Morgenstern, J. PATCH-trauma: Another negative (but complicated) TXA trial, First10EM, July 12, 2023. Available at:
https://doi.org/10.51684/FIRS.130935
I have spent a lot of time reading and talking about the TXA literature. The more literature I see, the less valuable TXA seems. However, trauma remains the one area of practice with a clearly positive trial, with the CRASH2 trial that started it all. Despite its size, the CRASH2 trial was imperfect, and replication is the core of science, so I have always said we need more studies in this area. The PATCH-Trauma trial, although not actually a replication of CRASH2, is the closest we have seen, in a high quality double blind RCT of prehospital TXA in trauma.
The paper
PATCH-Trauma Investigators and the ANZICS Clinical Trials Group; Gruen RL, Mitra B, et al. Prehospital Tranexamic Acid for Severe Trauma. N Engl J Med. 2023 Jun 14. doi: 10.1056/NEJMoa2215457. Epub ahead of print. PMID: 37314244 NCT02187120
The Methods
A double-blind, placebo controlled RCT from 15 EMS services and 21 hospitals in Australia, New Zealand, and Germany.
Patients
Adult trauma patients with suspected severe injuries thought to be at risk of trauma induced coagulopathy (based on the COAST score) and in whom the study drug could be given within 3 hours.
Exclusions: pregnancy and residence in a facility for older persons.
Intervention
TXA 1 gram IV pushed over 10 minutes, followed by a second gram infused over 8 hours.
Comparison
Matching placebo.
Outcome
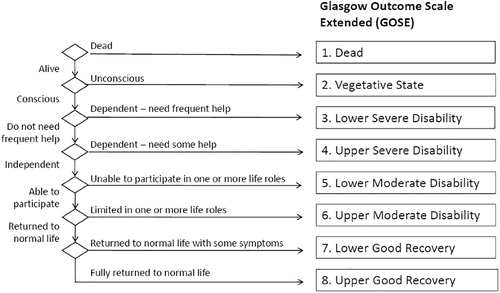
The primary outcome was survival with a favorable functional outcome at 6 months, based on the Glasgow Outcome Scale – Extended (GOS-E).
The Results
They enrolled 1310 patients. After loss to follow-up, withdrawal of consent, and a few patients in whom the study packs were lost, there were 1131 patients included in the primary intent to treat analysis.
The patients are what you would expect for trauma: young (44 years) and predominantly male (70%). About 24% had laboratory evidence of coagulopathy. These were badly injured patients, with a median ISS of 29. Most (92%) had blunt trauma. About 40% received a diagnosis of severe head of neck injury. Protocol variations occurred in more than 30% in both groups, including about 15% of both groups receiving open-label TXA.
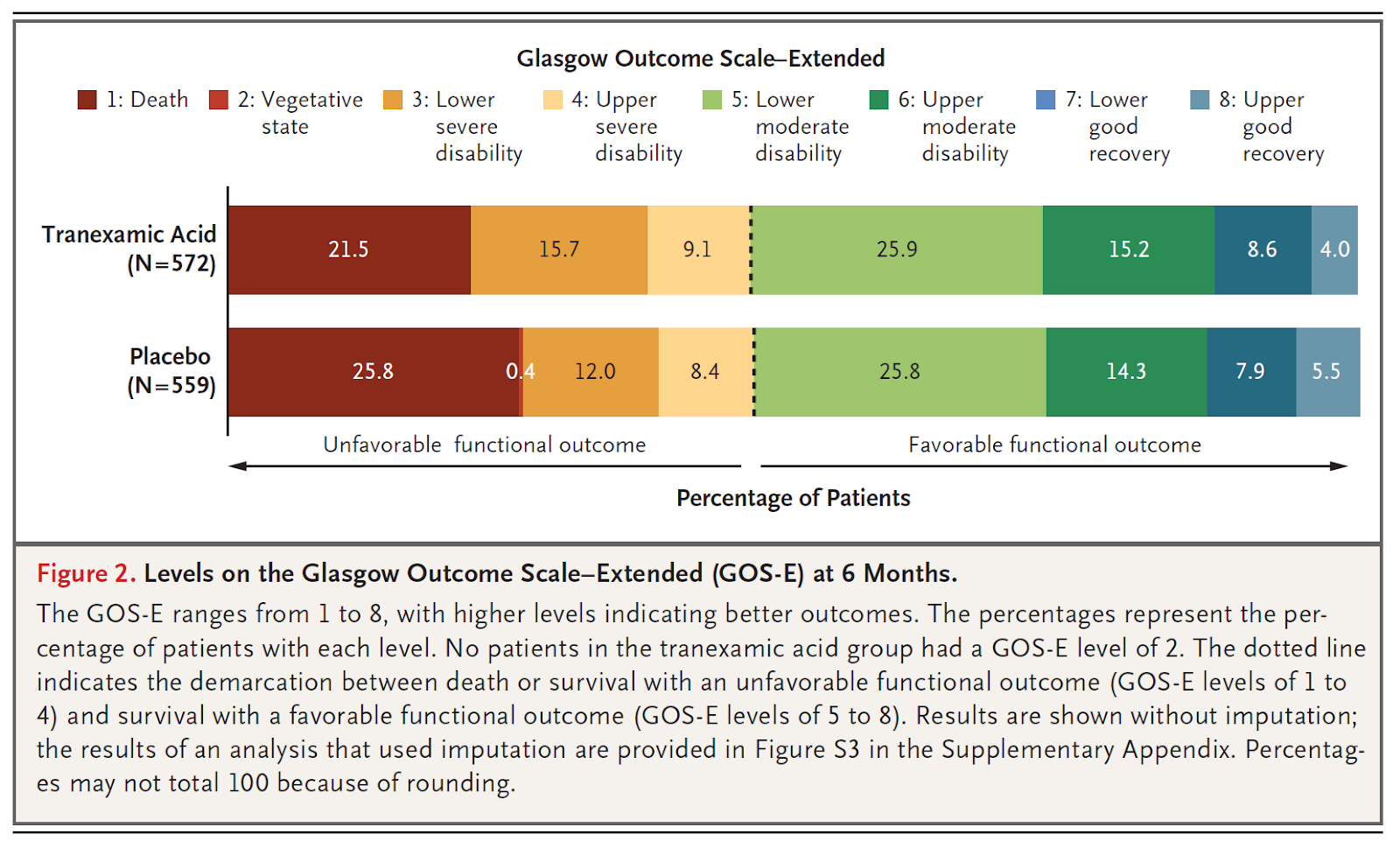
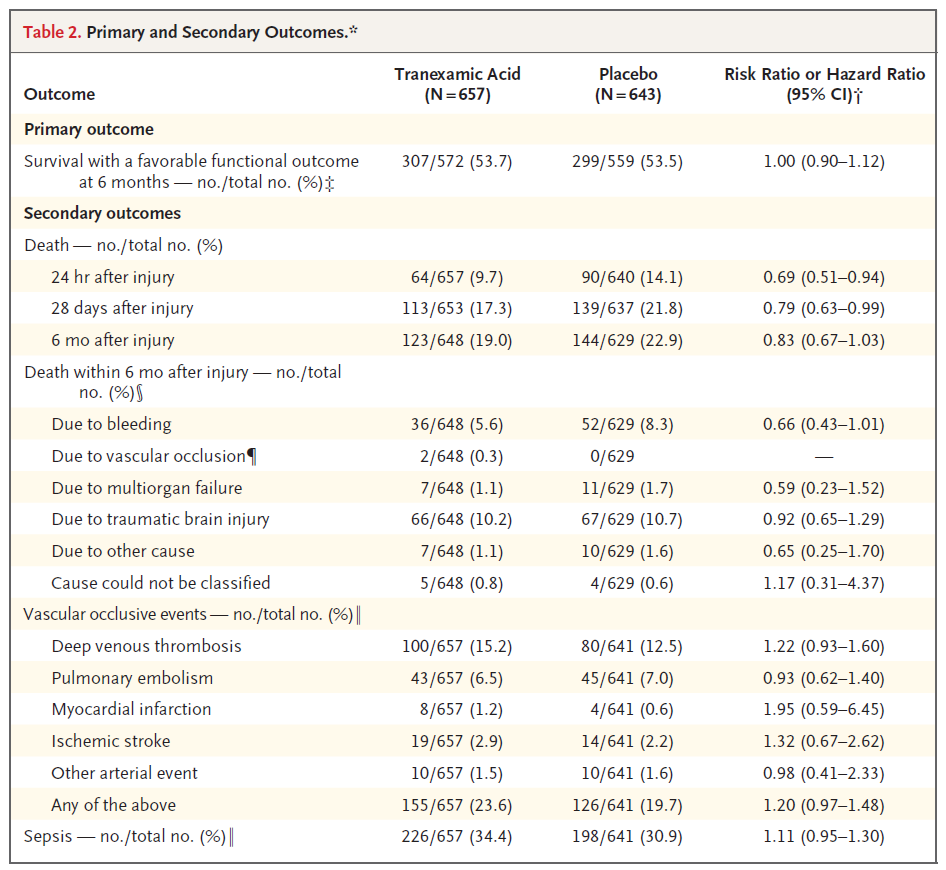
There was no difference in the primary outcome of favourable functional outcome at 6 months (53.7% vs 53.5%, RR 1.00, 95%CI 0.9-1.12, p=0.95).
6 month mortality was also not statistically different between the groups (19% vs 23%, RR 0.83, 95%CI 0.67-1.03). However, the difference here would still be clinically significant, and there was a statistical difference favouring TXA in 24 hour and 28 day mortality.
Conversely, vascular occlusive events were not statistically higher with TXA, but the difference would be clinically important (20% vs 24%, RR 1.2, 95% CI 0.97-1.48).
This graph seems to indicate that almost all of the difference between the two groups was a shift from death to the worst category of severe disability:
My thoughts
I have always argued that we need a replication of CRASH2. Although CRASH2 was an amazing study, and I give my bleeding patients TXA based on CRASH2, there were many issues with CRASH2, and I still believe that a high quality replication has at least a 50% chance of demonstrating no benefit. Since CRASH2, there have been many large high quality trials of TXA in other conditions (HALT-IT, CRASH3, WOMAN, NOPAC, TICH2), all of which have been negative (although not without some debate). These trials have made it very clear that TXA is not a wonder drug, and have really emphasized the need for a CRASH2 replication. In PATCH-Trauma we get our first quasi-replication, and like the many other trials we have seen since CRASH2, it is a negative trial, but with multiple complicating factors.
The primary outcome of this trial is clearly negative. The groups look identical. Therefore, any arguments you hear about this trial will all be based around secondary outcomes. However, you should be very cautious of secondary outcomes. (This is especially true in medicine, because the statistical cutoffs we use are far more prone to false positives than those used in other sciences.)
Before getting to the secondary outcomes, let’s think a little bit about the logic behind the primary outcome. When assessing other therapies, such as epinephrine in cardiac arrest, I have spent a lot of time talking about the importance of looking at functional outcomes over all cause mortality. Patients have told the medical community very clearly that functional outcomes are more important than simple survival. However, I am not sure this outcome makes as much sense in the context of trauma. In cardiac arrest, we anticipate that people will have devastating neurologic outcomes, and simply restarting the heart doesn’t solve that issue. Furthermore, cardiac arrest studies generally include older patients with more comorbidities, who are more reticent to have prolonged invasive medical interventions.
In trauma, there are really two completely distinct groups of patients: those with and without brain injury. I anticipate poor functional outcomes in the setting of brain injury, and would make functional outcomes my primary outcome in that setting. However, in a general trauma population, with a focus on the subset of patients with hemorrhage, mortality might be the more important primary outcome. Furthermore, the trauma population is usually younger and lacking significant comorbidities, and therefore might be more willing to accept the risk of a poor functional outcome for the benefit of survival. (I have never seen research looking at opinions about mortality and quality of life in the trauma population, but I expect the answers might be very different from what we see in the cardiac arrest literature.)
The other major point of debate is the time frame of 6 months. Mortality at 6 months is clearly more important than mortality at 24 hours, but it also complicates study interpretation, as long term mortality is influenced by many factors other than the study drug. I don’t expect TXA to have long term effects. Run any study long enough, and mortality will reach 100%. On the other hand, short term benefits that cannot be maintained are not real benefits (think heparin in ACS). Conversly, some might argue that 6 months was too early a cutoff for neurologic outcomes, as function often continues to improve with physiotherapy long after trauma. People might quibble, but I think 6 months was an appropriate choice for this study, and an appropriate time frame on which to judge our resuscitative efforts.
Although the primary outcome in this trial is exactly neutral, I think it probably demonstrates harm (if we believe the mortality numbers from the secondary outcomes). More people are alive, but there is no difference in the number of people with good functional outcomes. The graph demonstrates pretty clearly that all of the saved lives end up with severe disabilities. How that should drive practice is a value judgment that reaches far beyond science, but it is a value judgment that medicine really needs to grapple with.
This trial is also a very long way from perfect, with 35% of patients having some kind of protocol violation. This included about 15% of the placebo group getting TXA and and 21% of the TXA not getting the infusion dose. Those protocol violations could certainly bias the trial results towards the null hypothesis. There was also a significant loss to follow-up in this trial, which adds uncertainty around the results.
I have some concerns about the enrollment in this trial and the potential for selection bias. The manuscript doesn’t say how many people they screened in order to identify the 1310 originally enrolled. However, considering that the study period was more than 7 years, they were enrolling less than one patient a month at each hospital, which is clearly only a tiny subset of all trauma patients. What happened to all the other patients?
In the modern era of publication, where papers are released electronically rather than on paper, there is really no reason to leave important information out of manuscripts, but it happens with almost every manuscript I read. It drives me crazy when there are dozens of secondary outcomes listed in the clinicaltrial.gov listing, but only a small subset are included in the manuscript. This is a form of a bias, in which authors get to pick and choose which information to present to us, which is one of the many reasons you should always be very skeptical of secondary outcomes.
Among the secondary outcomes, it is interesting to note that the group given TXA after 2 hours in this trial looks like they have worse outcomes, although the results are nowhere close to statistical significance. The association between delayed TXA and harm grows stronger, although it still isn’t exactly clear what that means.
Although I was already very skeptical about the role of TXA in trauma, and this is a negative trial, I don’t think it is enough to overrule the results of CRASH2. I will continue to give TXA to my bleeding trauma patients, as long as they are seen within 2-3 hours. However, I think there is clearly equipoise, that a CRASH2 replication is warranted, and that there is at least a 50% chance that replication will be negative.
Bottom line
This is a double blind, multicentre, prehospital trial of TXA for patients with severe trauma and predicted trauma induced coagulopathy. There was no difference in the primary outcome of 6 month survival with good functional status. However, these results are probably not enough to overrule the CRASH2 trial, and therefore I don’t think practice should (or will) change based on this trial.
Other FOAMed
SGEM 408: Hey, I, Oh I;m still alive – Is it due to TXA?
REBELEM: Rethinking the Role of TXA: Are We Asking Too Much?
St Emlyn’s: The PATCH trial. TXA in major trauma
References
PATCH-Trauma Investigators and the ANZICS Clinical Trials Group; Gruen RL, Mitra B, Bernard SA, McArthur CJ, Burns B, Gantner DC, Maegele M, Cameron PA, Dicker B, Forbes AB, Hurford S, Martin CA, Mazur SM, Medcalf RL, Murray LJ, Myles PS, Ng SJ, Pitt V, Rashford S, Reade MC, Swain AH, Trapani T, Young PJ. Prehospital Tranexamic Acid for Severe Trauma. N Engl J Med. 2023 Jun 14. doi: 10.1056/NEJMoa2215457. Epub ahead of print. PMID: 37314244



4 thoughts on “PATCH-trauma: Another negative (but complicated) TXA trial”
Excellent review as always. I am frustrated by these scoring systems. There are robust systems to measure outcomes i.e. QALYs and DALYs. Death scores better than severe disability on any patient centered outcome measure and the ALYs allow valuing a leg amputation vs aphasia.These systems are not perfect but are far better than “lower severe disability” whatever that means.