
Morgenstern, J. COVID therapy evidence updates: fluvoxamine, First10EM, February 4, 2022. Available at:
https://doi.org/10.51684/FIRS.125040
This is part of the ongoing series of articles updating the evidence on current COVID-19 therapies. The rest of the series can be found here, and there is more to come. This article will cover the evidence for fluvoxamine in COVID-19.
A philosophical interlude
If this is the first post in this series that you are reading, it might be worth reading the philosophical interlude from part 1 of the series which explains why my conclusions sometimes differ from those of the Ontario Science Table.
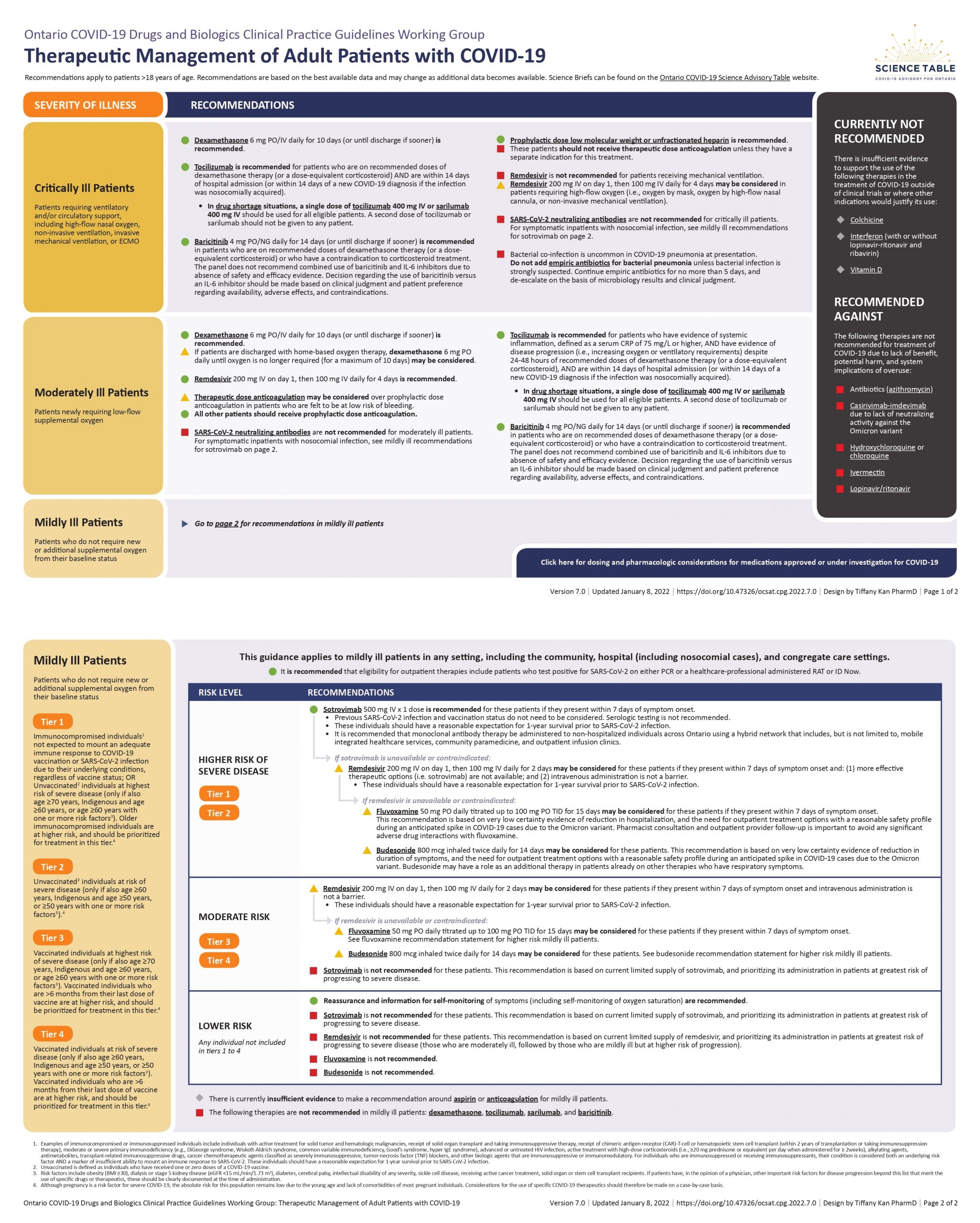
The Ontario Science Table recommendation
Not recommended for severely ill or moderately ill patients.
For mildly ill patients, fluvoxamine may be considered in patients at high risk of severe disease if paxlovid is unavailable or contraindicated.
In mildly ill outpatients with moderate risk of severe disease, fluvoxamine may be considered for those presenting within 7 days.
For mildly ill patients with low risk of progression to severe disease, fluvoxamine is not recomended.
(Full recommendations available here.)
The evidence for fluvoxamine
The STOP COVID trial was a placebo-controlled, double-blind RCT comparing 15 days of fluvoxamine to placebo in outpatients within 7 days of symptoms onset with confirmed COVID-19 infection. (Lenze 2020) It is an interesting study design, as the patients were never seen in person. They were enrolled electronically, and all data was collected through REDCap surveys. They enrolled 152 patients in the study, and a big weakness is that only 115 (76%) completed the trial. Their primary outcome was clinical deterioration, and was significantly decreased in the fluvoxamine group (0% vs 8.3%, p=0.009)
The TOGETHER trial was a randomized, adaptive platform trial that randomized unvaccinated adult patients within 7 days of symptom onset and at least 1 high risk feature to either a 10 day course of fluvoxamine or placebo. (Reis 2021) Although technically positive, there are some major issues with this trial. Their primary outcome was incredibly biased and not patient oriented. It was the composite of hospitalization or 6 hour emergency department observation due to COVID. In these COVID evidence summaries, I have already decried the use of disease specific hospitalization many times. It is inherently biased, in that it automatically ignores any hospitalizations from drug side effects, and is completely irrelevant to patients (who would care about all cause hospitalization). This trial is even worse, as they equate a 6 hour ED visit with hospitalization, when in fact those outcomes are completely opposite. If you are observed for 6 hours and well enough to go home, that is actually a good outcome and the exact opposite of hospitalization. So although this primary outcome is reported as positive (16% vs 11%, RR 0.69), it is completely irrelevant. There was no change in mortality (2% vs 3%, p=0.24). There was no difference in viral clearance at day 7, mechanical ventilation, number of days ventilated, or number of days hospitalized. There wasn’t even a difference in COVID-19 related hospitalization. The only outcome that changed was ED observation (1% vs 5%, p=0.0001). Bottom line: Despite the headline, I think this is clearly a negative trial. No important outcomes were changed, and the obvious bias should overrule any differences that were seen.
Comments
The proposed physiologic mechanism for fluvoxamine to work against COVID-19 is an anti-inflammatory effect mediated through the sigma-1 receptor. Considering the complexity of the immune system, it is not surprising that almost any chemical will have some effect on inflammation, but the data that fluvoxamine did anything of value in infections prior to COVID was scant at best. (Lenze 2020; Hashimoto 2022) More importantly, this mechanism suggests that if fluvoxamine is going to be beneficial, it will be beneficial in the later stages of disease, in the same populations in whom we use steroids or tocilizumab. However, it is being tested in healthy outpatients soon after symptom onset, which makes absolutely no sense to me considering the proposed mechanism of action. Furthermore, if the mechanism of action truly is anti-inflammatory, is there any reason I would want to use an SSRI to indirectly target just one aspect of the immune system, rather than using an actual anti-inflammatory, like a systemic steroid?
The STOP COVID trial data is reasonable, but as the authors state, preliminary and incomplete. (And it sounds like STOP COVID 2 was stopped early for futility.) The STOP COVID results do increase my estimation that fluvoxamine could help, but our a priori belief that fluvoxamine would improve outcomes in COVID should have been very very low. Thus, if I started with a less than 5% belief that fluvoxamine would help patients (to be generous), the STOP COVID trial might increase that to as high as 10%. On the other hand, the TOGETHER trial looks very negative to me, and may even decrease my confidence in fluvoxamine. Thus, I am left with (very generously) a 10% chance fluvoxamine might provide some value in unvaccinated COVID patients, but still a 90% chance that there is no value and only harm.
The TOGETHER trial only included unvaccinated patients. If for some reason, the small decrease in emergency department observations convinced you to prescribe it, you should be aware that the difference will probably almost completely disappear in a vaccinated population.
As I discussed with molnupiravir, I think we need to be very cautious about publication bias during COVID. Although most COVID trials have been registered, there has been a clear pattern of positive trials being published immediately (or through press releases) while negative trials of the same drug remain unpublished. There are a number of ongoing trials of fluvoxamine. I believe the STOP COVID 2 trial is completed but not yet published. (It seems like it was stopped early for futility.) I don’t know of any other completed trials, but I think it is prudent to expect that there may be a significant delay in the publication of negative or ‘less exciting’ results for all COVID therapies. Obviously, there is no way to know for sure whether publication bias is influencing the published results for fluvoxamine or any other potential COVID therapy, but I think we should anticipate it will occur with some regularity and temper our conclusions accordingly.
Bottom line
At this point, I don’t think there is any convincing evidence of benefit from fluvoxamine, so all we are left with is potential harm. I don’t think anyone should be prescribing it for COVID-19 outside of proper RCTs.
Other FOAMed
Other First10EM COVID therapeutics updates can be found here
Ontario Science Table Recommendations
COVID-19 Update: An Interesting Study on Serotonin Antagonism
The TOGETHER Trial: COVID-19 and Fluvoxamine Take Two
References
Hashimoto Y, Suzuki T, Hashimoto K. Mechanisms of action of fluvoxamine for COVID-19: a historical review. Mol Psychiatry. 2022 Jan 7:1–10. doi: 10.1038/s41380-021-01432-3. Epub ahead of print. PMID: 34997196
Lenze EJ, Mattar C, Zorumski CF, Stevens A, Schweiger J, Nicol GE, Miller JP, Yang L, Yingling M, Avidan MS, Reiersen AM. Fluvoxamine vs Placebo and Clinical Deterioration in Outpatients With Symptomatic COVID-19: A Randomized Clinical Trial. JAMA. 2020 Dec 8;324(22):2292-2300. doi: 10.1001/jama.2020.22760. PMID: 33180097
Reis G, Dos Santos Moreira-Silva EA, Silva DCM, et al. Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial. Lancet Glob Health. 2021 Oct 27:S2214-109X(21)00448-4. doi: 10.1016/S2214-109X(21)00448-4 PMID: 34717820 NCT04727424
Photo by Annie Spratt on Unsplash




{kind=link}
One thought on “COVID therapy evidence updates: fluvoxamine”