Should we use TXA for traumatic brain injury? This is a topic that received a lot of discussion after the CRASH3 trial was published. You can read my take on that trial here. In that blog post, I mention a second RCT that was completed long before CRASH3, but never published. (This is a form of publication bias.) That trial has now been published, so let’s do a quick update on the topic.
The paper
Rowell SE, Meier EN, McKnight B, et al. Effect of Out-of-Hospital Tranexamic Acid vs Placebo on 6-Month Functional Neurologic Outcomes in Patients With Moderate or Severe Traumatic Brain Injury. JAMA. 2020 Sep 8;324(10):961-974. doi: 10.1001/jama.2020.8958. PMID: 32897344. ClinicalTrials.gov Identifier: NCT01990768
The Methods
This is a multi-center, prehospital, randomized, double-blind trial from the North American Resuscitation Outcomes Consortium.
Patients
Patients aged 15 years and older with moderate to severe blunt or penetrating traumatic brain injury, a GCS 3-12, at least 1 reactive pupil, and a systolic blood pressure of at least 90.
Intervention
There were two intervention groups:
- TXA 2 gram IV bolus followed by a placebo infusion.
- TXA 1 gram IV bolus followed by 1 gram IV infused over 8 hours.
Comparison
Placebo for both the bolus and infusion.
Outcome
The primary outcome was functional neurologic outcomes at 6 months using the Glasgow Outcome Scale Extended (GOSE), dichotomized to favourable (GOSE >4) and poor (GOSE <5).
Glasgow Outcome Scale Extended
- Death
- Vegetative sate
- Lower severe disability – completely dependant on others
- Upper severe disability – dependent on others for some activities
- Lower moderate disability – unable to return to work or social activities
- Upper moderate disability – some disability but can return to some form of employment or social activities
- Lower good recovery – minor physical or mental defect
- Upper good recovery – full recovery
The Results
1063 patients were randomized, but 97 were excluded after randomization (not ideal, but understandable in prehospital research), leaving a study population of 966 patients.
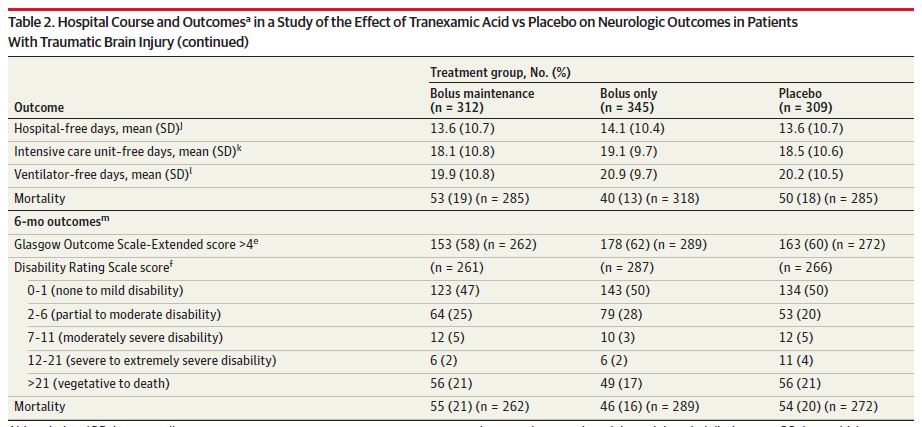
There was no difference in the primary outcome of favourable neurologic outcome on the GOSE score. 58% of the bolus/infusion group, 62% of the bolus only group, and 60% of the placebo group had a favourable outcome.
Overall mortality at 28 days was 16%, with 87% of being attributed to neurologic injury. Mortality was 21% with the bolus/infusion, 16% with the bolus alone, and 20% with placebo. The combined, adjusted analysis did not show a statistical difference between the groups (14% vs 17%, p=0.26).
Seizure looked a little higher in the bolus only group than the other groups (5% vs 2%).
My thoughts
This is a good RCT asking a question that we care about, but there are a few weaknesses to consider. About 10% of the patients were excluded after randomization, which can introduce bias. Furthermore, follow-up was incomplete, and loss to follow-up was unbalanced. More people were lost in the treatment groups, which could significantly bias the results. There appear to be some slight changes in the protocol that occurred after the data was collected, and not all the secondary outcomes appear to have made their way into the manuscript. Furthermore, they present their main outcomes after a statistical adjustment, but the details of this adjustment are not clear, including whether it was a planned adjustment.
As always, your interpretation of these results will depend on your pretest probability of TXA helping. Although TXA is often touted as a wonder drug, there is really only 1 high quality trial that demonstrated an important benefit with the agent (CRASH-2). Every other major trial has been negative (TICH-2, the WOMAN trial, CRASH-3, and HALT-IT). In the context of those massive, negative RCTs, my general sense is that TXA is far from a wonder drug. (I have a very long, deep-dive post on TXA pending, so hopefully you will be able to decide for yourself.)
I really like that they looked at different dosing regimens for TXA. The 8 hour infusion has always been annoying when managing trauma patients, and I know there are trauma experts who have been suggesting the 2 gram bolus to simplify treatment. Unfortunately, we know from the surgical literature that larger boluses are associated with seizures, and we seem to be seeing that here. If TXA could be given as a bolus rather than an infusion, that would eliminate one of the major harms of the drug (the fact that it can distract us from more important interventions). Although not definitive, this trial should raise questions about the safety of this approach.
One of the consistent comments about TXA is that it needs to be given early A prehospital trial is about as early as we can get, and these results do not look promising. That makes it somewhat less likely that TXA would help when given later in the emergency department.
There are some trends, which the authors describe using interesting statistics, suggesting that despite this negative trial there is still a chance that TXA could work. Overall, though, the results of TXA in TBI are not very encouraging. I have been privileged to be involved in a meta-analysis on the topic. I will share the results with you when they are published, but I will say that after reviewing all the data on this topic, I do not prescribe TXA for patients with traumatic brain injuries.
Bottom line
This is a large, double-blind RCT that demonstrated no benefit from giving TXA in the prehospital setting for traumatic brain injury. The trial is not definitive, but I believe the results.
Other FOAMed
TXA for traumatic brain injury:
EM Lit of Note: TXA, The Miracle Drug With Mostly Negative Trials
St Emlyn’s: JC: TXA in severe head injury.
Other TXA Trials:
TXA for GI bleeds: No benefit (The HALT-IT trial)
CRASH 3: TXA is no wonder drug
3 misunderstandings about WOMAN (TXA in postpartum hemorrhage)
References
Rowell SE, Meier EN, McKnight B, et al. Effect of Out-of-Hospital Tranexamic Acid vs Placebo on 6-Month Functional Neurologic Outcomes in Patients With Moderate or Severe Traumatic Brain Injury. JAMA. 2020 Sep 8;324(10):961-974.
Morgenstern, J. TXA in traumatic brain injury – a quick update, First10EM, September 28, 2020. Available at:
https://doi.org/10.51684/FIRS.46312


4 thoughts on “TXA in traumatic brain injury – a quick update”
Hi Justin, we always seem to take a different view on TXA and perhaps that says a lot about how the evidence is presented to us by the authors. In this study my concern was that did not stratify for GCS and pupils. Yet in CRASH-3 we know that there was a big difference between outcomes in these groups, and there is a good pathophysiological argument why TXA would not be effective in patients with severe brain injury.
I would love to see the results presented by initial GCS – as I think they said they would – but I cannot find that data.
S
Yeah – and I failed to mention in the write up that 40% of this group didn’t have intracranial hemorrhage, which significantly limits TXA’s chance of working. (I think I accidentally cut that paragraph – might add it back in after this post). There are lots of reasons that this study might have failed to show a benefit, but I am still not convinced that the subgroups in CRASH 3 are real. The authors of CRASH 3 themselves, in the protocol, said that they didn’t expect the effect of TXA to vary by severity of TBI, so those subgroups were really only emphasized after looking at / analyzing the data which makes them far more suspect. There are interesting enough for a follow up trial, but definitely not convincing enough to chance practice.