
Last week we covered TXA for epistaxis. The NoPAC study kept with the recent tradition in TXA papers and showed no benefit. This week, we are going to look at another TXA RCT, but this time for the management of subarachnoid hemorrhage (SAH). In case you were worried, this paper also stays within that tradition.
The paper
Post R, Germans MR, Tjerkstra MA, et al; ULTRA Investigators. Ultra-early tranexamic acid after subarachnoid haemorrhage (ULTRA): a randomised controlled trial. Lancet. 2021 Jan 9;397(10269):112-118. doi: 10.1016/S0140-6736(20)32518-6. Epub 2020 Dec 23. PMID: 33357465 NCT02684812
The Methods
This is a multi-center, open-label, randomized, controlled trial from the Netherlands.
Patients
Adult patients presenting less than 24 hours after symptom onset with CT confirm SAH. Exclusions included perimesencephalic bleedings with normal mentation, trauma, a history of PE or DVT, severe renal failure, pregnancy, or imminent death.
Intervention
Tranexamic acid (TXA), started as soon as the diagnosis was made, 1 gram IV bolus, then 1 gram every 8 hours for 3 doses or until surgery started.
Comparison
Usual care.
Outcome
The primary outcome was a good neurologic outcome on the modified Rankin Scale (3 or less) based on a telephone call at 6 month.
The Results
They enrolled 955 patients over 6 years. (There isn’t a flow diagram to tell us how many they screened to find those 955.) The mean age was 58, 67% were female, 13% were on anti-platelet medications, and 3% on anticoagulation. TXA was given an average of 3 hours after symptom onset, and surgical management was done by an average of 14 hours. The groups look similar at enrollment.
There was no change in the primary outcome. If anything, the TXA group looks a little worse. A good neurologic outcome was obtained in 60% of the TXA group and 64% of the control group (OR 0.87, 95% CI 0.67-1.13).
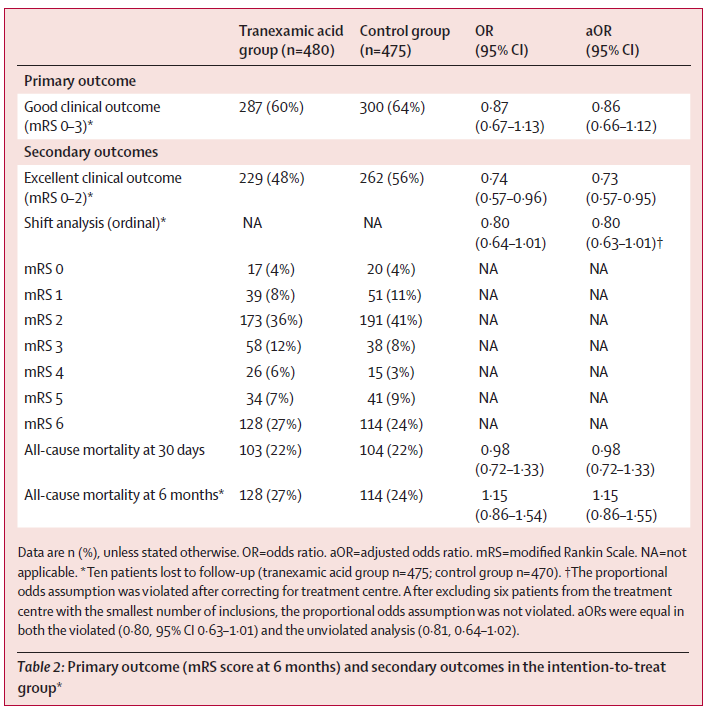
All cause mortality was 22% in both groups at 30 days. By 6 months it was 27% with TXA and 24% with placebo.
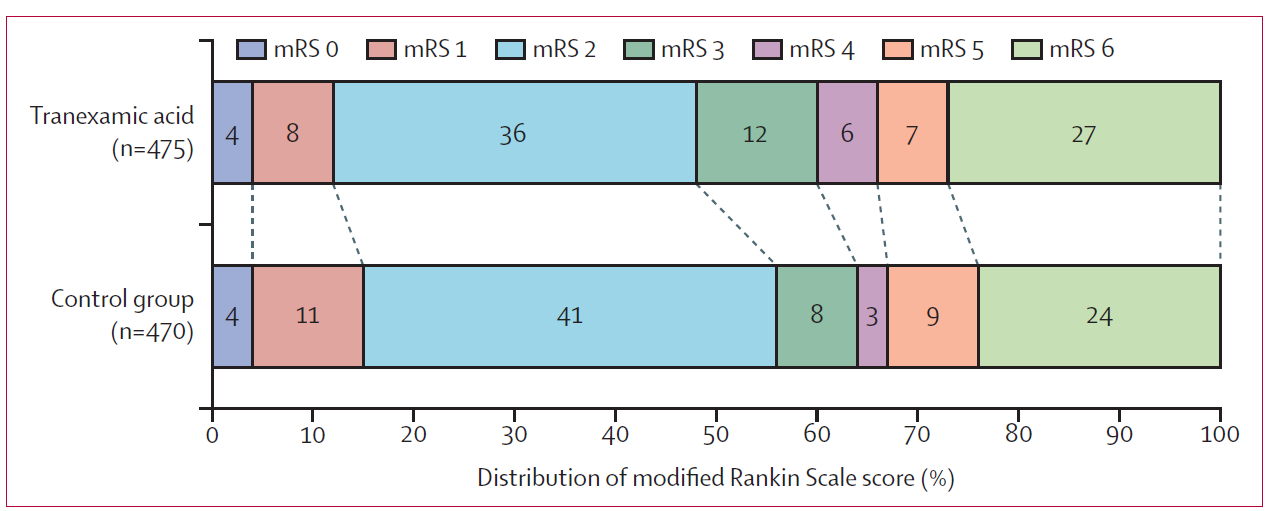
The ordinal shifts were not statistically different, although they came close. However, this “trend” was actually towards showing that TXA was harmful (OR 0.80, 95% CI 0.63-1.01). There weren’t any changes among the other secondary outcomes either.
My thoughts
This is another negative trial for TXA, which is becoming quite the trend. In fact, there is really only one high quality trial to ever show a benefit with TXA, and despite its size, CRASH 2 was not a perfect trial. Although they all look at different clinical scenarios, each additional negative TXA trial makes me more and more skeptical that TXA has any effect at all.
This trial is strong, but far from perfect. It was not blinded, which is always a major source of bias. However, usually unblinded trials favour the intervention, unless there is a lot of TXA skepticism among neurosurgeons (or the Dutch) that I am not aware of.
The modified Rankin Scale is a very poor tool, with poor inter-rater reliability, and therefore significant subjectivity (as I explore in much greater detail in the review of the thrombolytics for stroke literature). This is made worse by the fact that the outcomes were measured by phone, and even worse by the fact that this was an open label trial. This fact alone severely diminishes my trust in the results of this trial.
There are prior studies looking at TXA for subarachnoid hemorrhage. A Cochrane review found 10 RCTs, encompassing 1904 patients. (Baharoglu 2013) The overall quality isn’t great, with only 6 using placebo and only 5 employing an intention to treat analysis. TXA did not change the number of people with a poor neurologic outcome (RR 1.02, 95% CI 0.91 – 1.15). It also didn’t change all cause mortality (RR 1.00, 95% CI 0.85 – 1.18). There was a significant reduction in the rate of rebleeding (RR 0.64), however this was balanced by a significant increase in cerebral ischemia (RR 1.41). Neither surrogate really matters if both mortality and neurologic outcomes are completely unchanged. When combined with that prior data, this trial makes it pretty clear that TXA should not be used for all comers with subarachnoid hemorrhage.
Bottom line
This is the largest RCT to date looking at TXA in subarachnoid hemorrhage, and based on these results, it should not be prescribed routinely.
References
Baharoglu MI, Germans MR, Rinkel GJ, et al. Antifibrinolytic therapy for aneurysmal subarachnoid haemorrhage. The Cochrane database of systematic reviews. 2013; PMID: 23990381
CRASH-2 trial collaborators, Shakur H, Roberts I, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet (London, England). 2010; 376(9734):23-32. PMID: 20554319
Post R, Germans MR, Tjerkstra MA, et al; ULTRA Investigators. Ultra-early tranexamic acid after subarachnoid haemorrhage (ULTRA): a randomised controlled trial. Lancet. 2021 Jan 9;397(10269):112-118. doi: 10.1016/S0140-6736(20)32518-6. Epub 2020 Dec 23. PMID: 33357465
Morgenstern, J. TXA for SAH: Another swing and a miss for the wonder drug, First10EM, March 1, 2021. Available at:
https://doi.org/10.51684/FIRS.76651

3 thoughts on “TXA for SAH: Another swing and a miss for the wonder drug”
As someone claiming to be an impartial judge you failed to mention TXA reducing rebleeding, yet we’re more than eager to show case 64% vs 60% which is less of a statistical difference than 10% vs 14%… both of which are not statistically significant given the sample size.
I agree TXA is not effective in SAH.
I disagree with your bias while interpreting this article.
I strongly believe TXA has a place in non neurotic traumatic injuries where internal bleeding is likely.
I also strongly believe we should continue to test TXA’s effectiveness in head bleeds as this study has. Not so we can use TXA for bleeds, it wont work, but so that we may stop the fear of “giving seizures” or “messing with their brain.” As many of our less educated EMS coworkers have said by bumpers and break rooms.
Thanks for your comment. I am not sure it is fair. The outcome that you say I was “eager to show case” was the primary outcome of the trial. Of course I am going to talk about it. As for rebleeding – in a trial that has no change in mortality and no change in neurologic outcomes, rebleeding is completely irrelevant. It is a disease oriented outcome. The neurologic outcomes after a rebleed are the important outcomes, and if anything they seem to be worse with TXA.
Whether this is a topic worth more study is somewhat more complex. There was no hint of benefit in the earlier studies, and this trial was clearly negative, with even a hint of harm. That is certainly not definitive, but I imagine there are a lot better ways that we could spend research dollars, because this is a very long shot.