Morgenstern, J. Balanced transfusion: Less evidence than you might think, First10EM, March 27, 2023. Available at:
https://doi.org/10.51684/FIRS.129577
Over the last decade, I have heard the language around balanced transfusions shift from an ‘interesting new idea’ to the ‘proven standard of care’. Although that is the direction that science is supposed to progress, in this case there is really no science. We only have a single full RCT, and it showed no difference based on transfusion ratios. In that context, I find this shift in language troubling.
We seem to do this all the time in medicine. When a new study is published, we talk about its many shortcomings in our journal clubs. We emphasize the need for caution; the necessity for replication. Then a few years go by and the practice is incorporated into guidelines. In order to provoke practice change, people at conferences use strong language, omitting all nuance. These novel practices are interesting topics for grand rounds, and learners are exposed to these ideas frequently. However, these lectures are usually framed as ‘this is now how we practice’, rather than exploring the underlying evidence and uncertainty. And so over a few short years, a practice with questionable evidence becomes enshrined as standard care. We seem to collectively forget about evidence based medicine. Then a (predictably) negative study is published, and the medical world acts shocked at this ‘medical reversal’ that actually perfectly matches the original research. Or worse, that follow-up research is never done, and we continue to practice in veiled ignorance.
We move through this cycle of evidentiary amnesia over and over again. I see it in the guidelines for blood pressure management in intracranial hemorrhage. We definitely see it in every discussion of ‘therapeutic’ hypothermia. The language we use to talk about topics like fluids in pediatric DKA, balanced IV solutions, TXA for most indications, and pediatric UTI, among a much much longer list, lacks nuance and seems to forget the massive limitations of the available science.
In that context, I thought it would be worthwhile to review the evidence for balanced transfusions.
The RCT
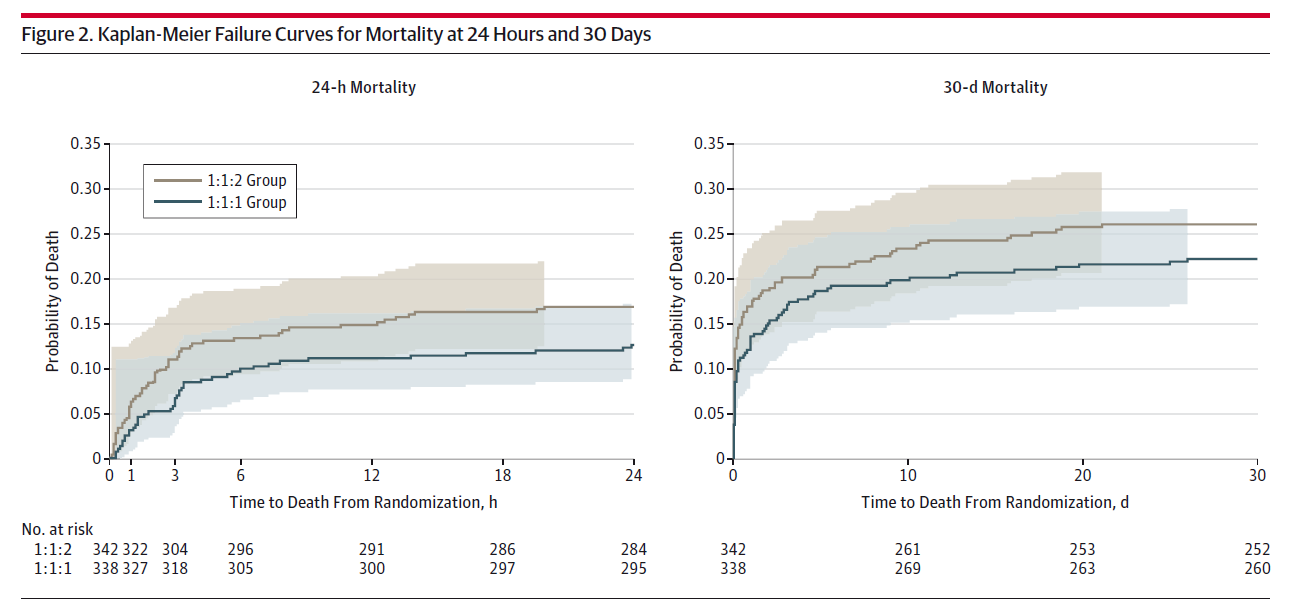
The one RCT of balanced transfusion that we have is the PROPPR trial, a multi-center, partially blinded, RCT comparing a 1:1:1 ratio of plasma to platelets to red blood cells to a 1:1:2 ratio in 680 adult trauma patients predicted to need massive transfusion. (Holcomb 2015) Statistically speaking, this was a negative trial, with no difference in all cause mortality, which was their primary outcome. That being said, the point estimate for mortality at both 24 hours (12.7% vs 17.0%, p=0.12) and 30 days (22.4% and 26%, p=0.26) was better in the 1:1:1 group, so this trial can’t be used to make a definitive conclusion one way or the other. There were also no significant differences in any of their original secondary outcomes, including time to hemostasis, total blood products used, hospital free days, ICU free days, ventilator free days, functional outcomes, or disposition.
Despite being an excellent and necessary trial, PROPPR has numerous weaknesses that add uncertainty. The treating physicians were unblinded, and lack of blinding is the biggest single source for bias in any trial. It is probably underpowered, as they were rather optimistic in designing the trial thinking that a 1:1:1 ratio would result in a 10% absolute decrease in mortality. Perhaps the most important thing to note about this trial is that it just assumed that a ratio was important, rather than including a control group which just received packed red blood cells (which would have been standard care in 2012).
So, PROPPR was a negative trial, but it hints at a possible benefit. It doesn’t prove that balanced transfusion helps, but it also doesn’t prove that it’s useless. The treatment strategy remains unproven.
Although PROPPR is the only full RCT of balanced transfusion, there was another pilot RCT that is worth mentioning. (Nascimento 2013) They only include a total of 78 adult trauma patients, randomized to either a 1:1:1 ratio or control (laboratory guided transfusion of platelets and plasma), as their goal was just to test the feasibility of the research. They found that the RCT was feasible, but did result in more plasma wastage. However, I think it is worth noting that their clinical results are dramatically different from PROPPR. Mortality was 32.5% with the 1:1:1 ratio, as compared to 14.3% in the control group, an absolute increase in mortality of 18.2% which came very close to being statistically significant (95% CI -0.4 to 36.8% absolute difference in mortality). People only ever talk about PROPPR, but in the one other trial we have, mortality doubled in the 1:1:1 group! When data is imperfect, you really want to see consistency. We certainly don’t have that here.
Observational data
Before discussing individual observational trials, we need to discuss the one major bias that shapes this entire topic: survivorship bias. In short, people who survive longer have more time to be given more treatments.
In terms of balanced transfusions, it is important to remember what practice looked like in 2010. We routinely gave 6 or more units of packed red blood cells before even thinking about platelets or FFP. Thus, the platelets and FFP were frequently given hours into the resuscitation. And when do many trauma patients die? The first few hours. In other words, the only patients who received FFP and platelets were those healthy enough to survive.
With such an inherent bias, you would usually want to use propensity-matching or other related statistical tools when analyzing the observational datasets. I don’t think these techniques really work in trauma. Usually, propensity matching is based on age and comorbidities, but those aren’t the factors that really drive mortality in trauma. Even vital signs are significantly impacted by things like time since injury, and so not directly related to severity of injury. What really drives mortality in trauma is the pattern of injury, but that is not something that is clearly recorded on a chart, and therefore propensity matching is unlikely to be helpful in these trauma data sets. (I will admit that I am not a statistician, so people may want to correct me here.)
This survivorship bias is nicely demonstrated in the PROMMTT trial (discussed below). At 30 minutes 99% of the cohort had not received platelets and 67% had not received plasma. (All patients had received at least 1 unit of PRBCs to be enrolled). At 3 hours, 28% had not received platelets and 10% had not received plasma. Despite the lag to receive balanced transfusion, the majority (58%) of deaths occurred within the first 3 hours. In other words, most patients didn’t survive long enough to receive platelets and plasma.
The bottom line is, at least based on the way trauma patients were managed a decade ago, we expect patients who received FFP and platelets to be somewhat less sick and therefore to have lower mortality than patients who only received PRBCs.
The PROMMTT study is a prospective cohort from 10 US level 1 trauma centers looking at adult trauma patients who received at least 3 units of red blood cells in the first 24 hours. (Holcomb 2013) The trial includes 905 patients (out of 34,362 trauma admissions). Data collection was only initiated on ⅓ of the cohort, so selection bias is a massive concern. There is a strong association between higher transfusion ratios and decreased mortality for the first 6 hours (HR0.31), although the trend reverses by 24 hours and indicates possible harm (HR 1.2). As discussed above, there is a strong indication of survivorship bias in this data.
In what I think is the largest dataset to date, Nederpelt and colleagues performed a retrospective review of a trauma database, looking at patients who received at least 10 units of PRBCs and 1 unit of FFP. (Nederpelt 2019) The result is a cohort of 4427 patients (out of more than a million in the trauma database) with a median injury severity score of 29. They excluded patients who died in the emergency department, which helps decrease the risk of survivorship bias, but also means the data is hard to apply to the patient in front of you. Most patients (72%) in the database were being treated with a 1:1 or 1:2 FFP:PRBC ratio. In other words, the community had already bought into the dogma, and it is likely that patients receiving lower ratios were not being given those ratios on purpose, but because of some other undescribed confounder, which is a significant source of bias. There is a significant association between lower transfusion ratios and increased mortality. However, this is a retrospective look at a database that is designed for QA rather than research, which leaves it as low quality data.
The other observational studies are mostly similar, although mostly lower quality. The association between balanced transfusion and decreased mortality is fairly consistent, although as compared to many other topics, the numbers are relatively small. (Bhangu 2013; da Luz 2019) However, there is no way to know whether this consistency is because of a treatment effect or an artifact of survivorship bias. Thus, the conclusions we can draw from observational data are extremely limited.

However, not every study reaches the same glowing conclusion. A chart review of 1788 patients who ended up receiving less than 10 units of PRBCs (so not massive transfusion), which used propensity matching based on initial bloodwork, compared the outcomes of patients with high ratios of platelets and FFP to PRBC (1:1 or more) to those with low ratios (1:2 or less). (Sambasivan 2011) Although not statistically significant, patients with high FFP ratios had a mortality of 23% as compared to only 13% in those with low ratios. For platelets, the mortality was 21% in the high ratio group as compared to 14% in the low ratio group. Those would certainly be clinically important outcomes, and they go in the exact opposite direction of the other studies discussed. There were statistically significant increases in ventilator use and ICU use in the patients receiving more platelets and plasma. Like the purported benefits above, it is possible that all these differences are fake, based on bias or underlying confounders. However, it is also theoretically possible that these transfusion ratios help in massive transfusion, but cause significant harm in less sick patients. That would be a major problem, as it isn’t always easy to predict which patients will need more than 10 units of blood (the cutoff used in this study), and should give us caution when rushing to start platelets and plasma.
Not all bleeding is trauma
Balanced transfusions came into vogue based on trauma literature, but the concept was quickly adopted for just about any bleeding patient. But what is the evidence outside of trauma?
One single-center chart review looked at all massive transfusions given, and compared trauma to non-trauma patients. (Mesar 2017) There were a total of 865 massive transfusion events, of which the vast majority (89%) occurred in non-trauma patients. Comparing survivors to nonsurvivors, the FFP:RBC ratio was identical (1:1.5 in both groups). (All of the caveats about bias in observational research apply.)
Another very similar retrospective analysis looking at 600 nontrauma patients receiving massive transfusion found no association between mortality and FFP to PRBC ratio (using a cutoff of 1:2). (Etchill 2017) There were also no associations with hospital length of stay, ICU days, or ventilator-free days.
It was not the focus of my review, but, despite widespread adoption, there does not seem to be a lot of data on balanced transfusion outside of trauma.
Discussion
The pathophysiologic rationale for balanced transfusion is strong. Coagulopathy is strongly associated with death in trauma, and dilution of coagulation factors is a major component of that coagulopathy. Our pretest probability for benefit should probably start much higher than many other therapies. That being said, Richard Dutton freely admits that he just made up the 1:1:1 ratio based on the rationale that it mimics whole blood, and there are significant harms and costs to using plasma and platelets that need to be considered. Despite being good in theory, this practice still needs good clinical data.
Balanced transfusion is not free. Adverse events are higher with plasma and platelet transfusions than they are with PRBCs. There are clear financial costs in using additional blood products. There are the practical issues of providing multiple blood products in a timely fashion, which may needlessly complicate resuscitation if platelets and plasma turn out to be unnecessary.
Even in the observational data, there is an indication that ongoing or later treatment with platelets and plasma might be harmful. Similarly, there is an indication of harm in patients receiving higher ratios who don’t actually need massive transfusion.
I think we have already seen massive indication creep. I think every hospital now has a massive transfusion protocol. These protocols are initiated frequently, with any kind of brisk bleeding, and all of these protocols seem to be based on the 1:1:1 ratio. The result is that we are treating a large number of patients with balanced transfusions who never meet the study definitions of massive transfusion. That is concerning, considering the potential harm of added blood products, and the lack of good evidence for this practice.
Bottom line
Although it is reasonable to use a balanced transfusion strategy while waiting for more science, it is unreasonable to talk about it as a proven standard of care.
We need to be careful in our choice of language. Evidentiary amnesia leads to the repeated phenomenon of “medical reversal”, even though these supposed “reversing” studies perfectly match with the available research. Given that the only RCT ever published on balanced transfusion was negative, we shouldn’t be surprised if a future high quality RCT is also negative. (Especially when the other pilot RCT had massively worse outcomes.)
Most importantly, when we discuss medical interventions, let’s try to avoid evidentiary amnesia. Let’s openly discuss our uncertainty. I think it will help end the seemingly endless cycle of predictable ‘medical reversals’.
Other FOAMed
My comments on the PROPPR trial can be found in the Articles of the Month February 2015
Hemostatic Resuscitation with Richard Dutton:
Massive hemorrhage and emergency transfusion on Canadian Blood Services
Massive Blood Transfusion on EMDocs
References
Bhangu A, Nepogodiev D, Doughty H, Bowley DM. Meta-analysis of plasma to red blood cell ratios and mortality in massive blood transfusions for trauma. Injury. 2013 Dec;44(12):1693-9. doi: 10.1016/j.injury.2012.07.193. Epub 2012 Sep 25. PMID: 23021369
da Luz LT, Shah PS, Strauss R, Mohammed AA, D’Empaire PP, Tien H, Nathens AB, Nascimento B. Does the evidence support the importance of high transfusion ratios of plasma and platelets to red blood cells in improving outcomes in severely injured patients: a systematic review and meta-analyses. Transfusion. 2019 Nov;59(11):3337-3349. doi: 10.1111/trf.15540. Epub 2019 Oct 15. PMID: 31614006
Etchill EW, Myers SP, McDaniel LM, Rosengart MR, Raval JS, Triulzi DJ, Peitzman AB, Sperry JL, Neal MD. Should All Massively Transfused Patients Be Treated Equally? An Analysis of Massive Transfusion Ratios in the Nontrauma Setting. Crit Care Med. 2017 Aug;45(8):1311-1316. doi: 10.1097/CCM.0000000000002498. PMID: 28537938
PROMMTT: Holcomb JB, del Junco DJ, Fox EE, Wade CE, Cohen MJ, Schreiber MA, Alarcon LH, Bai Y, Brasel KJ, Bulger EM, Cotton BA, Matijevic N, Muskat P, Myers JG, Phelan HA, White CE, Zhang J, Rahbar MH; PROMMTT Study Group. The prospective, observational, multicenter, major trauma transfusion (PROMMTT) study: comparative effectiveness of a time-varying treatment with competing risks. JAMA Surg. 2013 Feb;148(2):127-36. doi: 10.1001/2013.jamasurg.387. PMID: 23560283
PROPPR: Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM, del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, Cohen MJ, Cotton BA, Fabian TC, Inaba K, Kerby JD, Muskat P, O’Keeffe T, Rizoli S, Robinson BR, Scalea TM, Schreiber MA, Stein DM, Weinberg JA, Callum JL, Hess JR, Matijevic N, Miller CN, Pittet JF, Hoyt DB, Pearson GD, Leroux B, van Belle G; PROPPR Study Group. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015 Feb 3;313(5):471-82. doi: 10.1001/jama.2015.12. PMID: 25647203
Mesar T, Larentzakis A, Dzik W, Chang Y, Velmahos G, Yeh DD. Association Between Ratio of Fresh Frozen Plasma to Red Blood Cells During Massive Transfusion and Survival Among Patients Without Traumatic Injury. JAMA Surg. 2017 Jun 1;152(6):574-580. doi: 10.1001/jamasurg.2017.0098. PMID: 28273299
Nascimento B, Callum J, Tien H, Rubenfeld G, Pinto R, Lin Y, Rizoli S. Effect of a fixed-ratio (1:1:1) transfusion protocol versus laboratory-results-guided transfusion in patients with severe trauma: a randomized feasibility trial. CMAJ. 2013 Sep 3;185(12):E583-9. doi: 10.1503/cmaj.121986. Epub 2013 Jul 15. PMID: 23857856
Nederpelt CJ, El Hechi MW, Kongkaewpaisan N, Kokoroskos N, Mendoza AE, Saillant NN, Fagenholz PJ, King DR, Velmahos GC, Kaafarani HM. Fresh Frozen Plasma-to-Packed Red Blood Cell Ratio and Mortality in Traumatic Hemorrhage: Nationwide Analysis of 4,427 Patients. J Am Coll Surg. 2020 Jun;230(6):893-901. doi: 10.1016/j.jamcollsurg.2019.10.012. Epub 2019 Nov 21. PMID: 31759164
Sambasivan CN, Kunio NR, Nair PV, Zink KA, Michalek JE, Holcomb JB, Schreiber MA; Trauma Outcomes Group; Wade CE, Brasel KJ, Vercruysse G, MacLeod J, Dutton RP, Hess JR, Duchesne JC, McSwain NE, Muskat P, Johannigamn J, Cryer HM, Tillou A, Cohen MJ, Pittet JF, Knudson P, De Moya MA, Tieu B, Brundage S, Napolitano LM, Brunsvold M, Sihler KC, Beilman G, Peitzman AB, Zenait MS, Sperry J, Alarcon L, Croce MA, Minei JP, Kozar R, Gonzalez EA, Stewart RM, Cohn SM, Bulger EM, Cotton BA, Nunez TC, Ivatury R, Meredith JW, Miller P, Pomper GJ, Marin B. High ratios of plasma and platelets to packed red blood cells do not affect mortality in nonmassively transfused patients. J Trauma. 2011 Aug;71(2 Suppl 3):S329-36. doi: 10.1097/TA.0b013e318227edd3. PMID: 21814100



One thought on “Balanced transfusion: Less evidence than you might think”
Thank you!
Don’t know if you read it, but there’s a recent bayesian post-hoc on PROPPR published in JAMA NO: 10.1001/jamanetworkopen.2023.0421
Yeah, I know, post-hoc and doesn’t overcome PROPPR inherent problems…just to let you. I declare that I always struggle to intrepret bayesian analysis.