Morgenstern, J. PACER: Prophylactic platelets before central lines, First10EM, September 4, 2023. Available at:
https://doi.org/10.51684/FIRS.131393
There is an odd paradox in medicine: our sickest patients are in the most need of intervention, but they are also the most likely to have complications from those interventions. (This is why I have always opposed the “kitchen sink” philosophy, in which we throw everything at an apparently dying patient. That philosophy assumes that what you are throwing provides more benefit than harm, but if you wouldn’t use the treatment in a healthier population because of lack of proven benefit, you shouldn’t use it in the sickest patients, where harms are likely to be even higher.) When it comes to procedures like central lines, the patients who need them are more likely than the average patient to have coagulopathies which increase their risk. The PACER trial looks at the role of prophylactic platelet transfusion prior to central venous catheter (CVC) placement.
The paper
The PACER trial: van Baarle FLF, van de Weerdt EK, van der Velden WJFM, et al. Platelet Transfusion before CVC Placement in Patients with Thrombocytopenia. N Engl J Med. 2023 May 25;388(21):1956-1965. doi: 10.1056/NEJMoa2214322. PMID: 37224197
The Methods
This is a multicenter, randomized, controlled, noninferiority trial at 10 hospitals in the Netherlands.
Patients
Patients with severe thrombocytopenia (platelet count, 10,000 to 50,000 per cubic millimeter) who were being treated on the hematology ward or in the intensive care unit and required a CVC. Exclusions: Therapeutic anticoagulant, coagulation factor deficiency, INR 1.5 or higher.
Intervention
Prophylactic platelet transfusion (one unit of platelet concentrate) prior to ultrasound guided CVC placement.
Comparison
No platelet transfusion prior to ultrasound guided CVC placement.
Outcome
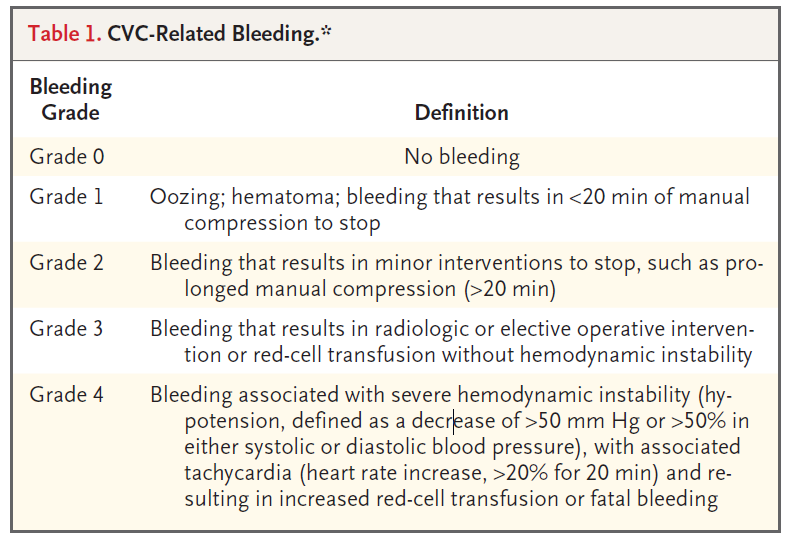
The primary outcome was catheter-related bleeding (grade 2-4). A noninferiority margin was set at 2.5%.
Physicians in both groups had to have placed at least 50 central lines previously.
The Results
They included 373 CVC placements among 338 patients. The median platelet count was 30,000. About 50% of lines were placed in the IJ, and 40% subclavian.
They were unable to demonstrate noninferiority, with 4.8% of the transfusion group and 11.9% of the no-transfusion group having grade 2-4 bleeding after CVC placement (ARR 7.1%, 90% CI 1.3-17.8%). In fact, although this is how they phrased their results, they actually demonstrated that prophylaxis is superior. (More on these distinctions in an upcoming post on the ins and outs of noninferiority trials.)
There were no grade 4 bleeds in the trial. Grade 3 bleeds followed the same trend as the overall bleed rate, with 2.1% in the transfusion group and 4.9% in the no-transfusion group.
There were 2 allergic transfusion reactions in the transfusion group as compared to 1 in the no transfusion group. There was one case of acute lung injury in the transfusion group.
My thoughts
I really like this study, because it is the kind of clinical question we often try to address using observational data. Having an RCT is incredibly valuable, and the fact that this is a well done multicenter RCT, with a pre-published protocol, excellent follow-up, and very few protocol violations is fantastic.
Unfortunately, this trial was open-label, and there was really no reason for that. It feels like a very easy intervention to blind. Worse, the physicians were aware of the purpose of the trial, and the outcome is pretty subjective. Furthermore, when you know your bleeding rates are being monitored, you might be far more careful in your procedural technique than you usually would be (the Hawthorne effect). Thus, instead of a near perfect study, which would have settled this issue nicely, we are left with a lot of uncertainty.
Furthermore, although the study was probably powered appropriately for the bleeding events, it is much to small to assess the harms of platelet transfusions. It only takes a few cases of acute lung injury to completely overwhelm the benefits of reduced minor bleeding, because minor bleeding is easily controlled with local pressure (even if it takes a lot of clinician time). We will need a much larger study to compare the real harms of transfusion again the true complications (bleeding significant enough to have patient impact).
It is also worth noting that this study has a very high bleed rate, even compared to other thrombocytopenia literature. That might be explained by a more rigorous documentation of bleeding, but it makes extrapolation somewhat difficult.
Finally, different guidelines have suggested prophylaxis at different levels, anywhere between 20 and 50,000. This trial doesn’t clarify those levels, and the data is not granular enough to assess the risk at the higher end (for example, the patients with platelet levels between 40 and 50,000, who some people might not be transfusing based on current guidelines).
Bottom line
This is a well done (although far from perfect) RCT that demonstrates better outcomes with platelet transfusion prior to CVC placement in patients with platelet counts between 10 and 50,000. Based on this study, I will aim to provide a prophylactic platelet transfusion for patients with thrombocytopenia and platelet counts less than 50,000 per mm3. That being said, neither hospital I work in has platelets on hand, so there I will need to continue to assess the urgency of the CVC against the risk of performing the procedure prior to the platelets arriving (which usually takes a few hours).
Other FOAMed
Platelet Transfusion before CVC Placement in Patients with Thrombocytopenia on The Bottom line
References
van Baarle FLF, van de Weerdt EK, van der Velden WJFM, et al. Platelet Transfusion before CVC Placement in Patients with Thrombocytopenia. N Engl J Med. 2023 May 25;388(21):1956-1965. doi: 10.1056/NEJMoa2214322. PMID: 37224197
Photo by Diana Polekhina on Unsplash




4 thoughts on “PACER: Prophylactic platelets before central lines”
Just a small point (and maybe I’m focusing on the introduction as we don’t do CVKs in Scandinavia as ED docs)
“our sickest patients are in the most need of intervention, but they are also the most likely to have complications from those interventions”
Can’t help thinking about Gilbert Welch’s “Overdiagnosed” book and the spectrum of illness severity-graph that he draws (https://m.youtube.com/watch?v=QzQxv4bFUds ) and how benefit and harms from treatment have different curves
He would argue that (paraphrasing) , “while we don’t know the exact slope of the harms-curve, the benefit-curve is way more steep than the harms curve” . In the graph it’s benefit going up and harms stable (wiggling to indicate minor up- or downsloaping)
Of I’m extrapolating his book on mainly chronic illness with acute illness , but as you’ve written / talked on the topic of overdiagnosis before , I thought it may be something to think about
I don’t have an answer either and I know for some conditions like trombolytics for PE or stroke it’s less dangerous to give to someone with no / mild disease than someone with severe disease (implying that the harms-curve may very well be upsloping for some conditions at least)
So our sickest patients may very well be the ones to have highest risk of complications but it’s important to think about the curves and their slopes . Quiet possibly the benefit-curve is more steep than the often less inclining harms-curve
It could be argued that the kitchen sink approach (if treatments are aimed at the right disease process) may have a more favourable benefit-harm ratio in the severely sick , than someone who’s not .
However so many other factors goes into decision making in the critically Ill patient and at that point a more iterative hypothesis testing approach would probably be better than a less flexible one
Thanks again for all your work !
All the best
Peter
I have used and reflected on those harm benefit curves a lot in the past. I think the problem with the standard curves is that they fail to reflect the non linear nature of harms in the critically ill. Critically ill patients have very little physiologic reserve. A small GI bleed or a small pneumothorax, which may be inconsequential in an outpatient, could be the difference between life and death in the critically patient. I think iatrogenic harms have been overplayed in medicine in general, but among the critically ill, I think they are likely overplayed, because when the kitchen sink actually kills the patient, it is easy to rationalize that the patient was going to die anyway. So I don’t think it is easy to extrapolate those same curves to the sickest patients. (Of course, this is all theoretical. I really appreciate the comment. Important stuff to be reflecting on.)
I’m surprised at the high amount of subclavian lines, as my teaching was this is non compressible, if bleeding occurs.
Hey Justin,
Great review as always…a few thoughts from me…
1. The 1st question I ask is does the patient need emergent vascular access…if the answer is yes there may not be time to give platelets regardless of platelet count. I would try to get US guided PIV, PIV, or IO 1st as this may buy some time for platelets to be initiated
2. If patient needs emergent access and PIV or IO not possible then no platelets…obviously use the US, Do IJ or Femoral (compressible sites), and consider doing micro puncture access to improve visibility of needle going into vessel
3. It seems from the details of the study the highest risk of bleeding was in patients with platelet counts <30k, hematology/oncology patients, and patients with hemodyalsis and tunneled catheters…these are the patients I would consider platelet transfusion on
4. Finally, not all low platelet counts are the same…it depends on whether there is a consumptive platelet process or dysfunctional platelet process going on. You could have a patient with 40k platelets with completely functional platelets but could also have a patient with 60k platelets with completely dysfunctional platelets
This is what I took away from the study…
-Prophylactic platelets for patients with <30k platelets, hematology/oncology patients, dialysis/tunneled catheters
-No Prophylactic platelets for patients in the ICU (They have a lower bleeding risk due to consumptive process as apposed to dysfunctional process & better monitoring), emergent vascular access needed
-As you stated there was a very high bleeding rate in this trial, I suspect due to better reporting, but the rate was even high in the patients that got 1U of platelets. Future trials should consider maybe even 2U of platelets as 1U may not have been enough
Always enjoy reading your breakdowns and hope this helps others reading this post
Salim