
Massive GI bleeds can be very scary (for both the patient and the clinician), and it makes sense that we want to do everything possible to stop the bleeding. Until now, I have been using TXA (tranexamic acid) as a component of my resuscitation for massive GI bleeds. I reviewed the prior evidence in this post, and although the trials were small and at high risk of bias, there was an indication of possible benefit that seemed to make it reasonable to prescribe. However, my primary conclusion in that post was that we need to wait for the results of the HALT-IT trial, and that I wouldn’t be surprised if the HALT-IT trial was negative. HALT-IT has now been published, and it appears I was correct: there is absolutely no benefit.
The paper
Roberts I, Shakur-Still H, Afolabi A, et al. Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): an international randomised, double-blind, placebo-controlled trial The Lancet. 2020; 395(10241):1927-1936. DOI: 10.1016/S0140-6736(20)30848-5 NCT01713101
The Methods
HALT-IT is a large, pragmatic, international, multi-centre, placebo-controlled RCT conducted in 164 hospitals in 15 countries.
Patients
HALT-IT included patients with acute gastrointestinal bleeding. The bleeding had to be defined as “significant” by the treating clinician, which was defined as a risk of bleeding death, and included patients with hypotension, tachycardia, signs of shock, or those likely to need transfusion, urgent endoscopy, or surgery. They included adult patients (of the age of consent in their country, so over 16 or 18). The treating clinician also had to be “substantially uncertain” about whether to use TXA.
Intervention
Tranexamic acid (TXA) 1 gram IV over 10 minutes, and then infused at 125 mg/hour for 24 hours.
Comparison
Matching placebo.
Outcome
They changed their primary outcome. The trial was originally designed to look at all-cause mortality, and they changed it to death due to bleeding at 5 days. Considering that all-cause mortality is an important outcome, and disease specific mortality is an inaccurate, imaginary statistical concept, I clearly think that was a bad choice.
The Results
HALT-IT enrolled 12,009 patients, with a mean age of 58, and 65% being male. The mean time from onset of bleeding to randomization was about 22 hours, with only 16% of patients presenting within the first 3 hours. 90% of patients had upper GI bleeding, and 45% were suspected of having variceal bleeds. Overall, the group only seems moderately ill, with almost 60% showing no signs of shock at enrollment.
There was absolutely no benefit.
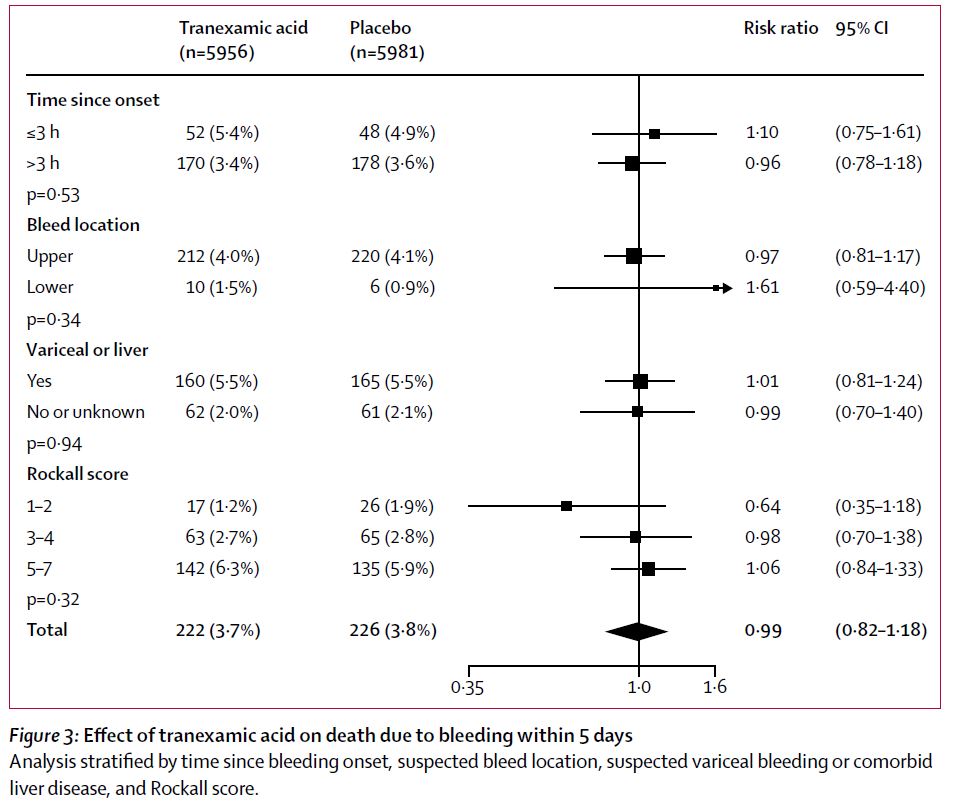
The new primary outcome, death due to bleeding at 5 days, occurred in 3.7% of the TXA group and 3.8% of the placebo group (RR 0·99, 95% CI 0·82–1·18).
The original primary outcome (and truly important outcome) of all cause mortality at 28 days was also unchanged (9.5% with TXA vs 9.2% with placebo, RR 1·03, 95% CI 0·92– 1.16).
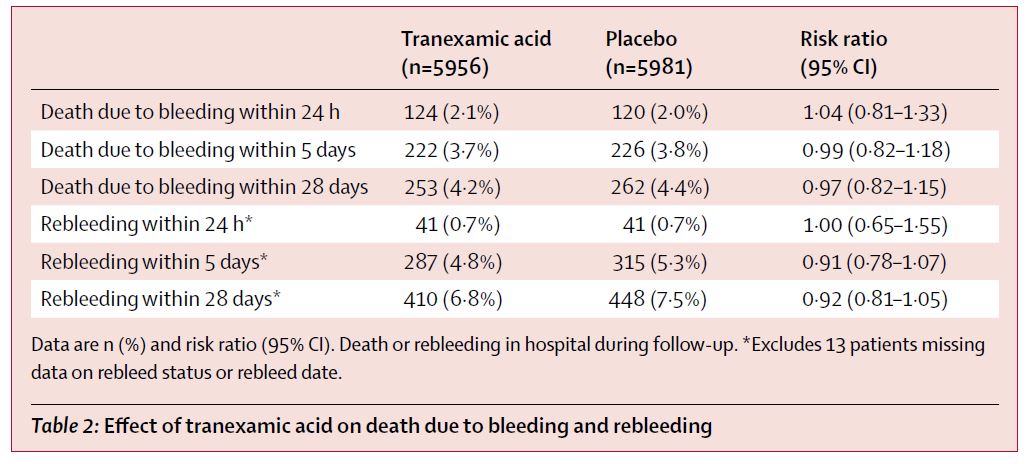
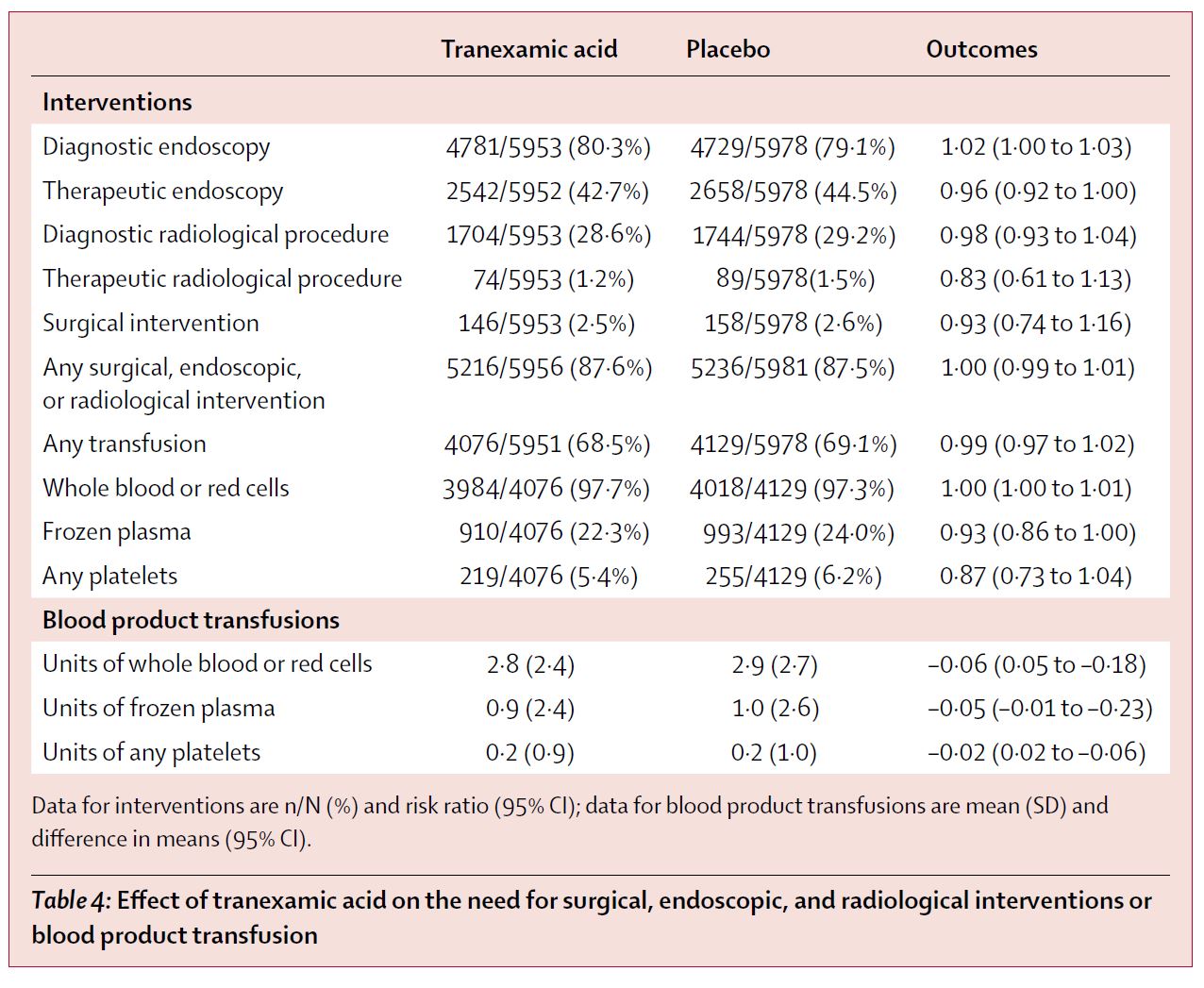
There were also no differences in rebleeding, surgery, endoscopy, need for transfusion, or total blood products transfused.
The only change in the trial was a doubling of venous thromboembolic events (from 0.4% with placebo to 0.8% with TXA, RR 1.85, 95% CI 1.15-2.98). This translated to a number needed to harm of 250.
My thoughts
HALT-IT was a fantastic and important trial. It answers a clinically important question about which we had lots of uncertainty. It had appropriate randomization, allocation concealment, and blinding. It enrolled appropriate patients, and therefore gives us an answer we care about. There were very few protocol violations and almost perfect follow-up. The risk of bias is pretty low, so I think you can trust these results.
That being said, there are a few reasons that this could be a false negative trial result. The patients presented later in this study than they do with trauma, and the time of onset of a GI bleed is less clear than it is with trauma. I am not sure the “3 hour rule” is really a thing, but there is some evidence that you need to give TXA early, and patients with GI bleeds might just present too late to benefit. (This is a clinical feature, not a fault of the trial. It is unlikely we will ever get TXA to these patients early, so TXA is unlikely to help. Also, the group that was treated early in this trial actually had a higher mortality.) I also think TXA is less likely to help brisk, arterial type bleeding, as a clot never forms for TXA to stabilize. Although varices are technically venous, they bleed with a lot of force. 45% of the patients in this trial had suspected variceal bleeding, and I could imagine that TXA would be less likely to work in this subset of patients (although it is also the subset in which we most want it to work). That being said, seeing as we don’t know the cause of bleeding in the emergency department, this distinction is not super helpful for the resuscitation.
Luckily, the decision to change the primary outcome to disease specific mortality did not result in confusion this time, but it was still a very poor choice. I have discussed this in the past, but disease specific mortality is inaccurate, misleading, and doesn’t actually represent a real entity. It is inaccurate because it is based on what the treating clinician writes on the death certificate, not even autopsy, which is prone to way too much error. More importantly, it is not a thing you can point at in the real world. You are either alive or dead. You aren’t “dead due to bleeding.” It is an outcome that sounds important, but does not represent any patient important outcome, and therefore often completely misleads us.
Doctor: The treatment was a resounding success!!!
Nurse: But doctor, the patient is dead…
Doctor: Yes, but she didn’t die from bleeding!
I think it is worth noting that a form of publication bias can occur even when trial results are published. When CRASH3 was published, the internet was flooded with infographics and advertisements touting the “miracle cure”. This is an equally important trial, and I can’t find a single infographic or press release on their website. This is less important than true publication bias, where the results are completely hidden, but our awareness of scientific results can also be shaped by how widely they are discussed, and positive results are always more advertised than negative, despite being equally important to our patients.
As an aside, I think the authors do an excellent job describing a stepwise consent process that acknowledges the difficulties with consent in the context of critical illness. I am still not sure that any critically ill patient can truly understand and appreciate the implications of research, so safety structures are clearly important. The process they describe sounds good, and should probably be replicated in other critical care research.
HALT-IT is the 4th major RCT of TXA in a row with negative results. TICH-2 found no difference in mortality or neurologic outcomes with TXA in intracerebral hemorrhage. (Sprigg 2018) The WOMAN trial found no difference in mortality or hysterectomy in patients with postpartum hemorrhage. (WOMAN 2017) The CRASH3 trial found no difference in mortality or neurologic outcomes in patients with traumatic brain injury. (CRASH3 2019) And now HALT-IT finds no difference in mortality in GI bleeds. There have been a handful of positive studies for things like epistaxis and hemoptysis, but those studies are small and at high risk of bias, so not nearly as reliable as these 4 major trials. I think it is interesting to consider how the totality of this evidence affects our understanding of TXA, and especially our interpretation of CRASH2.
Although it has been enshrined in the EBM hall of fame, CRASH2 did have a number of issues that could have biased the results of the trial, and should make us less certain about the reported benefit. (CRASH2 2010) I think the results were convincing enough to change practice. I give TXA to all my high risk bleeding trauma patients. However, I also recognize that the results of CRASH2 could be wrong. Replication is the foundation of science, no matter how small a p value a single trial happens to obtain. I think we need further RCTs to confirm the role of TXA in trauma, especially in modern trauma systems that were not well represented in CRASH2. If all the subsequent TXA trials had been positive, they would have reassured me about the CRASH2 results. Insead, these results make CRASH2 look like a bit of an outlier. The overwhelmingly negative data from TXA since CRASH2 really highlights the need for a replication of that seminal study.
Bottom line
This is a very high quality RCT that demonstrated no benefit from TXA in GI bleeding, and a small increase in venous thromboembolism. TXA should not be routinely used for GI bleeding.
Other FOAMed
Coming soon, I am sure.
References
Brenner, A., Afolabi, A., Ahmad, S.M. et al. Tranexamic acid for acute gastrointestinal bleeding (the HALT-IT trial): statistical analysis plan for an international, randomised, double-blind, placebo-controlled trial. Trials 20, 467 (2019). https://doi.org/10.1186/s13063-019-3561-7
CRASH-2 trial collaborators, Shakur H, Roberts I, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet (London, England). 2010; 376(9734):23-32. PMID: 20554319
CRASH 3 Trial Collaborators. Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH 3): a randomised, placebo-controlled trial. Lancet (London, England). 2019; PMID: 31623894 [free full text] Cincaltrials.gov: NCT01402882
Sprigg N, Flaherty K, Appleton JP, et al. Tranexamic acid for hyperacute primary IntraCerebral Haemorrhage (TICH-2): an international randomised, placebo-controlled, phase 3 superiority trial. Lancet (London, England). 2018; 391(10135):2107-2115. PMID: 29778325 [free full text]
WOMAN trial collaborators . Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet (London, England). 2017; PMID: 28456509 [free full text]
Morgenstern, J. TXA for GI bleeds: No benefit (The HALT-IT trial), First10EM, June 19, 2020. Available at:
https://doi.org/10.51684/FIRS.26255



13 thoughts on “TXA for GI bleeds: No benefit (The HALT-IT trial)”
Hey Justin, great review of a great study.
Just wanted to say that as one of the HALT-IT collaborators, I wasn’t really surprised at the “no benefit” result of the trial. I was very interested in your comment about the potential for this being a false negative trial.
As well as a modification of primary outcome during the trial, the recruitment target was changed at the end of 2017 (by which time we had been pulled for losing equipoise) from 8000 to 12000. I judged at the time (and I’d be interested to know if I was wrong to do this empirically) that it was because the data was showing a minimal difference if any at all and they wanted to avoid a Type II error.
https://clinicaltrials.gov/ct2/history/NCT01658124?A=1&B=7&C=Side-by-Side#StudyPageTop
I’m not disagreeing with your analysis of the pathophysiology of a GIB, just wondering if it makes any difference to the potential for a false negative result?
BW
David
Thanks for the comment, and the incredible work!
I think this is one of the most important distinctions in EBM, and one that we overlook all the time. There are two major aspects of trial that can make it either falsely positive or falsely negative: chance and bias. The massive sample sizes of CRASH2 and HALT-IT make chance errors much less likely, but do nothing to deal with issues of bias. I think it is incredibly unlikely that if this trial were exactly repeated that we would see a benefit. There was a Type II statistical error. However, that doesn’t exclude a benefit in a different population (ie if we could get treatment on board earlier). That’s what I was trying to get at with that comment.
The converse is true of CRASH2. The massive numbers mean that a statistical or chance error is very unlikely, but that doesn’t eliminate errors from internal and external validity.
I actually don’t think it is very likely that this is a false negative, but much like we always discuss the short-comings of positive trials, it is also important to consider the reasons why the results of a negative trial may be incorrect.
Does that answer your question?
Yeah, I think so.
It was a great trial to be a part of, while it lasted.
Now just got to change policy / minds in the place that I work!
Otherwise, why bother doing the work in the first place?
Yet another excellent review Justin, thank you.
I’m a bit concerned about the use of the terminology “false negative trial”. This leaves the reader with the impression that you think the trial was negative when it really should have been positive.
You do go on to explain what you mean – that there are very good reasons in practice why TXA might not help, but you leave the reader with the impression that if they do the study again “the right way”, a different result would result.
Thanks for the comment. I hope with the title and bottom line pretty strongly proclaiming a lack of benefit, no one will be confused by the discussion going into the various ways that trials can be misleading. No single trial can stand alone as “the answer” in science, and I think routinely discussing these shortcomings helps prevent that common mistake in medicine.