
Took a quick break from paternity leave to have a chat with my good friend Casey Parker, which of course meant we were going to talk about some evidence based medicine. I will go back to not doing academic work for a while, but for now here is that hit of nerdy goodness I know you have also been craving. (RIght?)
Bell’s Palsy and Leukemia in Children
Babl FE, Kochar A, Osborn M, Borland ML, West A, Williams A, Dalziel SR; PREDICT network. Risk of Leukemia in Children With Peripheral Facial Palsy. Ann Emerg Med. 2020 Aug 9:S0196-0644(20)30491-1. doi: 10.1016/j.annemergmed.2020.06.029. PMID: 32788067
For me this is a surprising, practice changing article. The authors are performing a triple blind multicenter trial of steroids in pediatric Bell’s palsy. However, this is not the manuscript of that trial. Instead it is a case series, because during their trial they found 5 patients with leukemia as a probable cause of their unilateral facial paralysis. They had screened 644 patients with unilateral facial paralysis, so that is a rate of 0.8%. One was a child with known leukemia, so the novel diagnosis rate was 0.6%. That isn’t a very big number, but facial paralysis is an unusual diagnosis in children, and the diagnosis of Bell’s palsy cannot be made until alternate diagnoses have been excluded. Usually that is done clinically. There are clear guidelines in adults: no testing is required unless you live in a Lyme endemic region. However, identifying 1 case of leukemia by performing 100 CBCs seems like it could be worth it, especially considering that steroids are used to treat some kinds of leukemia, and so your steroid prescription could either delay the diagnosis of leukemia or provoke a tumor lysis syndrome.
Bottom line: It is rare, but leukemia needs to be on your differential for unilateral facial paralysis in children. Whether this risk is high enough to warrant screening blood work in all children might be debatable, but my initial instinct is yes.
Avoiding troponin (and the problems with modern medicine)
Smith LM, Ashburn NP, Snavely AC, Stopyra JP, Lenoir KM, Wells BJ, Hiestand BC, Herrington DM, Miller CD, Mahler SA. Identification of very low-risk acute chest pain patients without troponin testing. Emerg Med J. 2020 Nov;37(11):690-695. doi: 10.1136/emermed-2020-209698. Epub 2020 Aug 4. PMID: 32753395
In a lot of ways, this paper epitomizes the major problems with modern medicine. During my emergency medicine training a decade ago, we spent a lot of time discussing which patients presenting with chest pain required blood work. Now, the question has been completely reversed. This paper asks: which chest pain patients don’t need blood work. That subtle shift – to the assumption that all chest pain requires a troponin – is symbolic of a larger issue throughout medicine. We have a fixed (and almost certainly false) belief that more testing is always better. Unfortunately, that shift in medical culture appears to shift the burden of proof. I don’t think anyone has ever convincingly proven that a troponin is required or beneficial for all chest pain, but now we will see demands for proof that it is appropriate to avoid blood work in some patients. This study is a secondary analysis of the HEART pathway study, which was a before and after study of adult patients with chest pain. They excluded patients with ischemic ECGs or known coronary artery disease, leaving them with a study population of 3809 patients. (They also had to exclude a significant number of patients who didn’t have a HEART score recorded, which introduces selection bias.) In these patients, they look at the performance of just the HEAR components of the HEART score. Specifically, they look at the group of patients with a HEAR score of 0 or 1, to determine whether these patients can be discharged without a troponin. Only 9% of the cohort fell into this low risk group (1.6% had a HEAR score of 0 and 7.3% had a HEAR score of 1), so the results will not let you send huge numbers of people home without bloodwork. In this group, there were 2 deaths and 2 MIs, which translates to a 30 day MACE rate of 0.9%. In itself, this could be useful, although I think the number is too high to make most physicians comfortable (even if our patients would be happy with this level of risk.) However, closer inspection reveals that these may not have been real misses. The 2 deaths were both from malignancy – so I don’t think adding a troponin was going to help. One of the MIs was in a known chronic cocaine user, and his troponin was chronically elevated, and it resulted in no changes in management. I think we would have caught this as high risk on history, and they didn’t change his management at all, so its hard to count this as a miss. The other ‘MI’ didn’t have an MI. She had a clean cardiac catheterization and a diagnosis of Takotsubo cardiomyopathy. That is a diagnosis I want to make, but even based on the limited information available – she was 56 years old and had chest pressure – it is clear to me she deserved at least a 2 on the HEART score, and wouldn’t be the kind of patient I am trying to send home without testing anyway. At the end of the day, I think that is the biggest flaw in this study. As nice as the HEART score is, it doesn’t really capture the patients I consider very low risk. When I started, if you presented with sharp chest pain that was reproducible with palpation, you didn’t get a cardiac workup. Now, those patients are getting troponins drawn at triage, and that is the trend we need to reverse. The HEAR score won’t help us with that
Bottom line: Strictly speaking, without validation, this approach is not ‘ready for prime time’. That being said, there is clearly a group of chest pain patients that don’t need troponin testing, and I think the HEAR score of 1 or less here realistically had a 0% miss rate, so there is definitely room to incorporate this data with your clinical judgement when advising patients.
Humans need food and drink. Despite rumors, physicians are humans.
Food and Drink for Staff in the Emergency Department. Ann Emerg Med. 2020 Oct;76(4):e75. doi: 10.1016/j.annemergmed.2020.06.014. PMID: 33012396
This is a really short paper, but it is probably worth including because every couple years someone will sweep through and try to completely ban food and drink for our working spaces in the emergency department. This is the ACEP policy on the issue, and they point out that we frequently do not have time for adequate breaks in the emergency department setting, and food and hydration is essential. Therefore, they think that organizations should allow food and beverages to be kept and ingested by staff in the ED. They do note food should be stored away from anywhere where specimens would be handled, should be consumed in a dedicated safe area, and appropriate hand hygiene is essential. (The need for masks during COVID obviously complicates all of this.) I have never seen a perfect solution in an emergency department, but I do think having coffee available to me is essential to my patients.
Bottom line: As a human being, you will function better if you eat and drink.
Delayed reactions to COVID vaccinations
Blumenthal KG, Freeman EE, Saff RR, et al. Delayed Large Local Reactions to mRNA-1273 Vaccine against SARS-CoV-2. N Engl J Med. 2021; [article]
As vaccination really ramps up, emergency clinicians need to be very aware of side effects. (Although, since this was written 2 months ago, I assume we have all become experts at this point.) One of the interesting things about the mRNA vaccines is the occurrence of delayed reactions, occurring more than a week after the injection. Anecdotally, I have heard of many people having a rebound of fatigue and myalgias a week after their shot. (It seemed to happen to me after my second shot, although there are many many sources of fatigue and myalgias in an aging man’s life.) This is a brief letter describing skin reactions that occur close to the infection site about a week after vaccination. Because of the timing, we might be tricked into thinking these are cellulitis rather than immunologic reactions, but a biopsy on one patient was in keeping with delayed type hypersensitivity. In other words, these need antihistamines not antibiotics (if they need any treatment at all).
COVID is airborne
Greenhalgh T, Jimenez JL, Prather KA, Tufekci Z, Fisman D, Schooley R. Ten scientific reasons in support of airborne transmission of SARS-CoV-2. The Lancet. 2021; [full text article]
Everyone reading this will already know that COVID is airborne. I am pretty certain that the people who refuse to accept this science are not among my readers. So why bother covering the topic again? (Previously covered, among many other articles, here, here, and here.) Well, I am hopeful that some of you might be in contact with the people who are still making policy decisions based on the completely misguided concept that this is a droplet spread disease, and this article is one of the most succinct summaries of the science you will find. They present 10 arguments that demonstrate fairly clearly that COVID-19 is an airborne disease:
- Superspreading events have been incredibly common, and are clearly best explained by airborne transmission
- There are multiple documented cases of long range transmission
- Asymptomatic spread – ie from people not producing significant droplets – is incredibly common
- Indoor transmission is higher than outdoor – that only makes sense with airborne spread
- Nosocomial infections are occurring even with strict adherence to droplet contact PPE
- Viable SARS-CoV-2 has been detected in the air
- SARS-CoV-2 has been found in air filters and air ducts
- Animal studies, where animals are separated in a way that only aerosols can spread between cages, show airborne spread
- There is really no evidence against airborne spread
- There is really no direct evidence that COVID is droplet spread
Bottom line: COVID is an airborne disease, and our policies and PPE decisions should reflect that fact.
Once again: Routine testing should not be performed before psychiatric admissions
Farkas A, Lipanot K, Sherman K. Routine Laboratory Screening for Acetaminophen and Salicylate Ingestion in Preadmission Psychiatric Patients Is Unnecessary. Annals of Emergency Medicine. 2021;
I have written at length about the waste and harm caused by the routine screening tests often required for psychiatric admission (despite universal agreement in guidelines that this is bad practice.) However, the practice continues, so I will continue sharing evidence as I see it. This is a chart review of 17,000 patient visits in which 33,439 acetaminophen and salicylate assays were sent for screening purposes prior to psychiatric admission. Not a single case of toxicity was diagnosed! The authors conclude the practice is unnecessary and wasteful.
Bottom line: Routine toxicology screening in psychiatric patients is unnecessary and wasteful.
Epinephrine in cardiac arrest: still no good evidence of benefit
Haywood KL, Ji C, Quinn T, Nolan JP, Deakin CD, Scomparin C, Lall R, Gates S, Long J, Regan S, Fothergill RT, Pocock H, Rees N, O’Shea L, Perkins GD. Long term outcomes of participants in the PARAMEDIC2 randomised trial of adrenaline in out-of-hospital cardiac arrest. Resuscitation. 2021 Mar;160:84-93. doi: 10.1016/j.resuscitation.2021.01.019 PMID: 33524488
It has been 3 years since the PARAMEDIC 2 trial was published, and there are still a lot of questions about the role of epinephrine in cardiac arrest. Although epinephrine results in more ROSC, more admission to hospital, and even more survival overall, it doesn’t seem to result in survival with good functional outcomes. I would interpret that as harm, but others (including our current guidelines) seem to take a life at all costs approach to the issue. To be fair, we haven’t excluded an improvement in neurologically intact survival, we just haven’t demonstrated one. Hence, the importance of the long term outcomes from the PARAMEDIC 2 trial, which is exactly what this paper looks at. They are looking at quality of life surveys from 3 and 6 months, as well as 12 month overall survival. (Unfortunately, the response rate to these surveys is poor, and not the same in both groups, which leaves the results at very high risk of bias.) At 6 months, there was still a statistical survival benefit (although quite small), with 2.9% of the epinephrine group and 2.1% of the placebo group alive (adjusted OR 1.43; 95% CI 1.05 to 1.96, and I can’t find an unadjusted OR anywhere.) However, the neurologic outcomes are complicated and overall don’t look great. Like in the original trial, the number of survivors with a good functional outcome was not statistically significant, but could favour epinephrine (2.0% vs 1.5%, aOR 1.35, p5% CI 0.93 to 1.97). However, there are numerous quality of life scales that all favour placebo based on their point estimate, and “a greater proportion of adrenaline survivors required help from another person to conduct their daily activities at 3 (adrenaline: 47% versus placebo: 31%, or 1.2% vs 0.5% respectively in all randomised patients) and 6 months (46% versus 33%, or 0.9% vs 0.4%)”. The neurologic outcomes in both groups were poor, with means scores in both groups exceeded the threshold for cognitive impairment. This remains a really complex decision without a clear answer. Unfortunately, it is not a decision in which we can involve our patients. If you know a patient’s cultural values, that should guide your decision. However, in most scenarios we will not know the patient, and will have to follow the general cultural norms. Based on previous work by this group, functional outcomes are much more important than life in the majority of North Americans surveyed. Thus, I think epinephrine should be removed from the algorithms and not used routinely.
Bottom line: The results are not easy to interpret, but overall it appears that while epinephrine increases survival by a very small amount, most of the survivors have a quality of life that most of us would not want to have. If you think all life is sacred at all costs, epinephrine is a winner. Otherwise, epinephrine should probably not be used routinely.
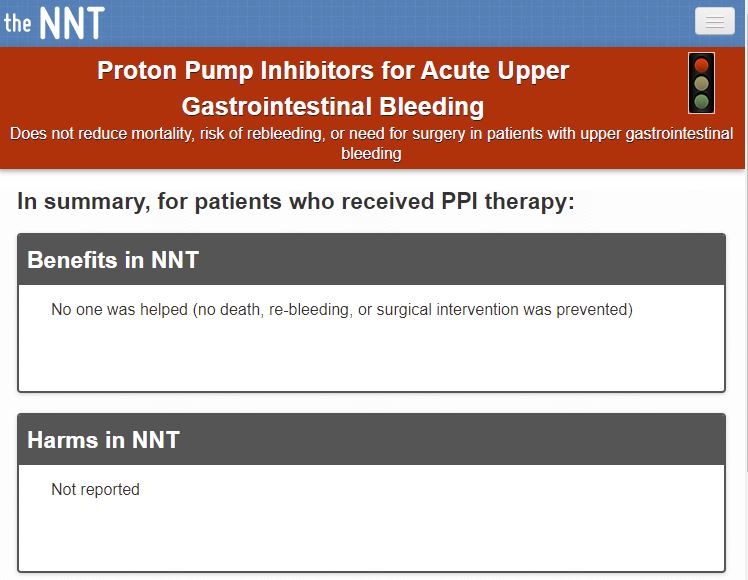
Another “we already knew that”: PPIs are useless for upper GI bleeds
Serpico M, Riscinti M. Proton Pump Inhibitors for Acute Upper Gastrointestinal Bleeding. Acad Emerg Med. 2020 Apr;27(4):336-338. doi: 10.1111/acem.13899. Epub 2019 Dec 29. PMID: 31808973
This is a “Brass Tacks” review, as part of the collaboration between AEM and theNNT, looking at proton pump inhibitors for upper GI bleeds. I have covered this topic at length in the past, so just include this paper as staged repetition. They give PPIs a “red light”, meaning no benefit. That is, across the 2,223 patients in RCTs, PPIs show no benefit in terms of mortality, need for surgical intervention, rebleeding, blood transfusion, or hospital length of stay. I will add that there was one RCT stopped early because of increased mortality in the PPI group.
Bottom line: There is no role for PPIs in the emergency management of upper GI bleeds. I have not prescribed them in at least 8 years.
The theme of the month is things we already knew. This time: CT contrast does not cause kidney injury.
Goulden R, Rowe BH, Abrahamowicz M, Strumpf E, Tamblyn R. Association of Intravenous Radiocontrast With Kidney Function: A Regression Discontinuity Analysis. JAMA Intern Med. 2021 Apr 5. doi: 10.1001/jamainternmed.2021.0916 PMID: 33818606
Any long time readers will be well aware that I believe contrast induced nephropathy is a myth. Although another observational study is unlikely to add a lot to our knowledge, I thought this study used an ingenious approach that makes it valuable to talk about. They look at 156,028 emergency department patients who had a D-dimer test drawn, and make the assumption that those just above the threshold will be very similar in all respects to those just below the threshold, with the exception of their exposure to contrast. I think that is a good assumption, and probably makes this the best control group to date. I don’t know that I fully comprehend the stats here, but a “fuzzy regression discontinuity” is an amazing name for an analysis. There was no difference in their primary outcome of change in long term eGFR (although data was only available for half the patients). There was no difference in the need for renal replacement therapy, acute kidney injury, or all cause mortality. I think the data was already pretty convincing, but this is one of the strongest studies to date.
Bottom line: Contrast almost certainty doesn’t cause important levels of kidney injury.
Bushfires and kangaroo injuries
Hardy P, Harris D, Clarke C, Ellis DY. Increased incidence of kangaroo-related trauma following a severe bushfire season. Emerg Med Australas. 2021 Mar 4. doi: 10.1111/1742-6723.13761. PMID: 33665990
We finally get to the important stuff. I know people tune in for highly practical information, and may have been disappointed so far, but this paper should satisfy your needs. This chart review found that the severe brushfire season in Australia was associated with a significant increase in kangaroo-related trauma. One might guess that this was just accidental: that with less room to work with, kangaroos are more likely to be found in the same space as humans, and therefore jumping out in front of cars. (I sort of assume the same would be true of deer or moose in Canada, but someone is going to have to do the study to find out). However, upon more reflection, I think this might be purposeful action on the part of the kangaroos. They are trying to punish the idiot humans for destroying the environment.
Need an excuse for sex? It will help you breathe
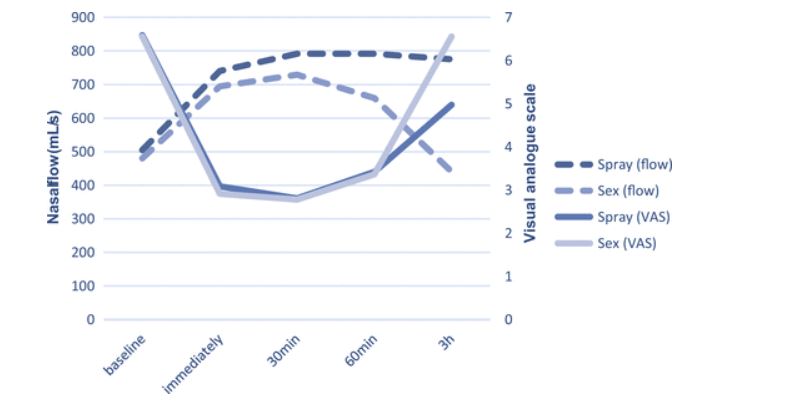
Bulut OC, Oladokun D, Lippert BM, Hohenberger R. Can Sex Improve Nasal Function? An Exploration of the Link Between Sex and Nasal Function. Ear Nose Throat J. 2021 Jan 4:145561320981441. doi: 10.1177/0145561320981441 PMID: 33393816
As a lifelong sufferer from allergic rhinitis, this paper immediately caught my eye. They jump right in by telling us that “a physiological connection between the nose and the genitals has long been proposed”. (Admittedly, this theory seems to have its origins in Freud, who literally thought there was a direct connection between the genitals and everything, so the nose may not be all that special.) There is a somewhat plausible connection, in that the nasal mucosa is controlled by the parasympathetic and sympathetic nervous systems, and the old “point and shoot” mnemonic reminds us that those systems are involved in normal sexual function. However, these authors note that there are no studies investigating the impact of sexual activity on nasal breathing, and so set out to test whether “love is all you need… to improve nasal breathing.” 18 heterosexual couples measured nasal function before sexual activity (baseline), immediately after orgasm, and then 30 minutes, 1 hour, and 3 hours after sexual climax. (They were all healthcare workers, so these results may not extrapolate to the sex lives of ‘normal’ people.) The data was only obtained if both people experienced an orgasm, which brings to mind many inappropriate jokes that I will leave out considering that this is a classy literature review. They also compared these results to the effects of a nasal decongestant (xylometazoline 0.1%). Both the decongestant and sexual orgasm improved nasal breathing for approximately 1 hour after use. However, the spray was still moderately effective at 3 hours, whereas sex was not. (I am not sure whether you would develop tachyphylaxis to sex like you do to these nasal sprays, as they did not look at long term outcomes in this study.)
Bottom line: Sex is good. Depending on your life circumstances, sex might be cheaper than a nasal decongestant. (Then again, it might not be.)
Cheesy Joke of the Month
Someone has been going around stealing the wheels off police cars.
The police have been working tirelessly to catch him.
Morgenstern, J. Research Roundup (May 2021), First10EM, May 3, 2021. Available at:
https://doi.org/10.51684/FIRS.78329


One thought on “Research Roundup (May 2021)”
I am reading this 3 months late, but it was worth it. Thanks for the excellent laugh!