
I will preface this COVID research roundup edition with the warning that we are making many decisions based on very weak science. I generally don’t include that many really weak studies in these write-ups, unless they are really entertaining. However, when searching for scientific answers to my questions about COVID, that was often the best I could find. I will also say that new publications are coming out at an astounding rate, and even with the amount of time I spend reading every day, I cannot keep up. Some of this information could be out of date by the time you read it. That being said, this is a collection of studies that I found interesting and helped answer some of my many questions about COVID-19.
I am not going to include any of the papers that describe the basic clinical course or management of this disease. At this point, you would have to be a hermit not to have heard those details, but if you want a refresher, you can check out the amazing summaries on REBEL EM or The Internet Book of Critical Care.
The podcast version of this post can be found here, or just listen below:
Some infection control stuff
COVID will cover all room surfaces, but cleaning works
Ong SWX, Tan YK, Chia PY, et al. Air, Surface Environmental, and Personal Protective Equipment Contamination by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) From a Symptomatic Patient JAMA. 2020; [article]
This is a very small sample, but provides some useful insights into COVID transmission. They swabbed surfaces in the rooms of 3 COVID patients. After cleaning (with sodium dichloroisocyanurate if you are interested), none of the surfaces were positive for COVID. Before cleaning, 87% of the surfaces samples were positive. However, despite widespread surface contamination, when they took swabs of PPE used in the room, only 1 of 10 was positive (on a shoe cover), and none of the surfaces in the anteroom or hallway were contaminated, so their practices seemed to work. Air samples were also negative. It is worth noting, positive samples were based on PCR and don’t mean live virus was present, and don’t tell us the likelihood of clinical infection. In fact, the amount of virus found at all locations was so low that infection is unlikely. However, these were not critically ill patients, so high risk, aerosol generating procedures were not being performed.
Bottom line: This very small study indicates that routine cleaning practices and PPE are likely sufficient for COVID well patients.
COVID will survive on surfaces
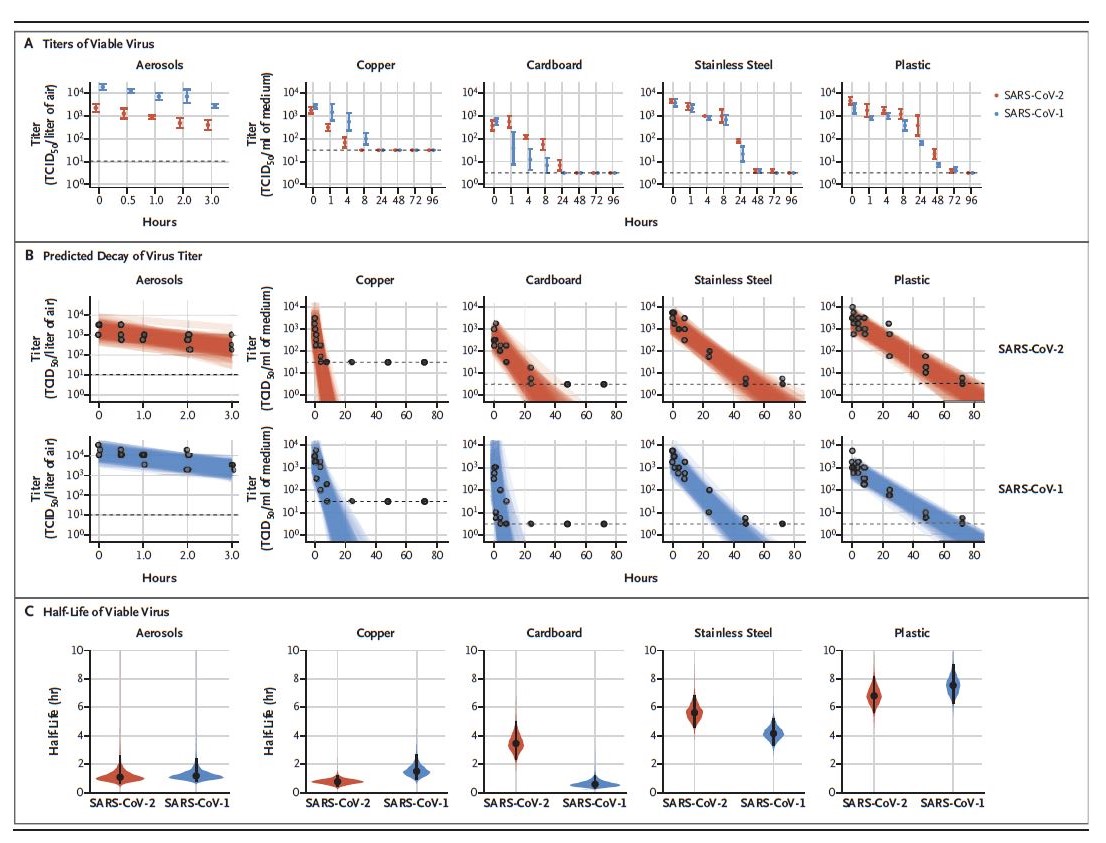
van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1 [published online ahead of print, 2020 Mar 17]. N Engl J Med. 2020;10.1056/NEJMc2004973. PMID: 32182409
In this research letter, they describe an experiment where they sprayed a bunch of SARS-CoV-1 and SARS-CoV-2 into the air and onto stuff. SARS-CoV-2 (COVID 19) remained viable in aerosols for the full 3 hours that they tested. We have no idea how long it would have lasted after that, because they didn’t test. The half life looks to be just over 1 hour, so the aerosol probably remains viable in the air for up to 5 hours. Given that these aerosols were artificially generated, it isn’t clear how this translates into clinical practice. It remained viable for more than 72 hours on stainless steel and plastic, 24 hours on cardboard, and 12 hours on copper.
Bottom line: Wear your mask and wash your hands after you touch anything. Hopefully that isn’t news to anyone.
What exactly are aerosol generating procedures?
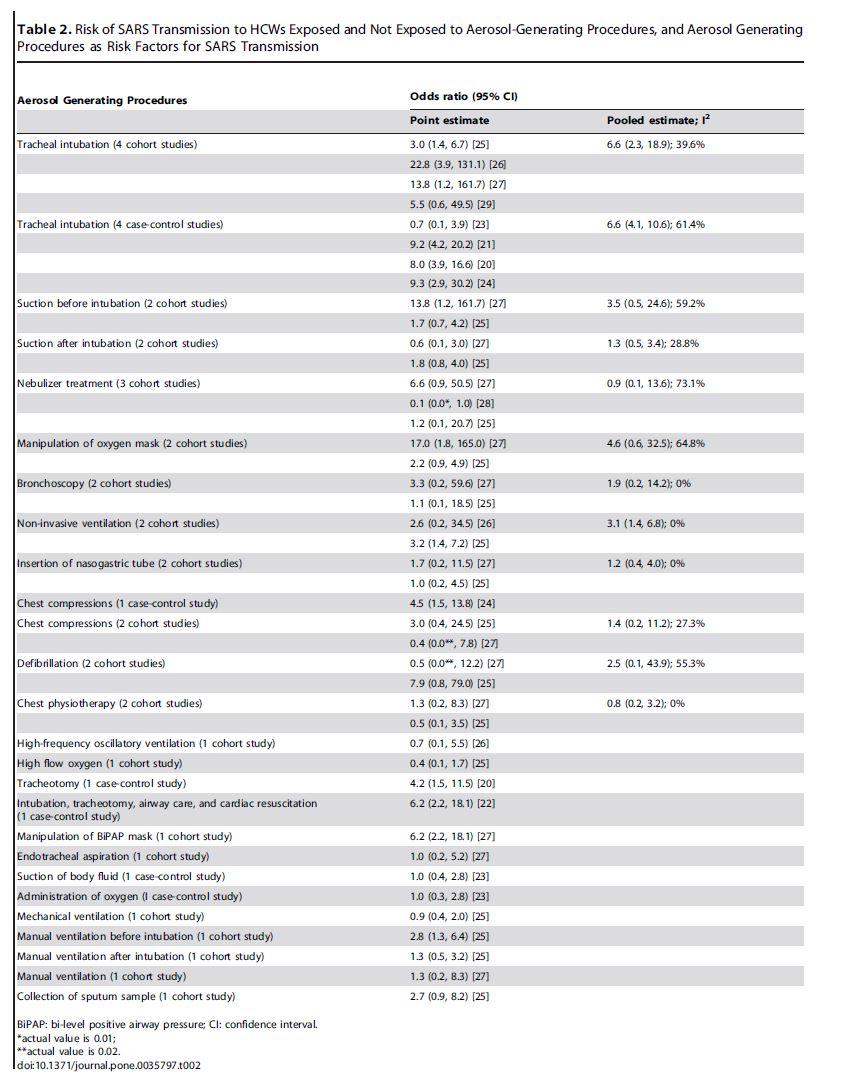
Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. PMID: 22563403
Obviously, there has been a great upheaval in resuscitation recently, in large part based around what we consider to be aerosol generating procedures. We clearly want to avoid transmission of COVID to healthcare workers. However, there are harms that come from getting this wrong, especially if we needlessly avoid treatments that could help our patients. This is a systematic review and meta-analysis that looked for studies comparing respiratory infection rates among healthcare workers exposed to an aerosol generating procedure compared to controls who were not. (Obviously, none of these studies were randomized, so there are almost certainly confounders that make the data less reliable.) They found 10 studies, 5 of which were case-control studies, and the other 5 were retrospective cohorts. All 10 looked specifically at SARS-CoV. Four were from Canada, 1 from Singapore, and 5 from China. Unfortunately, the data is inherently weak and most of the confidence intervals are really big. Intubation was a significant risk for transmission of SARS, with an odds ratio of around 7. Noninvasive ventilation (OR 3.1), tracheostomy (OR 4.2), and manual ventilation before intubation (OR 2.8) were all also associated with risk, but those numbers are based on 2, 1, and 1 studies respectively. Furthermore, the various procedures are intimately connected and hard to tease apart. How do you know if the clinician was infected while bagging before intubation, or during intubation itself? Interestingly, manual ventilation on its own was not associated with increased risk. Although nebulization was also not associated with increased odd ratio, the data sounds very complicated. One trial actually claims it was protective (OR 0.1), and I am not sure how that is even possible. Two other trials show risk. I will try to look at those studies myself and update you when I can, but the conflicting numbers really underline the problems with the data itself. Other procedures that were not associated with increased risk were administration of oxygen and high flow oxygen. Perhaps the biggest weakness in all this data is we have no idea what PPE was used by the providers that were infected, and whether it was used correctly. There are many reports on the SARS experience, and many of the clinicians who were infected during procedures like intubation were not wearing what we would consider to be appropriate PPE. Ultimately, given the weakness of the clinical data, we are left making extrapolations from basic science as to how far droplets and aerosols move and how long they last, but unfortunately that data is also sparse.
Hui DS, Chan MT, Chow B. Aerosol dispersion during various respiratory therapies: a risk assessment model of nosocomial infection to health care workers. Hong Kong Med J. 2014;20 Suppl 4:9–13. PMID: 25224111
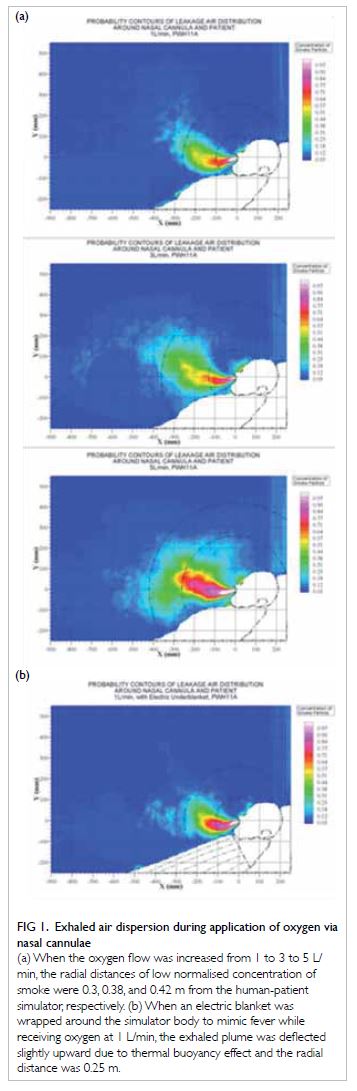
Speaking of basic science, let’s look at some. This is a study that uses a high fidelity simulator to simulate patient breathing, and then uses laser light to measure exhaled smoke particles to measure how far they went. They used this technique to compare a number of different respiratory therapies. On nasal prongs, exhaled smoke made it about 30 cm from the patient’s mouth. With a nonrebreather, it was 10 cm. With noninvasive ventilation, depending on your settings and the exhalation port used, it was between 40 and 100 cm. With a nebulizer, it was between 45 and 80 cm, depending on the degree of lung injury simulated. For the most part, they were just looking at exhalation here, not coughing or sneezing. They only tried coughing with a standard Hudson mask. Air comes out laterally (around the edges of the mask) about 20 cm with normal breathing, and beyond 40 cm with any coughing. When they didn’t have adequate ventilation in the room, smoke quickly filled the room and they couldn’t take measurements. Based on that result, they suggest you want a room that cycles the air 12 times an hour. In my mind, because they weren’t looking at real patients, or consistently simulating coughing or sneezing, the real value in these numbers is not the absolute numbers, but their relative numbers. Higher flows spread things further than lower flows. Open systems like nasal prongs result in more spread than a covered system like a nonrebreather. The numbers will be significantly bigger when looking at coughing or sneezing patients. That being said, these numbers are at least pretty reassuring when we are assessing patients in droplet precautions, or removing our PPE more than 2 meters from a patient.
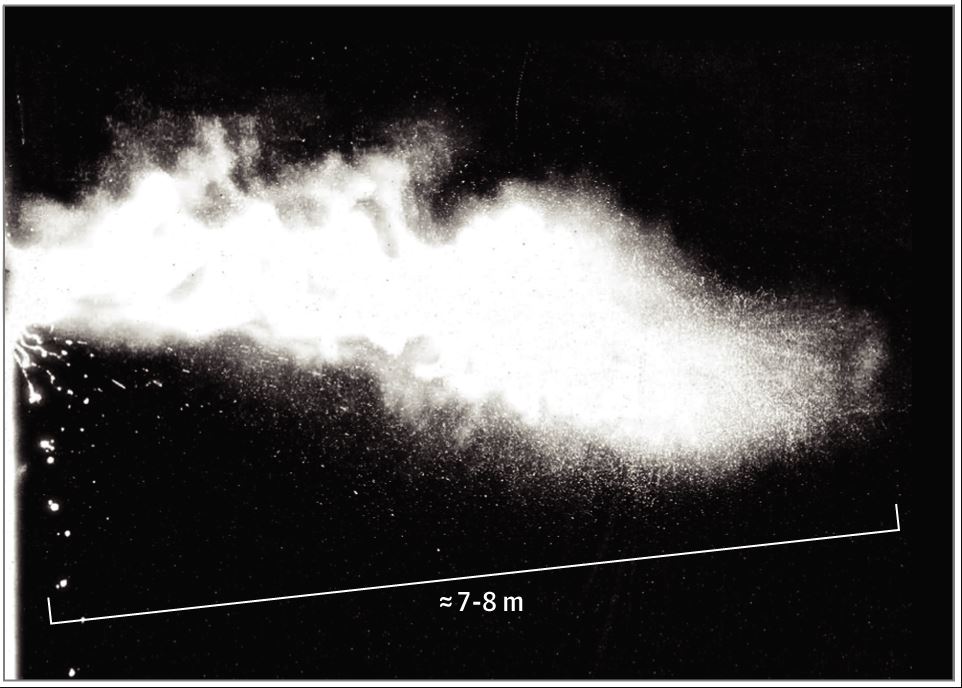
Bourouiba L. Turbulent Gas Clouds and Respiratory Pathogen Emissions: Potential Implications for Reducing Transmission of COVID-19 [published online ahead of print, 2020 Mar 26]. JAMA. 2020;10.1001/jama.2020.4756. doi:10.1001/jama.2020.4756 PMID: 32215590
This editorial acts as a bit of a rebuttal to the reassuring numbers in the last paper. The author argues that our current division into droplet and aerosol spread is antiquated, because it doesn’t account for the turbulent nature of sneezing and coughing. She presents data that pathogen bearing droplets of all sizes can be spread up to 7-8 meters (or 23-27 feet) after a sneeze. She references the study by Ong discussed above, where SAR-CoV-2 particles were found in ventilation systems, as more consistent with turbulent flow then our standard theories. She argues that the current advice for separation (1 m according to the WHO or 2 m according to the CDC) may be significant underestimates. There is a video of this turbulent cloud as part of the original article. There are some major limitations to this article. It is not a systematic review, so we are not presented with potentially conflicting data. More importantly, there is a difference between being able to detect particles from a sneeze up to 7 meters from the patient and those particles actually being infectious. It is possible that once you get beyond the 1-2 meters we currently use as cutoffs, the amount of virus spread is negligible. There are lots of very smart people working at the CDC and the WHO where those recommendations come from. However, every specialty has it’s evidence based medicine blind spots. I have been searching high and low for data on this issue for weeks, and I am still unsure how important this extra spread is, or how much to trust the 2 meter cutoff we currently use.
Overall, I still have a lot of droplet versus airborne questions. Unfortunately, there is not a lot of great clinical data. We are primarily making guesses based on basic science papers like the ones above. Although I think it is clear that some droplets will make it well beyond the 2 meter cut-off, it isn’t clear how much virus makes it that far, and what the real risk of transmission might be. There is a long list of papers that I am working my way through, and this topic will almost certainly get its own blog post when I can find time. In the meantime, there is a very interesting episode of the Epidemic podcast with Dr Celine Gounder (an ID doc and journalist) entitled “A False Dichotomy: Airborne versus Droplet”.
Clinical Assessment
The Roth Score
Chorin E, Padegimas A, Havakuk O, et al. Assessment of Respiratory Distress by the Roth Score. Clin Cardiol. 2016;39(11):636–639. doi:10.1002/clc.22586 PMID: 27701750
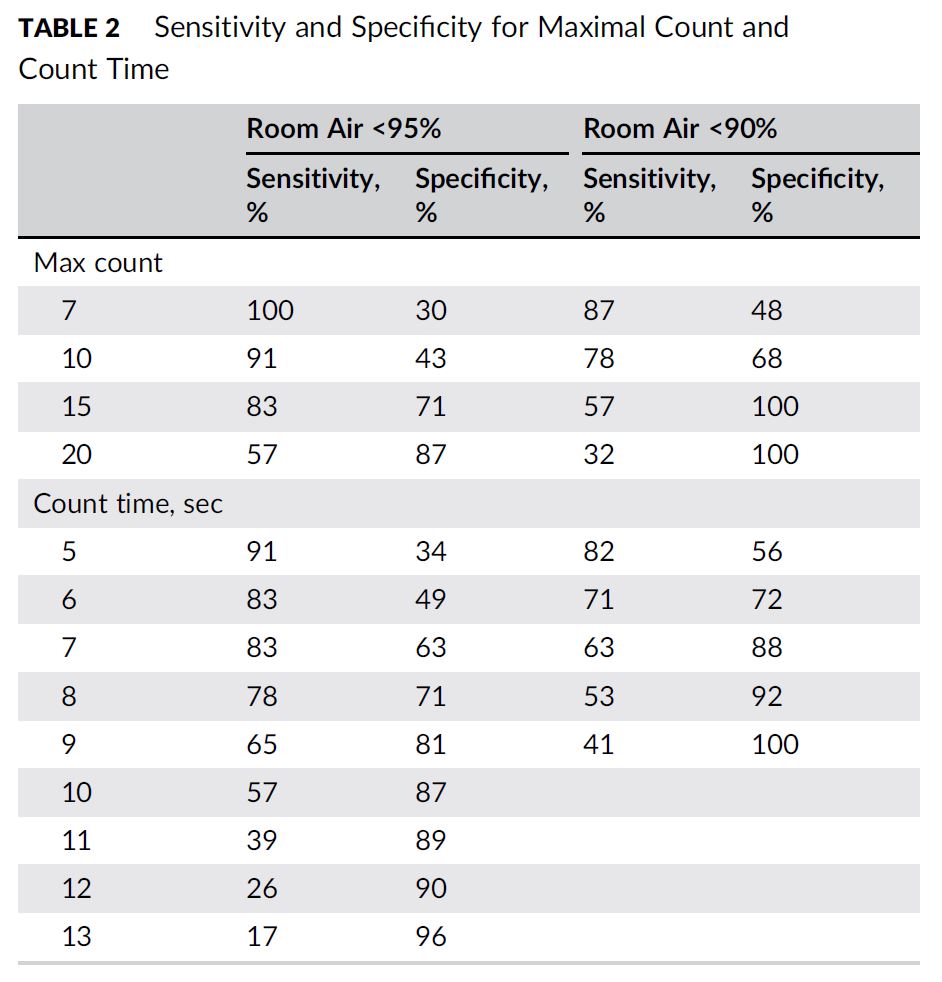
This is an interesting little study that has made the rounds on social media. They assessed 93 patients who were admitted to a single hospital in Israel and who required between 2 and 6 L/min of oxygen by nasal prongs. They were assessing a test which involved having the patient take a deep breath and then count from 1 to 30 in their native language as fast as they could. They measured two variables: the highest number they could get to in a single breath and how long it took them to get to that number. Patients were a mean age of 76, and admitted for CHF (25%), pneumonia (17%), ACS (15%), and a variety of other illnesses causing dyspnea. The test was good, but obviously not perfect for detecting hypoxia. Looking specifically at patients with a room air saturation less than 90%, the area under the curve was 0.84 for maximal count number and 0.81 for count time, which isn’t bad. The sensitivities and specificities are in the table below. Unfortunately, if you are going to use a test to avoid something that is part of standard care, you really want to see a high sensitivity. This test would miss 18% of patients with an oxygen saturation less than 90% if you used the time of 5 seconds and 13% if you used the maximal count number of 7. There was a mix of medical conditions here, and I bet this test works better in some than others. (It is likely to be more sensitive in diseases causing significant respiratory muscle fatigue, like COPD, than it is in something like PE.) Overall, they pitch this as a tool for telemedicine, when our normal vital sign machines are not available, and I think it is fine as an added data point. However, in the hospital we really should be able to get oxygen saturations. (If you don’t want to have to suit up to go into the room every time to measure one, make some signs and teach the patients to measure their own sats.)
Bottom line: I can’t see myself using the Roth score in the hospital, but maybe I will see how it works the next time I am called to an emergency on an airplane (right before I pull out the portable pulse ox I generally carry around with me.)
Some treatment stuff
Chloroquine is probably not a miracle cure
Gautret P, Lagier J, Parola P, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. International Journal of Antimicrobial Agents. 2020; [article]
PLEASE NOTE: This trial has since “received a statement of concern”, as the journal says it “does not meet the [International Society of Antimicrobial Chemotherapy’s] expected standard”
This is the “big study” that got president Trump all excited last week. It is an observational study of patients 12 years and older with documented COVID-19, admitted to a single hospital in France, with a control group from other hospitals around France. The patients were pretty healthy, with only 20% having pneumonia, and 17% being asymptomatic. At the single primary centre all patients were given oral hydroxychloroquine 200 mg three times a day. Patients at the other centers did not receive hydroxychloroquine. (This is clearly not an ideal control, as there are lots of reasons that care might differ between hospitals, especially when one of those hospitals is organizing a trial, while the others aren’t.) They originally enrolled 42 patients. However, 6 were excluded from the main site, mostly because of death or transfer to the ICU, while no patients were excluded from the controls. This means the sickest patients were excluded from the treatment group, so we should expect better outcomes in the treatment group. Many of the control group patient didn’t have a quantitative swab at the start of the trial, and they were swabbed less often than the treatment group. Their primary endpoint was viral clearance on day 6, which occured in 70% of the treatment group and 13% of the controls (p=0.001). Some patients also happened to get azithromycin, and those patients happened to have 100% viral clearance on day 6.
This study is a bit of a mess, and clearly should not drive clinical practice. It is the kind of study we wouldn’t even notice in normal times, but the pandemic is causing people to throw out scientific principles. This is an observational trial with significant sources of bias. It doesn’t assess any patient oriented or clinical outcomes. And it doesn’t look at the group of patients we are most concerned about (they included asymptomatic patients here). At best, this is an association at high risk of bias. The study raises a hypothesis. When combined with other data, it might be reasonable to proceed with an RCT, but based on historical examples, changing clinical practice at this point is more likely to do harm than good. With regards to azithromycin, the results are so weak I am not sure it’s even worth considering it a hypothesis.
Paper #2: Gautret P, Lagier J, Parola P, et al. Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: an observational study. Prepublished online
There is a follow up study from the same group. I don’t believe it is published in a journal yet, but it is available online here. This is even lower quality evidence than the last paper, because they don’t include a control group. They just tell us about 80 COVID-19 patients in whom they gave a combination of hydroxychloroquine and azithromycin.They did include some of the same patients as the first paper. The patients are young (median age 52), and sound relatively healthy, with only half having lower respiratory tract involvement, only 15% being febrile, and 94% having a low NEWS score. Despite that, only 81% have a “favourable outcome” at the time the paper was written up. One patient was admitted to the ICU and 1 patient died. Without a control group, it is impossible to know what this data means, but overall those numbers don’t sound good, and could easily be consistent with this treatment combination harming patients rather than helping them.
Bottom line: There is no role for chloroquine, hydroxychloroquine, or azithromycin in the management of COVID-19 yet. It is best to wait and see the results of the RCTs.
Neither is Lopinavir-Ritonavir
Cao B, Wang Y, Wen D, et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19 [published online ahead of print, 2020 Mar 18]. N Engl J Med. 2020;10.1056/NEJMoa2001282. PMID: 32187464 [open access article]
This is a single-center open-label RCT from Hubei, China. (They did not create placebos because of the speed with which the trial was put together.) They included adult patients with a positive PCR for COVID-19, pneumonia on chest x-ray, and an oxygen saturation of 94% or less on room air (or a PaO2:FiO2 <300). Physicians were allowed to exclude patients from the trial if they thought “it was not in the patient’s best interest”, which introduces possible selection bias, but they did use an appropriate allocation concealment procedure. They compared lopinavir-ritonavir (400 mg and 100 mg by mouth twice daily for 2 weeks) to standard care. They assessed patients using a 7 category scale:
- Not hospitalized, with resumption of normal activities
- Not hospitalized, but unable to resume normal activities
- Hospitalized, not requiring oxygen
- Hospitalized, requiring oxygen
- Hospitalized, requiring high-flow nasal oxygen, noninvasive ventilation, or both
- Hospitalized, requiring ECMO, mechanical ventilation, or both
- Dead
They included 199 patients, of whom 95% actually received the assigned treatment. The median age was 58, 60% were males, and the median time interval between symptom onset and randomization was 13 days. This was a very sick group, with a 22% mortality rate overall. For their primary outcome, the time until the patient improved by 2 points on that scale or were discharged from hospital, there was no difference at all. The median time to improvement was 16 days in both groups. There was also no difference in time to deterioration (HR 1.01; 95%CI 0.76-1.34). There was no statistical difference in mortality (19.2% vs 25.0%, ARR -5.8%, 95% CI -17.3 to 5.7%). Although this is not statistically significant, a lot of people have looked at the absolute difference here and become excited. I think there may be some leeway in what stats we should require in a pandemic (if we required a 5,000 person trial, it might not be completed until the pandemic was over), however, there are multiple methodologic problems with this trial, so I think it is difficult to put too much faith in this number. Furthermore, the stats say that this finding is consistent with lopinavir-ritonavir increasing mortality by 5.7%. There was also a borderline statistical decrease in ICU length of stay (6 vs 11 days, ARR -5 days, 95% CI -9 to 0 days). However, it isn’t clear to me how that is possible, when the primary outcome includes the things that would have kept these patients in the ICU and was negative. More importantly, the difference in length of ICU stay was only found among the patients who died, so it isn’t actually a very good surrogate for anything. As an interesting note, virus RNA was still detected in 41% of the patients at the end of the trial (28 days), and they say they didn’t find any significant antiviral effect from the antiviral medication. There are a number of issues with this trial. It was unblinded, and the primary outcome is only quasi objective. They adjusted their sample size on the fly. Now, it is very difficult to decide on a sample size when very little is known about a disease, so we need to give them some leeway, but they did change their sample size partway through, and then just decided to stop the study not because they reached a new sample size, but because there was a new agent available to test (remdesivir) that they were more excited about. Perhaps the biggest concern here may be the timing of therapy. This will be an issue for all antivirals. Patients weren’t treated until 13 days into their course. At the point, viral replication is not the major physiologic issue (we believe patients are experiencing cytokine storm at this point), so it isn’t clear that we should expect an antiviral to work. However, if we give the antivirals earlier we will have to treat a lot of patients who were never going to get severely ill, and the harms will probably outweigh the benefits.
Bottom line: All that was a very long way of saying there is no cure for COVID-19. This was a negative trial. The reduction in mortality cannot be trusted. Although it should provoked more research (already underway), this is not a drug we should be using clinically at this time.
You can read more about this study on REBELEM and PulmCrit
I wanted to include a trial on remdesivir, because everyone is talking about it, and people are clamouring to get it from Gilead, but there is not a single clinical trial looking at this drug in humans. There is no evidence that it works. You can read about the lack of evidence for all the antivirals in this post.
Kalil AC. Treating COVID-19-Off-Label Drug Use, Compassionate Use, and Randomized Clinical Trials During Pandemics [published online ahead of print, 2020 Mar 24]. JAMA. 2020;10.1001/jama.2020.4742. doi:10.1001/jama.2020.4742 PMID: 32092748
I thought I would throw this editorial in here. It cautions us against conducting trials without control arms, because we are unlikely to gleen any valuable information from them. When patients die, we blame the disease, and when patients live, we tend to credit the treatment, biasing our thinking and ignoring the natural history of the disease. The editorial also cautions us against giving drugs “as a last resort”, because it wrongly assumes that the patient is more likely to benefit than harm (when in fact the opposite is probably true). I think those are important lessons from this COVID-19 therapeutics section.
Some PPE stuff
The big question: N95 or surgical mask?
Long Y, Hu T, Liu L, et al. Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta‐analysis J Evid Based Med.. 2020; [article]
The N95 versus surgical mask controversy looms large over many COVID discussions. Unfortunately, this paper is unlikely to be completely satisfying, but it probably represents the best summary of the evidence that we have. It is a systematic review and meta-analysis of studies comparing N95 and surgical masks in influenza. (So, our first problem is we have to extrapolate from influenza to COVID-19, because there isn’t good data available for this virus.) They found 6 RCTs, with sizes ranging from 435 to 5180 participants, so the total sample size is 9171. Although that sounds reasonably big, you have to remember that the power of a study comes from the number of events, not just the number of people included, and few people wearing masks should get sick. More importantly, the systematic review doesn’t give us a lot of the details that we would want about these studies, like how compliant were people with mask wearing, what was the total time spent in masks, how good were people with hand washing, what was the total time spent with patients, were they performing any high risk (aerosol generating) procedures, etc. They looked at a number of different outcomes, and didn’t find any statistically significant differences. However, the confidence intervals are pretty big, and the point estimates suggest N95s might be better. For example, 5 studies report influenza like illness as an outcome, and there is no statistical difference, but the relative risk is 0.61 favouring N95s, with a 95% CI from 0.33 to 1.14. I think the huge range tells us that we simply don’t know. They mention increased discomfort with N95 masks, and therefore prior research that indicates that people are less compliant with wearing N95 masks. They don’t report it here, but if compliance was an issue, that could bias the trials towards no effect. However, I don’t think compliance is going to be much of an issue over the next couple months. They also note that N95 masks were specifically designed to keep particles out, while surgical masks were actually designed to keep particles in (to protect the patient from the surgeon). In the ideal world, I think using N95s makes sense. The problem is, if you use them for low risk patients (with no aerosol generating procedures) now, there is a very high likelihood that you will be faced with seeing high risk patients with no N95s available in a few weeks. The difference in risk, if there is one, appears small, and so I think the current protocols are logical. As a side note, does anyone find it odd that the medical standard is an N95, which literally means it is designed to keep 95% of particles larger than 2.5 microns out, when there is such a thing as an N99 mask or N100 mask. Wouldn’t we prefer to filter 99% or 99.97% of the particulate matter out? And yet, I have never heard of these higher forms of protection being used in medicine.
Bottom line: We really don’t know what mask is best for the COVID pandemic. I will continue to use an N95 for all high risk encounters, but am happy to use a surgical mask (with face shield) when assessing lower risk patients.
But we are running out of masks. Can we make our own?
MacIntyre CR, Seale H, Dung TC, et al. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ Open. 2015;5(4):e006577. Published 2015 Apr 22. doi:10.1136/bmjopen-2014-006577 PMID: 25903751 [free full text]
As jurisdictions around the world have run out of PPE, we have seen heartwarming grassroots campaigns to protect our healthcare workers. One example has been people sewing masks at home to be used in hospitals, but are those masks any good? This is an interesting cluster randomized trial in which the healthcare workers on 74 wards considered to be high risk for respiratory infections (ED, ICU, pediatrics, and respiratory) were randomized to either wearing a medical mask at all times, wearing a cloth mask at all times, or standard practice. This took place in Vietnam, and they note that standard practice often involves very frequent mask use. People were excluded if they had beards, long mustaches, or allergic rhinitis. They had the health care workers wear the masks at all times during their shifts for a 4 week period, and then followed them for another week to catch respiratory illnesses. In the medical mask group, clinicians were given 2 masks per shift. In the cloth mask group, clinicians were given 5 masks in total and given instructions on how to wash them. Unfortunately, the study has 3 primary outcomes (you are only allowed to have one) and did not adjust for multiple comparisons. They looked for clinical respiratory illnesses, influenza like illnesses, and laboratory confirmed viral respiratory infection. On average the healthcare workers saw 36 patients a day. (The range was 0 to 661. We need to pause there for a second. How the hell does a healthcare worker see 661 patients in a day? Even if you were a triage nurse, that would have to be at the busiest emergency department in the world. Also, how does someone get away with seeing 0 patients on a clinical shift?) The rate of influenza-like illness was higher in the cloth mask group than the medical mask group (RR 13.25, 95% CI 1.74-100) and maybe the control group (RR 3.49, 95% CI 1.0-12.17). All of the other outcomes were also higher in the cloth mask group, but not statistically so. They did also test the masks themselves, and the cloth masks let through almost everything (97% of particles) while the medical masks blocked 56% (but n95 masks they tested blocked more than 99.9%). There are some issues that make this trial harder to interpret. A large number of the control group wore masks, although they did so for about half the total time of the test groups. Also, although they were supposed to wear masks at all times, both mask groups only wore their mask about 55% of the time. They did not directly measure hand hygiene, but it is very disturbing that these healthcare providers only report washing their hand 11-14 times when they are seeing 36 patients a day! There was no circulating RSV or influenza at the time of the study, which could affect the results, especially considering only 3% of these healthcare workers were immunized against the flu. They do note 2 other studies with similar results.
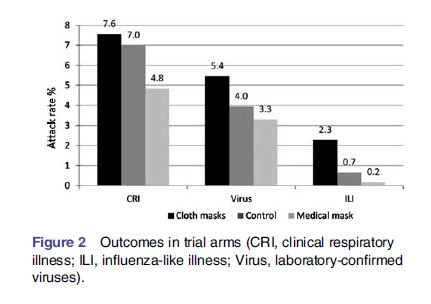
Bottom line: Only 2 of the 6 primary outcome comparisons were positive, and there were some issues with the trial. I don’t think the data definitively says the cloth masks are worse (and there are lots of different materials out of which you could make a cloth mask). However, all of the outcomes were on the side of cloth masks being worse, and you certainly can’t use this data to conclude they are safe either. Looking at this trial, I certainly wouldn’t wear a cloth mask during the COVID-19 pandemic.
Ibuprofen
Fang L, Karakiulakis G, Roth M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? [published online ahead of print, 2020 Mar 11]. Lancet Respir Med. 2020;S2213-2600(20)30116-8. doi:10.1016/S2213-2600(20)30116-8 PMID: 32171062
I wanted to include a paper that explained the whole ibuprofen fiasco, but it turns out, there is no clinical data at all. There may have been a few unofficial case reports, but it is hard to tell. Most media outlets say that some young patients died after “taking massive doses of ibuprofen”. If that is the case, I think we would blame the massive dose and not the ibuprofen. There were some rumours about 4 young patients who died of COVID-19 and had taken ibuprofen. Aside from the fact that those cases have never been officially reported, the bigger problem is that the reports are rather meaningless. You have to consider a control group. Sure, young people who died of COVID took ibuprofen, but I can almost guarantee you that so did all the young people who survived. Ibuprofen is what you take when you are sick and have headaches and myalgias. I doubt there was even a correlation. So why is this entire paragraph under a letter to the editor written about diabetes and hypertension? In this theoretical paper about the role of the ACE2 receptor in COVID-19, they include a single sentence that states that there may be upregulation of the ACE2 receptor in people taking ibuprofen (although there is no citation, so we don’t know how much ibuprofen you might have to take, or for how long, or whether this is theory or fact).
Bottom line: I would still take ibuprofen if I was sick and needed analgesia. I never treat fever for fever’s sake so I don’t have to worry about that. Although adverse events are rare with both drugs, starting with acetaminophen might make sense.
Palliative Care
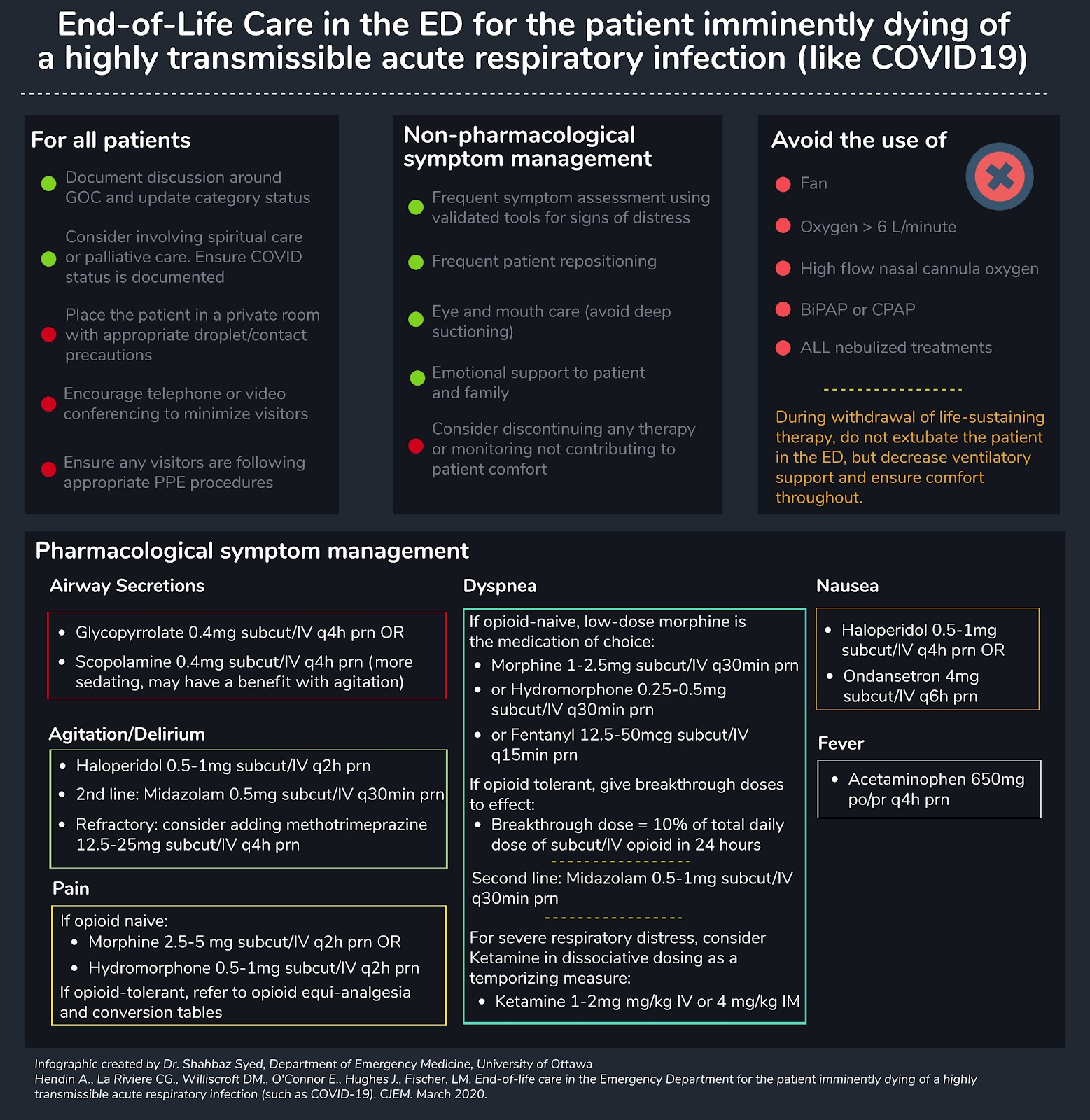
Hendin A, La Rivière CG, Williscroft DM, O’Connor E, Hughes J, Fischer LM. End-of-life care in the Emergency Department for the patient imminently dying of a highly transmissible acute respiratory infection (such as COVID-19) [published online ahead of print, 2020 Mar 26]. CJEM. 2020;1–5. doi:10.1017/cem.2020.352 PMID: 32213224
Palliative care is always an important part of emergency medicine, and unfortunately it is likely to become a much bigger part of our jobs over the coming months. This is an important paper. Although it is not the most comprehensive paper you will even read, it highlights a few of the key differences that we will have to consider when offering good palliative care to COVID patients. I have a general post about managing dyspnea in palliative care here, but there are some big changes to make. Many of our normal therapies are out: fans, open windows, high flow nasal cannulae (a mainstay of my usual palliative care approach), noninvasive ventilation, and nebulizers. Another major change is that they make a strong recommendation against extubation in the emergency department, whereas I think that is a great practice in usual times. Interactions with family will also be a big problem. Usually this is a time to have as many people at the bedside as the patient wants, but that clearly is impossible. Technology (video chat using the patient’s own own) offers an (infinitely inferior) alternative. One thing that doesn’t change is the demand that good palliative care places on nursing. In my original article, I argue for “palliative resuscitation”, meaning that these patients deserve the 1 on 1 nursing attention that goes with the degree of their critical illness. This is going to be even more difficult when every nursing assessment requires intensive PPE. One thing people may need to consider is much earlier institution of patient controlled opioids, which remain our primary pharmacologic therapy.
Bottom line: These are not going to be easy patients to manage. Just because you aren’t intubating doesn’t mean that they aren’t going to take a lot of time and resources. Start thinking about your plan now.
There is a nice infographic that summaries this paper from the great EMOttawaBlog:
Morgenstern, J. COVID Research Roundup, First10EM, April 1, 2020. Available at:
https://doi.org/10.51684/FIRS.16866




6 thoughts on “COVID Research Roundup”
Justin,
Thanks for your fantastic summaries and sage advice. Just a small note – in the UK, our FFP3 standard of mask are supposed to block out 99% of particles. The next standard down, FFP2 blocks ~95% and is supposed to be equivalent to your N95s. We don’t have many of either though.
Regards,
Steve Webb.
It’s always fascinating to me how many little differences there are between medical practices around the world. Stay safe out there.
Love your work, thanks Justin
You wrote:
.”the medical standard is an N95, which literally means it is designed to keep 95% of particles larger than 2.5 microns out”
I believe you are mistaken; the N95 is designed to filter out 95% of particles greater than 0.3 microns, not 2.5. (That’s a very important point when considering difference between filtering of so-called “respiratory droplets” and “droplet nucleii”.)