only if clinically relevant bleeding occurred. (Rahe-Meyer 2013) Although they say the study was blinded, they were using ROTEM to guide fibrinogen administration, and a median of 8 doses (8 grams) were given in the treatment group, so it seems like they must have known what they were giving. There was a clinically and statistically significant difference between the two groups in the primary outcome of total blood products received, but seeing as these were given by a ROTEM guided algorithm, I think the result could be biased. There were only 60 patients in the trial, so it is much too small to comment on clinically important outcomes. It is promising, but I think there is a high risk of bias despite the reported double-blind design.
In another placebo controlled RCT from the same group, 152 patients undergoing elective aortic surgery requiring cardiopulmonary bypass who bled at least 60 grams, fibrinogen concentrate (dosed based on FIBTEM maximum clot firmness) was compared to placebo. (Rahe-Meyer 2016) This study demonstrated a statistically significant harm, in that their primary outcome of total blood products transfused was actually increased in the fibrinogen group (5 units versus 3 at 24 hours, p=0.026). Secondary outcomes were similar, including more patients being brought back to the OR for bleeding in the fibrinogen group.
Another very small RCT (20 patients) with imperfect methods (randomization by envelope) compared an empiric 2 gram dose of fibrinogen to nothing (ie, this was open label) in patients undergoing coronary artery bypass whose preoperative fibrinogen level was 3.8 g/L or less.(Karlsson 2009) There was a statistical difference in blood loss (about 280 mL difference between the groups), and no obvious adverse events, but this is a very imperfect 20 patient trial.
There is an RCT comparing an preemptive 2 gram dose of fibrinogen, compared to placebo, in 244 women with postpartum hemorrhage. (Wikkelsø 2015) There was no difference in the primary outcome, with 20% of the fibrinogen group and 22% (p=0.88) of the placebo group receiving blood transfusions in the following 6 weeks (seems like a long time to make your primary outcome). There were also no differences in any of the secondary outcomes.
There is a prospective RCT in cardiac surgery patients with significant postoperative bleeding and laboratory confirmed hypofibrinogenemia comparing fibrinogen concentrates to cryoprecipitate. (Bartoszko 2022) They conclude fibrinogen concentrates are noninferior to cryoprecipitate, in terms of subsequent transfusion requirements. Although that doesn’t help us determine whether these products are needed empirically as part of a massive hemorrhage protocol, it is very useful, as cryoprecipitate is a frozen product that takes time to thaw and has a limited shelf life, and so fibrinogen concentrates are likely to be more pragmatic in the resuscitation setting.
A pilot study from 2 UK trauma centers showed it was feasible to provide cryoprecipitate within 90 minutes to adult trauma patients with active bleeding, and the CRYOSTAT-2 trial is a nearly completed multi-centre, randomised controlled trial by the same team evaluating the effects of early high-dose cryoprecipitate in adult patients with major trauma haemorrhage requiring major haemorrhage protocol (MHP) activation. (Curry 2015)
This conversation is complicated by the TEG and ROTEM, which might be used instead of specific fibrinogen cut-offs, and are discussed below.
If you are like me, you have a hard time keeping the many blood products straight, especially because what is available differs by country. A quick reminder:
Cryoprecipitate a product made from FFP, and contains a subset of the factors. It primarily contains fibrinogen, von Willebrand factor, and factor XIII. It is a multi donor product with no antiviral processing, which is why it is not available in some countries. The usual dose is 5-10 units.
Fibrinogen concentrates are also blood products from pooled donors, which undergo purification, viral inactivation, and removal processes and do not require cross-matching. The usual dose is 1-4 grams.
4 grams of fibrinogen concentrate is approximately equivalent to 10 units of cryoprecipitate, with regards to fibrinogen content.
EBM summary: There are a few small RCTs with promising (but not earth-shattering results), but there are also some negative RCTs. Thus, like with everything else we have discussed today, we are left with a tremendous amount of uncertainty about how to fit fibrinogen into our massive hemorrhage protocols.
Practical bottom line: Anticipate change in the future, as the current evidence is incredibly weak. If the fibrinogen is less than 1.5 grams/L (and perhaps 2.0 in high risk patients), most experts suggest replacement using either cryoprecipitate or fibrinogen concentrates (depending on what is available in your jurisdiction).
Tranexamic acid
I have covered this topic at great length already. Here are some links:
- Does TXA work for everything? For anything?
- PATCH-trauma: Another negative (but complicated) TXA trial
- CRASH 3: TXA is no wonder drug
- TXA in traumatic brain injury – a quick update
- TXA in ICH (TICH-2)
- TXA for SAH: Another swing and a miss for the wonder drug
- 3 misunderstandings about WOMAN (TXA in postpartum hemorrhage)
- TXA for GI bleeds: No benefit (The HALT-IT trial)
- NoPAC: No benefit from TXA in epistaxis
- Nebulized TXA for Hemoptysis (Wand 2018)
EBM summary: Since the CRASH 2 trial, essentially all of the high quality TXA research has been negative. A few of these studies have been spun as positives after primary outcomes were changed, or by focusing on disease specific rather than all cause mortality, but overall the evidence is not very convincing. Harms seem to be relatively low, but RCTs always under-estimate harm, the HALT-IT trial did see a doubling of thromboembolic events, there is a strong association with increased mortality when TXA is given late, and the PATCH-trauma trial raises the concern that improve survival might come with poor neurologic outcomes. Overall, given the ongoing debate despite many massive trials, it seems like TXA has a pretty minimal impact, and at this point it isn’t clear whether that impact is a net positive or negative.
Practical bottom line: I still give TXA within the parameters of CRASH 2, assuming it can be given in the first few hours, but not in any other clinical scenario.
Recombinant factor VII
Factor VII has never been used in any clinical setting I have worked in, so I wasn’t even going to cover it, but I guess a brief mention is warranted.
There is a 2012 Cochrane review that includes 29 RCTs. (Simpson 2012) 16 trials (1361 patients) looked at prophylactic use. There was no mortality benefit (RR 1.04, 95% CI 0.55-1.97). There was a statistical decrease in blood loss (300 mL) and transfusion requirements (260 mL), but they say that is an overestimate because they couldn’t include 4 trials, and all 4 showed no difference. There were 13 trials (2929 patients) looking at therapeutic use, and there were no statistical differences in any of the outcomes. When they pooled all the outcomes together, there was a statistical increase in thromboembolic events (RR 1.45 95% CI 1.02-2.05).
It is the only product discussed here that is specifically recommended against in guidelines. For example the Europeans say, “we do not recommend the use of recombinant activated coagulation factor VII (rFVIIa) as first-line treatment. (Grade 1B)” (Spahn 2019)
EBM summary: Presumably because it was a new product and there was a big potential for profit, this product has the largest number of RCTs by far. (Can we please take the research dollars out of large corporations’ hands already?) I think it is a reasonable reminder that there will always be a tradeoff when messing with the clotting cascade, as there may be a small benefit here, but it appears to be outweighed by harms.
Practical bottom line: I don’t think anyone is using factor VII routinely at this time.
Real-time viscoelastic testing
Theoretically, real time viscoelastic testing provides not just rapid feedback about coagulation, but also specific information about how to manage coagulopathy. The accuracy seems to be good, but not great (Hunt 2015) However, the important question is what clinical impact these tests have.
A Cochrane review from 2016 identified a total of 17 RCTs, encompassing 1493 participants, looking at TEG and ROTEM. (Wikkelsø 2016) Although the quality of the studies was low, there is high risk of bias, and the confidence intervals are huge, the outcomes favour use of TEG and ROTEM. There was a statistical decrease in mortality (7.4% versus 3.9%; risk ratio (RR) 0.52, 95% CI 0.28 to 0.95). Patients in the TEG/ROTEM groups also received significantly less PRBCs, FFP, and platelets.
I find that combination of results fascinating. If real, it is beneficial on both sides: we treat less and we save lives. That is an amazing outcome for viscoelastic testing, but if you think about it, it is a pretty damning conclusion for the currently recommended practice of empiric ratio based balanced transfusion. These results suggest that giving less FFP and less platelets, which is the direct impact of viscoelastic testing, saves lives. That seems to suggest that the push over the last decade to use more FFP and platelets as part of balanced transfusion might actually be causing significant harm. (Or these results are biased, and viscoelastic testing doesn’t help, but you don’t seem to be able to have it both ways.)
Another 2017 systematic review identified 15 RCTs (1238 patients), with a primarily cardiac surgery population, and also concluded that TEG/ROTEM results in less transfusion of PRBCs and FFP, but this time with no difference in mortality. (Fahrendroff 2017) The difference between these two reviews is just the overall power, because the point estimates all look similar.
Another small, single center pseudo-randomized trial (patients assigned by week) compared TEG to standard coagulation assays in the management of 111 trauma patients. (Gonzalez 2016) The primary outcome was mortality, and it was improved in the TEG group (20% vs 36%, p=0.049). The TEG group received a similar amount of PRBCs, but less FFP and platelets. Again, the test itself isn’t saving lives. The only effect it seems to be having is reducing the total amount of FFP and platelets given, and that seems to result in a decrease in mortality, which is pretty damning for the entire concept of 1:1:1 or whole blood transfusion.
The ITACTIC trial was a pragmatic, multi-centre, randomized controlled trial that enrolled 396 adult trauma patients requiring massive hemorrhage protocol, and randomizing them to either viscoelastic testing or conventional lab testing. (Baksaas-Aasen 2021) There were no differences in this trial, either in their primary outcome (a composite of death and ongoing massive hemorrhage) or the secondary outcomes. The big limitation with this study was that, despite suspecting the need for massive transfusion, the majority of patients didn’t actually receive it. In other words, they might have diluted out the effect by including patients who were too healthy. (You can read more about this study on The Bottom line.)
EBM summary: The available data is still relatively limited and low quality. There was a consistent trend demonstrating benefit in the early trials, but the largest trial (ITACTIC) was clearly negative. This is a pretty common trend in medicine, influenced by a combination of bias in the smaller trials (especially as all these trials are necessarily open label) and publication bias. I think the best guess is probably that we won’t see a benefit in the long run, however, with multiple small trials demonstrating a mortality benefit, I can understand why trauma centers are adopting this technology while we wait for more research.
In terms of the larger question that started this review, whether balanced transfusion is beneficial, I think this data might be the most damning available. The direct impact of TEG/ROTEM seems to be to decrease FFP and platelet use, and that might decrease mortality. These results seem to say that giving less FFP saves lives. In other words, the overzealous adoption of balanced empiric transfusion as part of massive hemorrhage protocols based on inadequate evidence might be doing significant harm.
Practical bottom line: Despite the remaining uncertainty, I think it is reasonable to be using this technology right now, but we should also be prepared for future trials to tell us this was a wasted investment. Whether it makes sense for any individual hospital to purchase this technology will depend on how often they are activating a massive hemorrhage protocol.
Calcium
Hypocalcemia is common in sick trauma patients. More than half of patients arriving at the ED are already hypocalcemic, even before receiving treatment. (Webster 2016; Magnotti 2011) Transfusion then makes the issue worse, both through dilution, and through the effects of citrate. (Giancarelli 2016) Hypocalcemia in trauma is associated with increased total transfusions and increased mortality. (Magnotti 2011; Giancarelli 2016)
However, we need to be very careful about these associations. Almost all of these trials are retrospective. Causation goes both ways (transfusions cause hypocalcemia). Bleeding itself causes hypocalcemia, but that doesn’t mean that the calcium is the issue (the bleeding is). The conclusion of this systematic review provides a reasonable summary: “Hypocalcemia is a common finding in shocked trauma patients. While an association between admission ionized hypocalcemia and mortality, blood transfusion requirements, and coagulopathy has been identified, further prospective trials are essential to corroborating this association.” (Vasudeva 2021)
Unlike some of the other topics covered here, the harms from empiric calcium are incredibly low. Therefore, although I am concerned that we have been overzealous in our empiric treatment with FFP and platelets, I think empiric therapy with calcium makes more sense (while we wait for proper studies confirming benefit).
There may be another benefit of including empiric calcium in a massive hemorrhage protocol: transfusions cause hyperkalemia. For a variety of reasons, potassium which starts inside red blood cells leaks and ends up outside of cells, and so each unit of PRBCs you transfuse can have as much as 80 mEq of potassium. (I find that number astounding, considering that for potassium repletion we are limited to 10-40 mEq per hour, but we are often transfusing 10 times that in an hour). Considering the relatively high risk of hyperkalemia, treatment with calcium doesn’t seem like that bad an idea. (Of course, that statement is pure physiologic reasoning, and not strong evidence.)
EBM summary: There is a strong physiologic rationale, in that we know calcium is important in clotting and cardiovascular function, and that calcium levels are decreased by both bleeding and transfusions. There is also a consistent association between hypocalcemia and bad outcomes in bleeding patients.
However, the observational data is at very high risk of bias. (Bleeding and transfusions both lower calcium. Low calcium is therefore obviously associated with the need for transfusion and bad outcomes. However, that doesn’t mean hypocalcemia is the cause, nor that treating the calcium is the solution.) Thus, we need to acknowledge the tremendous uncertainty that remains, and the fact that any action we take is based almost entirely on physiologic reasoning (which is an important part of science, but has a really bad track record in medicine.)
On the other hand, we know that giving calcium is relatively safe. (Although we shouldn’t be too cavalier in such statements after empiric calcium seemed to increase mortality in the COCA trial.) We should not be at all surprised if future RCTs show no benefit, or even harm.
Practical bottom line: At a minimum, we should be checking ionized calcium levels in bleeding patients, and replacing as needed. However, I think that empiric therapy probably makes sense, and I aim to give a gram of calcium chloride (or equivalent) for every 2 units of blood.
Avoiding hypothermia
Long taught as a central component of traumatic coagulopathy, the evidence around hypothermia is as weak as it is for almost everything related to massive transfusion. There is observational data (mostly chart review) that demonstrates that many trauma patients never have their temperature recorded, hypothermia is common among those that do, and that mortality is associated both with hypothermia and with not checking the temperature at all. (Jurkovich 1987; Rubiano 2012; Reynolds 2012; Alam 2018; Lester 2019) There is also data from the surgical literature demonstrating an association between hypothermia in the OR and both blood loss and transfusion requirements. (Rajagopalan 2008)
However, similar to everything else discussed, the logic here is circular, and confounders abound. If a nurse doesn’t have time to complete even a basic set of vitals, which they do on every single patient (even ankle sprains), you can be sure that patient is much sicker than the average patient. Similarly, in a relatively stable trauma patient, we are very good about getting them covered with warm blankets as soon as possible. Which patients can’t be covered? The ones that are so sick that there are multiple ongoing procedures. It is very hard to treat hypothermia while simultaneously performing a thoracotomy, but it would be spurious to conclude that the hypothermia killed the patient.
Much like the calcium conversation, the physiologic reasoning here is sound (assuming you reject the idea that ‘therapeutic hypothermia’ saves brains, which would complicate the physiologic reasoning significantly). Similarly, there is essentially no harm to keeping a patient warm and comfortable (unless your warming efforts hamper more important resuscitative efforts). However, I am not at all convinced by the data that this association is real (or anything more than a marker of underlying sickness in the hypothermic patients.)
This feels like the association between time to antibiotics and death in sepsis. No one is trying to delay antibiotics, and the association makes enough sense that we are never going to test it in an RCT, but it would be stupid to create core measures around time to antibiotics, because the evidence is not strong enough to support them. Similarly, we are always going to do everything we can to keep patients warm and comfortable, but I think we want to be careful about being overly dogmatic, because this evidence is nowhere strong enough to support dogma. (Or, perhaps, the evidence is exactly weak enough to support dogma?)
EBM summary: You can copy and paste the calcium comments here. There is an association and a strong physiologic rationale, and almost no harm to keeping people warm, but we need to acknowledge that there is room for tremendous bias in this observational data, and so the evidence that temperature matters is extremely weak. I doubt we will ever get better data on this topic, and I also doubt that it matters that much. Honestly, science is probably of secondary importance here. It is basic human courtesy to keep our patients comfortably warm in the trauma bay.
Practical bottom line: Don’t let concerns about hypothermia interfere with core resuscitation, but once the essential procedures are complete and time allows make sure you are keeping your patient warm.
Stopping the protocol
Considering the significant resources that go into running a massive hemorrhage protocol, it is important to consider triggers for stoppage. As far as I can tell, there is no research to guide us, and so this will just be left to clinical judgment (improving vital signs and control of hemorrhage). However, hospital protocols probably need to think clearly about human factor issues, as I have been involved in numerous resuscitations in which the “code transfusion” was left active far longer than necessary. We don’t see the consequences of that in the emergency department (or OR or whatever), but there are often significant implications for other areas of the hospital. Including some kind of automatic trigger to ask the clinical lead whether the code still needs to be active makes sense.
Harms
Data looking at stable patients does not apply when considering massive hemorrhage protocols. That being said, there is a large amount of high quality data that tells us that restrictive blood transfusion using lower hemoglobin targets is better than liberal targets. (Eg, Herbert 1999, Villaneuva 2013) I think this data is a really important reminder of the harms of blood transfusion, and we know that platelets and FFP are associated with more harms than PRBCs. These harms are an important consideration when designing massive hemorrhage protocols.
Transfusion related acute lung injury (TRALI) is related to the plasma component of blood, and is therefore only a risk with FFP, platelets, or whole blood. The risk is approximately 1 case per 5,000 units transfused, although the rate has been decreased by eliminating female plasma from the donor pool. On the other hand, the risk is higher in patients in shock, and so is an important consideration in empiric massive hemorrhage protocols. (Sayah 2012)
When thinking about balanced transfusion and massive hemorrhage, it is important to consider indication creep. Baseline practice was a relatively low rate of usage of both FFP and platelets, as compared to PRBC, but as time has passed and the 1:1:1 strategy has been widely promoted, clinicians are seemingly much more likely to pull the trigger on early transfusion of both platelets and FFP. As mentioned in the FFP section, there is a propensity matched study looking at 1700 trauma patients who received less than 10 units of PRBC, and the use of FFP was associated with a significant increase in adverse events. (Inaba 2010) While this is an association only, we know that FFP has a higher rate of adverse events that packed red cells, and so indication creep could cause significant harm, which is especially concerning if there is no proven benefit to a 1:1:1 strategy.
The empiric balanced transfusion approach almost certainly also increases costs and wasted blood products, which would clearly be warranted if there was evidence of benefit, but thus far that evidence is severely lacking. (Kelly 2013)
Some general evidence based medicine comments
There are many different definitions of “massive transfusion” that exist in the literature, from 10 units of PRBC is 24 hours, to 6 units in 6 hours or 5 units in 4 hours. (Flint 2018) I don’t think any of these really help clinically, and are mostly used for defining patients retrospectively. From an EBM standpoint, that means that the patients included in observational trials might not look the same as the patients you think of as critical bleeding patients. This is not a problem in RCTs, which need to use inclusion criteria closer to what we use clinically, but affects a lot of the observational research, because those studies tend to identify these patients retrospectively.
Survivorship bias is a recurrent issue in this literature. Critically ill patients die, and they often die before they can receive all the intended therapies. ‘Healthier’ patients live longer, receiving more therapy. In observational studies, this can make it look like the therapies are increasing survival, when in fact the exact opposite is true. Patients are just surviving long enough to get more therapy (which may not be helpful).
A common complaint about “EBM folks” is that we discount anything that isn’t an RCT. I don’t think that is true. Science is about embracing all forms of data, but also being acutely aware of the limitations of that data. I believe smoking causes cancer, despite only having observational data. Let me be very clear: the observational data we have for these topics is categorically unlike the smoking data. When using observational data to infer causality, you want the association to be strong, to be consistent across all available research, for the association to be specifically between the one cause and effect your are looking at, to be appropriately timed (the cause should come before the effect), to demonstrate a dose/response relationship, to be plausible, and to be coherent across different forms of evidence. If possible, you would also like to see experimental evidence, and consider analogies to other similar factors with known outcomes. (These are known as the Hill criteria). (Fedak 2015) For the most part, despite reasonable physiologic rationale, the observational data reviewed here is has had small effects, inconsistent results, and there are many sources of bias that have not been accounted for. (Really, even temporality is questionable in some of this data. If patients become hypothermic after receiving a large volume transfusion, you can’t really blame hypothermia as the cause of the large volume transfusion.)
Overall summary
From the standpoint of evidence based medicine, I think the only conclusion is uncertainty. That frustrates some people, but I think emphasizing the uncertainty in our current protocols will make it much easier to change practice in the future, and we should expect significant practice change in the area of massive transfusion, as the available data suggests that future research will likely overrule many areas of current practice.
From a pure clinical stand point, hopefully my “First 10 approach to massive hemorrhage” will be posted soon after this literature review (but I am busy, so who knows).
Other FOAMed
IBCC: Massive Transfusion Protocol (MTP)
Emergency Medicine Cases Episode 152: The 7 Ts of Massive Hemorrhage Protocols
LITFL: Massive Transfusion Protocol
EMCrit 298 – Calcium in Exsanguinating Patients with Ricky Ditzel and Jeffrey Siegler
EMCrit 197 – The Logistics of the Administration of Massive Transfusion
EMCrit 071 – Critical Questions on Massive Transfusion Protocols with Kenji Inaba
EMCrit 144 – The PROPPR trial with John Holcomb
References
Alam A, Olarte R, Callum J, Fatahi A, Nascimento B, Laflamme C, Cohen R, Nathens AB, Tien H. Hypothermia indices among severely injured trauma patients undergoing urgent surgery: A single-centred retrospective quality review and analysis. Injury. 2018 Jan;49(1):117-123. doi: 10.1016/j.injury.2017.11.028. Epub 2017 Nov 23. PMID: 29183635
Baharoglu MI, Cordonnier C, Al-Shahi Salman R. Platelet transfusion versus standard care after acute stroke due to spontaneous cerebral haemorrhage associated with antiplatelet therapy (PATCH): a randomised, open-label, phase 3 trial. Lancet (London, England). 387(10038):2605-13. 2016. PMID 27178479
Baksaas-Aasen K, Gall LS, Stensballe J, Juffermans NP, Curry N, Maegele M, Brooks A, Rourke C, Gillespie S, Murphy J, Maroni R, Vulliamy P, Henriksen HH, Pedersen KH, Kolstadbraaten KM, Wirtz MR, Kleinveld DJB, Schäfer N, Chinna S, Davenport RA, Naess PA, Goslings JC, Eaglestone S, Stanworth S, Johansson PI, Gaarder C, Brohi K. Viscoelastic haemostatic assay augmented protocols for major trauma haemorrhage (ITACTIC): a randomized, controlled trial. Intensive Care Med. 2021 Jan;47(1):49-59. doi: 10.1007/s00134-020-06266-1. Epub 2020 Oct 13. PMID: 33048195
Bartoszko J, Martinez-Perez S, Callum J, Karkouti K; FIBRES Study Investigators. Impact of cardiopulmonary bypass duration on efficacy of fibrinogen replacement with cryoprecipitate compared with fibrinogen concentrate: a post hoc analysis of the Fibrinogen Replenishment in Surgery (FIBRES) randomised controlled trial. Br J Anaesth. 2022 Sep;129(3):294-307. doi: 10.1016/j.bja.2022.05.012. Epub 2022 Jun 28. PMID: 35773027
Bouzat P, Ageron FX, Charbit J, Bobbia X, Deras P, Nugues JBD, Escudier E, Marcotte G, Leone M, David JS. Modelling the association between fibrinogen concentration on admission and mortality in patients with massive transfusion after severe trauma: an analysis of a large regional database. Scand J Trauma Resusc Emerg Med. 2018 Jul 9;26(1):55. doi: 10.1186/s13049-018-0523-0. PMID: 29986757
Bouzat P, Charbit J, Abback PS, Huet-Garrigue D, Delhaye N, Leone M, Marcotte G, David JS, Levrat A, Asehnoune K, Pottecher J, Duranteau J, Courvalin E, Adolle A, Sourd D, Bosson JL, Riou B, Gauss T, Payen JF; PROCOAG Study Group. Efficacy and Safety of Early Administration of 4-Factor Prothrombin Complex Concentrate in Patients With Trauma at Risk of Massive Transfusion: The PROCOAG Randomized Clinical Trial. JAMA. 2023 Apr 25;329(16):1367-1375. doi: 10.1001/jama.2023.4080. PMID: 36942533
Brockamp T, Nienaber U, Mutschler M, Wafaisade A, Peiniger S, Lefering R, Bouillon B, Maegele M; TraumaRegister DGU. Predicting on-going hemorrhage and transfusion requirement after severe trauma: a validation of six scoring systems and algorithms on the TraumaRegister DGU. Crit Care. 2012 Jul 20;16(4):R129. doi: 10.1186/cc11432. PMID: 22818020
Callum JL, Yeh CH, Petrosoniak A, McVey MJ, Cope S, Thompson T, Chin V, Karkouti K, Nathens AB, Murto K, Beno S, Pendergrast J, McDonald A, MacDonald R, Adhikari NKJ, Alam A, Arnold D, Barratt L, Beckett A, Brenneman S, Chaudhry HR, Collins A, Harvey M, Lampron J, Margarido C, McFarlan A, Nascimento B, Owens W, Pai M, Rizoli S, Ruijs T, Skeate R, Skelton T, Sholzberg M, Syer K, Viveiros JL, Theriault J, Tinmouth A, Van Heest R, White S, Zeller M, Pavenski K. A regional massive hemorrhage protocol developed through a modified Delphi technique. CMAJ Open. 2019 Sep 3;7(3):E546-E561. doi: 10.9778/cmajo.20190042. PMID: 31484650 Full guidelines here
Charbit B, Mandelbrot L, Samain E, Baron G, Haddaoui B, Keita H, Sibony O, Mahieu-Caputo D, Hurtaud-Roux MF, Huisse MG, Denninger MH, de Prost D; PPH Study Group. The decrease of fibrinogen is an early predictor of the severity of postpartum hemorrhage. J Thromb Haemost. 2007 Feb;5(2):266-73. doi: 10.1111/j.1538-7836.2007.02297.x. Epub 2006 Nov 6. PMID: 17087729
Collins PW, Lilley G, Bruynseels D, Laurent DB, Cannings-John R, Precious E, Hamlyn V, Sanders J, Alikhan R, Rayment R, Rees A, Kaye A, Hall JE, Paranjothy S, Weeks A, Collis RE. Fibrin-based clot formation as an early and rapid biomarker for progression of postpartum hemorrhage: a prospective study. Blood. 2014 Sep 11;124(11):1727-36. doi: 10.1182/blood-2014-04-567891. Epub 2014 Jul 14. PMID: 25024304
Cotton BA, Dossett LA, Haut ER, Shafi S, Nunez TC, Au BK, Zaydfudim V, Johnston M, Arbogast P, Young PP. Multicenter validation of a simplified score to predict massive transfusion in trauma. J Trauma. 2010 Jul;69 Suppl 1:S33-9. doi: 10.1097/TA.0b013e3181e42411. PMID: 20622617
Cotton BA, Podbielski J, Camp E, Welch T, del Junco D, Bai Y, Hobbs R, Scroggins J, Hartwell B, Kozar RA, Wade CE, Holcomb JB; Early Whole Blood Investigators. A randomized controlled pilot trial of modified whole blood versus component therapy in severely injured patients requiring large volume transfusions. Ann Surg. 2013 Oct;258(4):527-32; discussion 532-3. doi: 10.1097/SLA.0b013e3182a4ffa0. Erratum in: Ann Surg. 2014 Jul;260(1):178. PMID: 23979267
Crombie N, Doughty HA, Bishop JRB, Desai A, Dixon EF, Hancox JM, Herbert MJ, Leech C, Lewis SJ, Nash MR, Naumann DN, Slinn G, Smith H, Smith IM, Wale RK, Wilson A, Ives N, Perkins GD; RePHILL collaborative group. Resuscitation with blood products in patients with trauma-related haemorrhagic shock receiving prehospital care (RePHILL): a multicentre, open-label, randomised, controlled, phase 3 trial. Lancet Haematol. 2022 Apr;9(4):e250-e261. doi: 10.1016/S2352-3026(22)00040-0. PMID: 3527180
Curry N, Rourke C, Davenport R, Beer S, Pankhurst L, Deary A, Thomas H, Llewelyn C, Green L, Doughty H, Nordmann G, Brohi K, Stanworth S. Early cryoprecipitate for major haemorrhage in trauma: a randomised controlled feasibility trial. Br J Anaesth. 2015 Jul;115(1):76-83. doi: 10.1093/bja/aev134. Epub 2015 May 19. PMID: 25991760
Desborough MJR, Sandu R, Brunskill SJ, Doree C, Trivella M, Montedori A, Abraha I, Stanworth SJ. Fresh frozen plasma for cardiovascular surgery. Cochrane Database of Systematic Reviews 2015, Issue 7. Art. No.: CD007614. DOI: 10.1002/14651858.CD007614.pub2.
Duchesne J, Smith A, Lawicki S, Hunt J, Houghton A, Taghavi S, Schroll R, Jackson-Weaver O, Guidry C, Tatum D. Single Institution Trial Comparing Whole Blood vs Balanced Component Therapy: 50 Years Later. J Am Coll Surg. 2021 Apr;232(4):433-442. doi: 10.1016/j.jamcollsurg.2020.12.006. Epub 2020 Dec 19. PMID: 33348017
Etemadrezaie H, Baharvahdat H, Shariati Z, Lari SM, Shakeri MT, Ganjeifar B. The effect of fresh frozen plasma in severe closed head injury. Clin Neurol Neurosurg. 2007 Feb;109(2):166-71. doi: 10.1016/j.clineuro.2006.09.001. Epub 2006 Oct 9. PMID: 17029771
Fahrendorff M, Oliveri RS, Johansson PI. The use of viscoelastic haemostatic assays in goal-directing treatment with allogeneic blood products – A systematic review and meta-analysis. Scand J Trauma Resusc Emerg Med. 2017 Apr 13;25(1):39. doi: 10.1186/s13049-017-0378-9. PMID: 28403868
Fedak KM, Bernal A, Capshaw ZA, Gross S. Applying the Bradford Hill criteria in the 21st century: how data integration has changed causal inference in molecular epidemiology. Emerg Themes Epidemiol. 2015 Sep 30;12:14. doi: 10.1186/s12982-015-0037-4. PMID: 26425136
Flint AWJ, McQuilten ZK, Wood EM. Massive transfusions for critical bleeding: is everything old new again? Transfus Med. 2018 Apr;28(2):140-149. doi: 10.1111/tme.12524. Epub 2018 Apr 1. PMID: 29607593
Giancarelli A, Birrer KL, Alban RF, Hobbs BP, Liu-DeRyke X. Hypocalcemia in trauma patients receiving massive transfusion. J Surg Res. 2016 May 1;202(1):182-7. doi: 10.1016/j.jss.2015.12.036. Epub 2015 Dec 30. PMID: 27083965
Gonzalez E, Moore EE, Moore HB, Chapman MP, Chin TL, Ghasabyan A, Wohlauer MV, Barnett CC, Bensard DD, Biffl WL, Burlew CC, Johnson JL, Pieracci FM, Jurkovich GJ, Banerjee A, Silliman CC, Sauaia A. Goal-directed Hemostatic Resuscitation of Trauma-induced Coagulopathy: A Pragmatic Randomized Clinical Trial Comparing a Viscoelastic Assay to Conventional Coagulation Assays. Ann Surg. 2016 Jun;263(6):1051-9. doi: 10.1097/SLA.0000000000001608. PMID: 26720428
Hanna K, Harris C, Trust MD, Bernard A, Brown C, Hamidi M, Joseph B. Multicenter Validation of the Revised Assessment of Bleeding and Transfusion (RABT) Score for Predicting Massive Transfusion. World J Surg. 2020 Jun;44(6):1807-1816. doi: 10.1007/s00268-020-05394-5. PMID: 32006133
Hébert PC, Wells G, Blajchman MA, Marshall J, Martin C, Pagliarello G, Tweeddale M, Schweitzer I, Yetisir E. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med. 1999 Feb 11;340(6):409-17. doi: 10.1056/NEJM199902113400601. Erratum in: N Engl J Med 1999 Apr 1;340(13):1056. PMID: 9971864
Hunt H, Stanworth S, Curry N, Woolley T, Cooper C, Ukoumunne O, Zhelev Z, Hyde C. Thromboelastography (TEG) and rotational thromboelastometry (ROTEM) for trauma induced coagulopathy in adult trauma patients with bleeding. Cochrane Database Syst Rev. 2015 Feb 16;2015(2):CD010438. doi: 10.1002/14651858.CD010438.pub2. PMID: 25686465
Inaba K, Branco BC, Rhee P, Blackbourne LH, Holcomb JB, Teixeira PG, Shulman I, Nelson J, Demetriades D. Impact of plasma transfusion in trauma patients who do not require massive transfusion. J Am Coll Surg. 2010 Jun;210(6):957-65. doi: 10.1016/j.jamcollsurg.2010.01.031. Epub 2010 Apr 28. PMID: 20510805
Innerhofer P, Fries D, Mittermayr M, Innerhofer N, von Langen D, Hell T, Gruber G, Schmid S, Friesenecker B, Lorenz IH, Ströhle M, Rastner V, Trübsbach S, Raab H, Treml B, Wally D, Treichl B, Mayr A, Kranewitter C, Oswald E. Reversal of trauma-induced coagulopathy using first-line coagulation factor concentrates or fresh frozen plasma (RETIC): a single-centre, parallel-group, open-label, randomised trial. Lancet Haematol. 2017 Jun;4(6):e258-e271. doi: 10.1016/S2352-3026(17)30077-7. Epub 2017 Apr 28. Erratum in: Lancet Haematol. 2017 Jun;4(6):e257. PMID: 28457980
Johnson JL, Moore EE, Kashuk JL, Banerjee A, Cothren CC, Biffl WL, Sauaia A. Effect of blood products transfusion on the development of postinjury multiple organ failure. Arch Surg. 2010 Oct;145(10):973-7. doi: 10.1001/archsurg.2010.216. PMID: 20956766
Jurkovich GJ, Greiser WB, Luterman A, Curreri PW. Hypothermia in trauma victims: an ominous predictor of survival. J Trauma. 1987 Sep;27(9):1019-24. PMID: 3656464
Kao TW, Lee YC, Chang HT. Prothrombin Complex Concentrate for Trauma Induced Coagulopathy: A Systematic Review and Meta-Analysis. J Acute Med. 2021 Sep 1;11(3):81-89. doi: 10.6705/j.jacme.202109_11(3).0001. PMID: 34595091
Karkouti K, Callum J, Crowther MA, McCluskey SA, Pendergrast J, Tait G, Yau TM, Beattie WS. The relationship between fibrinogen levels after cardiopulmonary bypass and large volume red cell transfusion in cardiac surgery: an observational study. Anesth Analg. 2013 Jul;117(1):14-22. doi: 10.1213/ANE.0b013e318292efa4. Epub 2013 May 17. PMID: 23687229
Karlsson M, Ternström L, Hyllner M, Baghaei F, Flinck A, Skrtic S, Jeppsson A. Prophylactic fibrinogen infusion reduces bleeding after coronary artery bypass surgery. A prospective randomised pilot study. Thromb Haemost. 2009 Jul;102(1):137-44. doi: 10.1160/TH08-09-0587. PMID: 19572078
Karkouti K, Bartoszko J, Grewal D, Bingley C, Armali C, Carroll J, Hucke HP, Kron A, McCluskey SA, Rao V, Callum J. Comparison of 4-Factor Prothrombin Complex Concentrate With Frozen Plasma for Management of Hemorrhage During and After Cardiac Surgery: A Randomized Pilot Trial. JAMA Netw Open. 2021 Apr 1;4(4):e213936. doi: 10.1001/jamanetworkopen.2021.3936. PMID: 33792729
Kelly JM, Callum JL, Rizoli SB. 1:1:1 – Warranted or wasteful? Even where appropriate, high ratio transfusion protocols are costly: early transition to individualized care benefits patients and transfusion services. Expert Rev Hematol. 2013 Dec;6(6):631-3. doi: 10.1586/17474086.2013.859520. PMID: 24219547
Kumar A, Mhaskar R, Grossman BJ, Kaufman RM, Tobian AA, Kleinman S, Gernsheimer T, Tinmouth AT, Djulbegovic B; AABB Platelet Transfusion Guidelines Panel. Platelet transfusion: a systematic review of the clinical evidence. Transfusion. 2015 May;55(5):1116-27; quiz 1115. doi: 10.1111/trf.12943. Epub 2014 Nov 12. PMID: 25387589
Lester ELW, Fox EE, Holcomb JB, Brasel KJ, Bulger EM, Cohen MJ, Cotton BA, Fabian TC, Kerby JD, OʼKeefe T, Rizoli SB, Scalea TM, Schreiber MA, Inaba K; PROPPR study group. The impact of hypothermia on outcomes in massively transfused patients. J Trauma Acute Care Surg. 2019 Mar;86(3):458-463. doi: 10.1097/TA.0000000000002144. PMID: 30444856
Magnotti LJ, Bradburn EH, Webb DL, Berry SD, Fischer PE, Zarzaur BL, Schroeppel TJ, Fabian TC, Croce MA. Admission ionized calcium levels predict the need for multiple transfusions: a prospective study of 591 critically ill trauma patients. J Trauma. 2011 Feb;70(2):391-5; discussion 395-7. doi: 10.1097/TA.0b013e31820b5d98. PMID: 21307739
Maegele M, Lefering R, Wafaisade A, Theodorou P, Wutzler S, Fischer P, Bouillon B, Paffrath T; Trauma Registry of Deutsche Gesellschaft für Unfallchirurgie (TR-DGU). Revalidation and update of the TASH-Score: a scoring system to predict the probability for massive transfusion as a surrogate for life-threatening haemorrhage after severe injury. Vox Sang. 2011 Feb;100(2):231-8. doi: 10.1111/j.1423-0410.2010.01387.x. Epub 2010 Aug 24. PMID: 20735809
McQuilten ZK, Crighton G, Brunskill S, Morison JK, Richter TH, Waters N, Murphy MF, Wood EM. Optimal Dose, Timing and Ratio of Blood Products in Massive Transfusion: Results from a Systematic Review. Transfus Med Rev. 2018 Jan;32(1):6-15. doi: 10.1016/j.tmrv.2017.06.003. Epub 2017 Jul 6. PMID: 28803752
Murdock AD, Berséus O, Hervig T, Strandenes G, Lunde TH. Whole blood: the future of traumatic hemorrhagic shock resuscitation. Shock. 2014 May;41 Suppl 1:62-9. doi: 10.1097/SHK.0000000000000134. PMID: 24662782
Murad MH, Stubbs JR, Gandhi MJ, Wang AT, Paul A, Erwin PJ, Montori VM, Roback JD. The effect of plasma transfusion on morbidity and mortality: a systematic review and meta-analysis. Transfusion. 2010 Jun;50(6):1370-83. doi: 10.1111/j.1537-2995.2010.02630.x. Epub 2010 Mar 19. PMID: 20345563
Nascimento B, Callum J, Tien H, Rubenfeld G, Pinto R, Lin Y, Rizoli S. Effect of a fixed-ratio (1:1:1) transfusion protocol versus laboratory-results-guided transfusion in patients with severe trauma: a randomized feasibility trial. CMAJ. 2013 Sep 3;185(12):E583-9. doi: 10.1503/cmaj.121986. Epub 2013 Jul 15. PMID: 23857856
Nessen SC, Eastridge BJ, Cronk D, Craig RM, Berséus O, Ellison R, Remick K, Seery J, Shah A, Spinella PC. Fresh whole blood use by forward surgical teams in Afghanistan is associated with improved survival compared to component therapy without platelets. Transfusion. 2013 Jan;53 Suppl 1:107S-113S. doi: 10.1111/trf.12044. PMID: 23301962
Nunez TC, Voskresensky IV, Dossett LA, Shinall R, Dutton WD, Cotton BA. Early prediction of massive transfusion in trauma: simple as ABC (assessment of blood consumption)? J Trauma. 2009 Feb;66(2):346-52. doi: 10.1097/TA.0b013e3181961c35. PMID: 19204506
Petrosoniak A, Pavenski K, da Luz LT, Callum J. Massive Hemorrhage Protocol: A Practical Approach to the Bleeding Trauma Patient. Emerg Med Clin North Am. 2023 Feb;41(1):51-69. doi: 10.1016/j.emc.2022.09.010. PMID: 36424044
Prat NJ, Meyer AD, Ingalls NK, Trichereau J, DuBose JJ, Cap AP. Rotational thromboelastometry significantly optimizes transfusion practices for damage control resuscitation in combat casualties. J Trauma Acute Care Surg. 2017 Sep;83(3):373-380. doi: 10.1097/TA.0000000000001568. PMID: 28846577
Rahe-Meyer N, Pichlmaier M, Haverich A, Solomon C, Winterhalter M, Piepenbrock S, Tanaka KA. Bleeding management with fibrinogen concentrate targeting a high-normal plasma fibrinogen level: a pilot study. Br J Anaesth. 2009 Jun;102(6):785-92. doi: 10.1093/bja/aep089. Epub 2009 May 2. PMID: 19411671
Rahe-Meyer N, Solomon C, Hanke A, Schmidt DS, Knoerzer D, Hochleitner G, Sørensen B, Hagl C, Pichlmaier M. Effects of fibrinogen concentrate as first-line therapy during major aortic replacement surgery: a randomized, placebo-controlled trial. Anesthesiology. 2013 Jan;118(1):40-50. doi: 10.1097/ALN.0b013e3182715d4d. Erratum in: Anesthesiology. 2013 May;118(5):1244. PMID: 23249928
Rahe-Meyer N, Levy JH, Mazer CD, Schramko A, Klein AA, Brat R, Okita Y, Ueda Y, Schmidt DS, Ranganath R, Gill R. Randomized evaluation of fibrinogen vs placebo in complex cardiovascular surgery (REPLACE): a double-blind phase III study of haemostatic therapy. Br J Anaesth. 2016 Jul;117(1):41-51. doi: 10.1093/bja/aew169. PMID: 27317703
Reynolds BR, Forsythe RM, Harbrecht BG, Cuschieri J, Minei JP, Maier RV, Moore EE, Billiar EE, Peitzman AB, Sperry JL; Inflammation and Host Response to Injury Investigators. Hypothermia in massive transfusion: have we been paying enough attention to it? J Trauma Acute Care Surg. 2012 Aug;73(2):486-91. PMID: 23019675
Rubiano AM, Sanchez AI, Estebanez G, Peitzman A, Sperry J, Puyana JC. The effect of admission spontaneous hypothermia on patients with severe traumatic brain injury. Injury. 2013 Sep;44(9):1219-25. doi: 10.1016/j.injury.2012.11.026. Epub 2012 Dec 27. PMID: 23273319
Sayah DM, Looney MR, Toy P. Transfusion reactions: newer concepts on the pathophysiology, incidence, treatment, and prevention of transfusion-related acute lung injury. Crit Care Clin. 2012 Jul;28(3):363-72, v. doi: 10.1016/j.ccc.2012.04.001. PMID: 22713611
Schroll R, Swift D, Tatum D, Couch S, Heaney JB, Llado-Farrulla M, Zucker S, Gill F, Brown G, Buffin N, Duchesne J. Accuracy of shock index versus ABC score to predict need for massive transfusion in trauma patients. Injury. 2018 Jan;49(1):15-19. doi: 10.1016/j.injury.2017.09.015. Epub 2017 Sep 15. PMID: 29017765
Simpson E, Lin Y, Stanworth S, Birchall J, Doree C, Hyde C. Recombinant factor VIIa for the prevention and treatment of bleeding in patients without haemophilia. Cochrane Database Syst Rev. 2012 Mar 14;(3):CD005011. doi: 10.1002/14651858.CD005011.pub4. PMID: 22419303
Slichter SJ. Relationship between platelet count and bleeding risk in thrombocytopenic patients. Transfus Med Rev. 2004 Jul;18(3):153-67. doi: 10.1016/j.tmrv.2004.03.003. PMID: 15248165
Spahn DR, Bouillon B, Cerny V, Duranteau J, Filipescu D, Hunt BJ, Komadina R, Maegele M, Nardi G, Riddez L, Samama CM, Vincent JL, Rossaint R. The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition. Crit Care. 2019 Mar 27;23(1):98. doi: 10.1186/s13054-019-2347-3. PMID: 30917843
Sperry JL, Guyette FX, Brown JB, et al. Prehospital Plasma during Air Medical Transport in Trauma Patients at Risk for Hemorrhagic Shock. The New England journal of medicine. 2018; 379(4):315-326. PMID: 30044935
Spinella PC. Warm fresh whole blood transfusion for severe hemorrhage: U.S. military and potential civilian applications. Crit Care Med. 2008 Jul;36(7 Suppl):S340-5. doi: 10.1097/CCM.0b013e31817e2ef9. PMID: 18594261
Ucar HI, Oc M, Tok M, Dogan OF, Oc B, Aydin A, Farsak B, Guvener M, Yorgancioglu AC, Dogan R, Demircin M, Pasaoglu I. Preoperative fibrinogen levels as a predictor of postoperative bleeding after open heart surgery. Heart Surg Forum. 2007;10(5):E392-6. doi: 10.1532/HSF98.20071065. PMID: 17855205
van Baarle FLF, van de Weerdt EK, van der Velden WJFM, Ruiterkamp RA, Tuinman PR, Ypma PF, van den Bergh WM, Demandt AMP, Kerver ED, Jansen AJG, Westerweel PE, Arbous SM, Determann RM, van Mook WNKA, Koeman M, Mäkelburg ABU, van Lienden KP, Binnekade JM, Biemond BJ, Vlaar APJ. Platelet Transfusion before CVC Placement in Patients with Thrombocytopenia. N Engl J Med. 2023 May 25;388(21):1956-1965. doi: 10.1056/NEJMoa2214322. PMID: 37224197
van den Brink DP, Wirtz MR, Neto AS, Schöchl H, Viersen V, Binnekade J, Juffermans NP. Effectiveness of prothrombin complex concentrate for the treatment of bleeding: A systematic review and meta-analysis. J Thromb Haemost. 2020 Oct;18(10):2457-2467. doi: 10.1111/jth.14991. Epub 2020 Aug 2. PMID: 32638483
van der Horst RA, Rijnhout TWH, Noorman F, Borger van der Burg BLS, van Waes OJF, Verhofstad MHJ, Hoencamp R. Whole blood transfusion in the treatment of acute hemorrhage, a systematic review and meta-analysis. J Trauma Acute Care Surg. 2023 Aug 1;95(2):256-266. doi: 10.1097/TA.0000000000004000. Epub 2023 May 1. PMID: 37125904
Vasudeva M, Mathew JK, Groombridge C, Tee JW, Johnny CS, Maini A, Fitzgerald MC. Hypocalcemia in trauma patients: A systematic review. J Trauma Acute Care Surg. 2021 Feb 1;90(2):396-402. doi: 10.1097/TA.0000000000003027. PMID: 33196630
Villanueva C, Colomo A, Bosch A, Concepción M, Hernandez-Gea V, Aracil C, Graupera I, Poca M, Alvarez-Urturi C, Gordillo J, Guarner-Argente C, Santaló M, Muñiz E, Guarner C. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med. 2013 Jan 3;368(1):11-21. doi: 10.1056/NEJMoa1211801. Erratum in: N Engl J Med. 2013 Jun 13;368(24):2341. PMID: 23281973
Wafaisade A, Lefering R, Maegele M, Brockamp T, Mutschler M, Lendemans S, Banerjee M, Bouillon B, Probst C; Trauma Registry of DGU. Administration of fibrinogen concentrate in exsanguinating trauma patients is associated with improved survival at 6 hours but not at discharge. J Trauma Acute Care Surg. 2013 Feb;74(2):387-3; discussion 393-5. doi: 10.1097/TA.0b013e31827e2410. PMID: 23354229
Webster S, Todd S, Redhead J, Wright C. Ionised calcium levels in major trauma patients who received blood in the Emergency Department. Emerg Med J. 2016 Aug;33(8):569-72. doi: 10.1136/emermed-2015-205096. Epub 2016 Feb 4. PMID: 26848163
Wikkelsø AJ, Edwards HM, Afshari A, Stensballe J, Langhoff-Roos J, Albrechtsen C, Ekelund K, Hanke G, Secher EL, Sharif HF, Pedersen LM, Troelstrup A, Lauenborg J, Mitchell AU, Fuhrmann L, Svare J, Madsen MG, Bødker B, Møller AM; FIB-PPH trial group. Pre-emptive treatment with fibrinogen concentrate for postpartum haemorrhage: randomized controlled trial. Br J Anaesth. 2015 Apr;114(4):623-33. doi: 10.1093/bja/aeu444. Epub 2015 Jan 13. PMID: 25586727
Wikkelsø A, Wetterslev J, Møller AM, Afshari A. Thromboelastography (TEG) or thromboelastometry (ROTEM) to monitor haemostatic treatment versus usual care in adults or children with bleeding. Cochrane Database Syst Rev. 2016 Aug 22;2016(8):CD007871. doi: 10.1002/14651858.CD007871.pub3. PMID: 27552162
Yang L, Stanworth S, Hopewell S, Doree C, Murphy M. Is fresh-frozen plasma clinically effective? An update of a systematic review of randomized controlled trials. Transfusion. 2012 Aug;52(8):1673-86; quiz 1673. doi: 10.1111/j.1537-2995.2011.03515.x. Epub 2012 Jan 18. PMID: 22257164Yücel N, Lefering R, Maegele M, Vorweg M, Tjardes T, Ruchholtz S, Neugebauer EA, Wappler F, Bouillon B, Rixen D; Polytrauma Study Group of the German Trauma Society. Trauma Associated Severe Hemorrhage (TASH)-Score: probability of mass transfusion as surrogate for life threatening hemorrhage after multiple trauma. J Trauma. 2006 Jun;60(6):1228-36; discussion 1236-7. doi: 10.1097/01.ta.0000220386.84012.bf. PMID: 16766965



6 thoughts on “Massive hemorrhage: a very deep dive”
The problem is that Massive Hemorrhage is a finding, not a diagnosis. Medical patients tend to have underlying medical problems. Trauma patients are usually young and healthy. Bleeding that can be stopped is completely different than that which continues. I recently had a patient who lacerated his radial artery. We immediately stopped the bleeding but he had no measurable BP and a HR above his age adjusted max. I gave a 500cc fluid bolus and started 2 units of O + blood. The nurses wanted to give more LR (no, he will be diluted to death) and then wanted to stop the blood after the lab reported his Hgb of 16 (no just get me 4 units of type specific). His repeated Hgb after 2 units of PRBCs was 4 so the nurses then wanted to start our massive transfusion protocol (no, he is not bleeding so he doesn’t need coagulation factors). He was fine after 6 units of PRBCs. No competent physician would have done anything different but cases like this make the literature impossible to interpret.
Great post!
Just a quick comment: BE and lactate (but BE are the best) on ABG are the best to identify a patient that is bleeding and, perhaps, it will require a lot of blood in the next hour.