
Morgenstern, J. Gender inequity in emergency medicine, First10EM, December 20, 2021. Available at:
https://doi.org/10.51684/FIRS.123874
It is impossible to deny the significant gender inequities that currently exist in medicine. Women are under-represented in leadership positions.1–3 Women are less likely to be given senior academic promotions.4 There are fewer women in editor positions in our academic journals.5 Women receive less grant funding.6,7 Women are paid less than men, even after accounting for potential confounders.2,8–10
The literature describes many factors that contribute to this inequity. Institutional policies related to promotion or advancement may inherently disadvantage women, and are may be exacerbated by implicit bias and stereotyping.11–13 There are an insufficient number of women in current leadership positions, resulting in fewer mentors and role models for women early in their career.11 Women receive fewer opportunities to get started in academia, such as presenting at grand rounds.14 Policies around parental leave, emergency child-care, and breast-feeding affect women disproportionately.13 Unfortunately, sexual harassment is also still widely documented in emergency medicine, and has a major impact on career advancement and attrition.15–17
The gender pay gap is somewhat better studied, but the reasons for the gap are complex, and likely not completely understood. Existing gender balance within specialties, among other aspects of the ‘hidden curriculum’, likely influence career decisions, with women trainees more likely to enter lower paying specialties. (This is one of many reasons that I believe doctors deserve equal pay whatever your specialty, but that is a topic for another day.) Current leadership positions are dominated by males, who may then (consciously or not) be more supportive of other males for future promotions. Furthermore, there are numerous gender differences, both internal and external, that influence salary expectations and negotiations.18
Female physicians are more likely to have female patients, and medical pay structures are often inherently biased. For example, in Ontario (where I am now somewhat embarrassed to work) a biopsy of the penis pays almost 50% more than a biopsy of the vulva. Similarly, incision and drainage of a scrotal abscess pays twice as much as I&D of a vulvar abscess.18
There is data that suggests that practice patterns vary between women and men. Women in primary care are more likely to address multiple issues during a single appointment. They are more likely to provide emotional support and address psychosocial issues, and less likely to perform procedures. Although these are features most of us would want in our own physician, they unfortunately result in lower remuneration in more medical payment models.18
And of course, all of this occurs in the larger societal context in which women perform far more unpaid labour outside of medicine, resulting in a much larger overall workload, most of which is overlooked. (For a wonderful book on the topic, consider reading Invisible Women by Caroline Criado Perez).
Too often, women are blamed for the gender pay gap. It is true that women, on average, work fewer hours, and are more likely to work part time. However, this difference in work is not enough to explain the pay gap. For example, one study found that women earned 36% less than their male colleagues, despite only working 3 hours less per week.18 Disparities in pay begin immediately upon entry into the job market, so they can’t be explained by productivity or merit, and persist in analyses that adjust for a broad range of confounders, such as choice of specialty, part-time work, and level of training.2,19
It is also not true that women earn less because they are less efficient. Data from Ontario revealed that female surgeons earn 24% less per hour spent operating, despite completing procedures in the same amount of time as men. The difference seems to derive from women performing less lucrative procedures.20
In this month’s Skeptics’ Guide to Emergency Medicine Hot Off The Press episode, we discuss a paper by Lee and colleagues that discussed a local program developed to help address gender inequities.21
The Paper
Lee LK, Platz E, Klig J, Samuels-Kalow ME, Temin ES, Nagurney J, Marsh R, Rouhani S, Huancahuari N, Dubosh NM, Boyle KL, Stack A, Dobiesz VA. Addressing gender inequities: Creation of a multi-institutional consortium of women physicians in academic emergency medicine. Acad Emerg Med. 2021 Jul 31. doi: 10.1111/acem.14361 PMID: 34331734
Methods
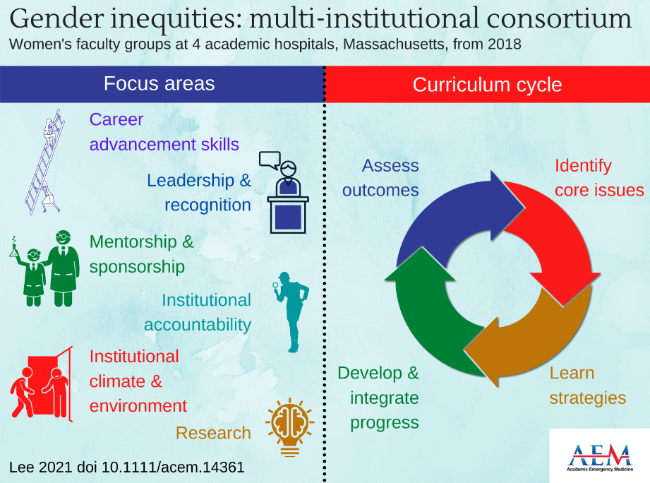
This article describes the creation of a multi-institutional consortium of female faculty in emergency medicine to promote career advancement and address issues of gender inequity. The consortium brought together female faculty from 4 hospitals associated with Harvard Medical School. Led by site champions at each site, they developed events based on informal needs assessments and literature reviews, and developed systems for information sharing for important policy information among the hospitals.Goals and priorities were developed using an interactive cycle: identify, learn, develop, and assess.
Key Results
These authors present their experience in the development of this female faculty consortium. A total of 80 female faculty (representing 37% of the total EM faculty) were represented by the consortium in the 2020 academic year. They ran multiple local career development events and organized a larger conference. The COVID pandemic derailed in person events, but they continued to host quarterly virtual events.
They identify a number of challenges. It is difficult to meet the individual needs of all participants across all career stages. Scheduling is difficult in emergency medicine, with clinical responsibilities continuing 24 hours a day. Operating without a formal budget makes sustainability challenging.
Based on their experience in establishing this consortium, the authors provide advice for others interested in developing a similar program in 4 key domains: leadership, finances, communications, and curriculum development. They believe a formal leadership structure will improve sustainability and accountability. Furthermore, a formal budget with ongoing funding is important for group sustainability. Although smartphone texting groups allow for very easy group communication, they suggest designating a specific communications director. Finally, they recommend adopting a formal process for curriculum development based on a formal needs assessment of the faculty members, combined with the published literature, and setting a calendar of events to enhance attendance and relevance for group members.
For a full discussion, check out the podcast. One of the big advantages of the SGEM Hot off the Press series is that the audience gets to interact with the authors of the paper, so please join the discussion either on the SGEM blog, or on twitter using the hashtag #SGEMHOP.
Discussion
I think programs like the one described are important, and we need to see more of them in medicine. Obviously, this publication is descriptive, and should leave the scientific minded with many questions.
This program appeared to be quite successful in the short term in generating engagement and developing career skills for female faculty, but it is unclear if these early successes will generate the desired gender equity in emergency medicine in the long run. It is unclear if this approach is the best approach. It is somewhat unlikely that a single approach works for everyone. It is unclear whether the program described will work in other settings. (We know that women are significantly under-represented in academic emergency medicine. This consortium brought together a group of women who hold academic positions at one of the most prestigious medical schools in the world. They are, by definition, outstanding.)
Despite these many remaining questions, there is no doubt that we face a massive inequity problem in medicine, and that will need to act now, even in the absence of perfect science to guide us.
Steps forward
We clearly have a problem in medicine. There is no denying the current state of gender inequity. Solutions, while in some cases glaringly obvious, are probably rather complex. Solutions are unlikely to be ‘one size fits all’. The needs and desires of individual women will obviously be far more varied and far more complex than the ‘average woman’. We should always be wary of unintended consequences when implementing social policy. We need to be careful to consider the true causes of inequity, as the solutions will be highly dependent on the cause. However, those are not excuses. The data speaks for itself. Action is needed, and it is needed now.
The first step is to widely and openly acknowledge the current problem.19 This would be aided with transparent reporting on physicians payment, stratified by gender. (It is worth noting that gender is not the only source of inequality in medicine, and this same data should be used to examine other factors such as race or disability.)
We need to consider more egalitarian interview processes, where leadership are blinded to characteristics like gender or race.22 We need better training about bias in medicine, especially for those in leadership positions.13,19 We need career development and mentorship programs dedicated specifically to women (and other groups facing discrimination).19,22 We need to consider the impacts of systemic discrimination, and recognize that simply being fair in a single hiring decision is unlikely to be good enough, as it doesn’t account for the incredibly different paths that candidates to reach the same point.13 We need to ensure that women are well represented on promotions committees.13,22 We need to fix clearly sexist billing codes and referral patterns. We need better parental benefits, and systems to ensure career advancement can continue even one one is taking time to raise children.19,22
This is just a subset of what needs to be accomplished. There are numerous excellent publications that go into more details.2,13,22
EDIT December 21, 2021: I have had a number of conversations about this post, and I think a few clarifications will help.
First, this is a brief review of the literature and not one of the deep dives many have becomes accustomed to on this blog. As such, I have spent less time discussing the short-comings of the methodology in the papers. These are all observational studies, and therefore the short-comings are substantial. Perhaps the biggest is that the studies don’t separate out the inequities faced by women from the inequities faced by mothers. Choices around parenthood will affect both genders, but disproportionately affect females. This is an important distinction, because it impacts solutions, and highlights issues that might be faced by primary caregivers who are not mothers.
It is also important to distinguish between inequity and difference. The studies can describe differences in medicine between genders, but differences do not automatically equate to inequities. For example, imagine we found that 75% of peer reviewers for a major journal were male. There is clearly a difference based on gender, but without more information it is impossible to know whether there is an inequity. Personally, I think peer review is silly. It is difficult, unrecognized, volunteer work, often done for for-profit companies. I always say no to requests for peer review. Perhaps women are just making smarter decisions with their time, and refusing to get involved in this kind of work. If the opportunity for such work is equal for both genders, and women simply choose not to partake, the published difference is not inequity.
It is essential to distinguish between equality of opportunity and equality of outcomes. I don’t think anyone believes that a physician working 20 hours a week should be paid identically to a physician working 80 hours a week (but overly simple comparisons of outcome can sometimes imply this). But equal work should clearly receive equal pay.
Not all of the differences I described at the outset will represent inequity. And not all inequity represents bias. I believe bias exists in medicine, but I don’t believe it explains all of the differences seen between men and women. These studies represent a complex mix of bias, different life choices, different personalities, and cultural expectations. These distinctions are important, because without them it is impossible to know what problem we are trying to solve, and what the appropriate solutions are likely to be.
Other FOAMed
SGEM#352: AMENDMENT – ADDRESSING GENDER INEQUITIES IN ACADEMIC EMERGENCY MEDICINE
References
1. Gold JA, Roubinov D, Jia LS, et al. Gender Differences in Endowed Chairs in Medicine at Top Schools. JAMA Intern Med 2020;180(10):1391–4.
2. Madsen TE, Linden JA, Rounds K, et al. Current Status of Gender and Racial/Ethnic Disparities Among Academic Emergency Medicine Physicians. Acad Emerg Med 2017;24(10):1182–92.
3. Cheng D, Promes S, Clem K, Shah A, Pietrobon R. Chairperson and faculty gender in academic emergency medicine departments. Acad Emerg Med 2006;13(8):904–6.
4. Jena AB, Khullar D, Ho O, Olenski AR, Blumenthal DM. Sex Differences in Academic Rank in US Medical Schools in 2014. JAMA 2015;314(11):1149–58.
5. Ravioli S, Rupp A, Exadaktylos AK, Lindner G. Gender distribution in emergency medicine journals: editorial board memberships in top-ranked academic journals. Eur J Emerg Med 2021;28(5):380–5.
6. Sege R, Nykiel-Bub L, Selk S. Sex Differences in Institutional Support for Junior Biomedical Researchers. JAMA 2015;314(11):1175–7.
7. Dubosh NM, Bellolio MF, Rabinstein AA, Edlow JA. Sensitivity of Early Brain Computed Tomography to Exclude Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis. Stroke 2016;47(3):750–5.
8. Wiler JL, Rounds K, McGowan B, Baird J. Continuation of Gender Disparities in Pay Among Academic Emergency Medicine Physicians. Acad Emerg Med 2019;26(3):286–92.
9. Read S, Butkus R, Weissman A, Moyer DV. Compensation Disparities by Gender in Internal Medicine. Ann Intern Med 2018;169(9):658.
10. Frintner MP, Sisk B, Byrne BJ, Freed GL, Starmer AJ, Olson LM. Gender Differences in Earnings of Early- and Midcareer Pediatricians. Pediatrics 2019;144(4):e20183955.
11. Yedidia MJ, Bickel J. Why aren’t there more women leaders in academic medicine? the views of clinical department chairs. Acad Med 2001;76(5):453–65.
12. Cooke M. Implicit Bias in Academic Medicine: #WhatADoctorLooksLike. JAMA Intern Med 2017;177(5):657–8.
13. Madsen TE, Heron SL, Rounds K, et al. Making Promotion Count: The Gender Perspective. Acad Emerg Med 2019;26(3):335–8.
14. Boiko JR, Anderson AJM, Gordon RA. Representation of Women Among Academic Grand Rounds Speakers. JAMA Intern Med 2017;177(5):722–4.
15. Lu DW, Dresden S, McCloskey C, Branzetti J, Gisondi MA. Impact of Burnout on Self-Reported Patient Care Among Emergency Physicians. West J Emerg Med 2015;16(7):996–1001.
16. Choo EK, Byington CL, Johnson N-L, Jagsi R. From #MeToo to #TimesUp in health care: can a culture of accountability end inequity and harassment? Lancet 2019;393(10171):499–502.
17. Fnais N, Soobiah C, Chen MH, et al. Harassment and discrimination in medical training: a systematic review and meta-analysis. Acad Med 2014;89(5):817–27.
18. Cohen M, Kiran T. Closing the gender pay gap in Canadian medicine. CMAJ 2020;192(35):E1011–7.
19. Choo EK, Kass D, Westergaard M, et al. The Development of Best Practice Recommendations to Support the Hiring, Recruitment, and Advancement of Women Physicians in Emergency Medicine. Acad Emerg Med 2016;23(11):1203–9.
20. Dossa F, Simpson AN, Sutradhar R, et al. Sex-Based Disparities in the Hourly Earnings of Surgeons in the Fee-for-Service System in Ontario, Canada. JAMA Surg 2019;154(12):1134.
21. Lee LK, Platz E, Klig J, et al. Addressing gender inequities: Creation of a multi-institutional consortium of women physicians in academic emergency medicine. Acad Emerg Med 2021;
22. Agrawal P, Madsen TE, Lall M, Zeidan A. Gender Disparities in Academic Emergency Medicine: Strategies for the Recruitment, Retention, and Promotion of Women. AEM Educ Train 2020;4(Suppl 1):S67–74.



5 thoughts on “Gender inequity in emergency medicine”
“Female physicians are more likely to have female patients, and medical pay structures are often inherently biased. For example, in Ontario (where I am now somewhat embarrassed to work) a biopsy of the penis pays almost 50% more than a biopsy of the vulva. Similarly, incision and drainage of a scrotal abscess pays twice as much as I&D of a vulvar abscess”
You are embarrassed to work in Ontario because of this?
The payment reflects the complexities of procedures, with a penile biopsy there is a risk of damage to the urethral meatus, and abscess drainage is in direct contact with the peritoneum, vulva is not. Take another example, tubal ligation pays more than vasectomy, is that related to “sexist” billing codes?
“There is data that suggests that practice patterns vary between women and men. Women in primary care are more likely to address multiple issues during a single appointment. They are more likely to provide emotional support and address psychosocial issues, and less likely to perform procedures. Although these are features most of us would want in our own physician, they unfortunately result in lower remuneration in more medical payment models”
Though I would agree that cognitive work should be rewarded, and in Ontario billing codes exist to reward the duration and complexity of consults. I fail to see why this should be examined through a gender lens. Let us perform a thought experiment, take the above example and say the reverse was true. In fact, women were less likely to perform cognitive and complex work and more likely to perform procedures, which benefited women financially more than men. Would that justify that cognitive or complex work continue to be rewarded less in the billing schedule? The question of fairness should be defined regardless of which gender benefits.
The issue of rewarding procedures over cognitive work has nothing to do with gender. For example, obstetricians are a female (62%) dominated surgical speciality and make on average $417,996, while neurology, a cognitive speciality dominated by males (64%) earns $333,065, even though neurologists work on average 6 hours more per week. A similar comparison can be shown with psychiatry.
“Too often, women are blamed for the gender pay gap. It is true that women, on average, work fewer hours, and are more likely to work part time. However, this difference in work is not enough to explain the pay gap. For example, one study found that women earned 36% less than their male colleagues, despite only working 3 hours less per week”
This is not a question of blaming women but highlighting the fundamental limitation with such research. When two populations are vastly different in working characteristics, even after adjustments for known confounders, the probability is high that many other confounders are not adjusted for, and therefore differences in pay may persist. The gender pay gap is then used to argue for underlying gender discrimination, when in fact confounders in working characteristics are more likely to explain the difference.
The article that you cite does not even remotely refute this. From the paper, “we found that female physicians earn less annually and have smaller practices and fewer annual patient contacts, compared to their male counterparts”. The authors did not measure hours worked between the sexes, they referenced a National Physician Survey, which reported the “3 hours less per week”, and concluded therefore the pay gap may not be explained by hours worked.
Ganguli (N Engl J Med 2020) demonstrated the gender gap may be completely explained in primary care in the United Stated after adjusting for working characteristics. They did find that women spent more time with patients and therefore earned less, however as mentioned above, I don’t see the justification in analyzing this through a gender lens.
Fee-for-service compensation does not contain any gender modifiers. There is a simple input (number and type of codes) and output (payment) relationship, and every single penny should be accounted for by the frequency and type of codes that are largely determined by working characteristics. The possible exception is surgery, as the study you referenced may be limited by access to procedures, however that does not exist in non-surgical specialties.
“We clearly have a problem in medicine. There is no denying the current state of gender inequity.”
Everyone believes in gender equality, the issue is not the goal, but the unconvincing arguments that are used to suggest how pervasive the problem is.
The one who makes the claim has the burden of proof, and I am unconvinced by your arguments and remain skeptical.
Huge fan of your Justin but I think this is off base.
As a female physician, I choose to work less nights/high acuity shifts. That’s my choice. Do I make less that my male counterparts because of that? Sure. But that’s ok.
If there’s any group out there that truly pays men more than women for the same work, then of course that’s blatantly wrong. I haven’t encountered that group, and it seems unlikely to me that it’s out there.
In regards to women in leadership positions, I agree there needs to be more balance. Have you considered; however, that maybe women apply less for these positions? That’s certainly less desirable to me as I consider my work-life balance.
The vast majority of people want gender equality. It seems extremely unlikely to me that men and women in EM make different monetary amounts for the same work. I followed the thread on EM Docs and there was a couple things pointed out that may results in a slight slow down on shift for women (being mistaken for nurses, etc), but this almost certainly does not account for the pay differences you site.
Thanks for the comment
This is certainly difficult as payment structures vary so dramatically around the world
I used to think this was primarily based on differing choices, whether for shifts or time off for parenting, But more and more studies seem to adjust for all those factors and still find a big difference
It’s certainly not all one or the other. I think individual choices like you describe certainly play a part. I imagine the biggest component is differing choices and societal expectations around being a parent. However I think the evidence is fairly solid that there is more to it than just different choices. When I say there’s a difference that isn’t to imply that it is 100% the result of bias, but I think there is still a component of bias based on the data we have.
Unlike many topics discussed on this blog, the data here is incredibly poor because it can only be retrospective observational data. So my level of certainty is low, and I think we all need to admit that. However, I think the data does still suggest inequity, so the question is which error is worse: denying inequity that is there or accepting the claim of inequity when it is not. In my mind, it really depends on what solutions you are proposing. I don’t pretend to have any answers, but I think we would be better off if this was an ongoing, open conversation in every department.
I see what you’re saying. You’d rather address a potential bias that may exist than ignore it.
To my read the blog was presented as pretty concrete, but in the response above you admitted the “data is incredibly poor”, and “level of certainty is low”. I guess I’m just wary of creating inflammation when (in my opinion) common sense would say there’s likely not a huge disparity here (i.e. there aren’t RVU multipliers for men, and hopefully no physician groups are paying docs differently simply because of gender). There’s so many bigger things to be fighting for in EM right now that have strong evidence behind them.
There are definitely societal expectations around being a parent. It’s certainly different than it was 50+ years ago, with men now typically being much more involved and sharing the burden of parenting (at least in my experience with my husband and observing friend’s husbands). I will say that I cherish the special bond I have with our babies due to the experience of carrying a baby for 9 months, birthing them, and breastfeeding them, an experience that a man will never have. I think that’s worth being celebrated.
I’m happy to live in an era and country where education for women is encouraged and celebrated. I’m happy to have a job that allows me to pursue as much financial gain as desired or spend more time at home. Gender inequality is overt in many parts of the globe and still exists in places in the western world, which is devastating.
I celebrate your desire for gender equality, trust me I want the same thing. I just think how we address a subject is important, and have some questions about what was presented/how it was presented. I would echo some of “Toms” sentiments in the comment above.
Keep on rockin Justin, you’ve been a favorite blogger for a long time!
Your critique is definitely valid.
Finding the right language to express this is difficult, and this was written primarily as an introduction for a journal article, rather than my standard (more verbiose) blog format.
The data itself is quite weak. However, I think the data is additive enough to be certain that there still exists some fundamental difference that is based on gender, rather than just life choices. (How life choices should impact careers is a much more difficult question that I am completely unable to answer.) We are certain that there is a gap – not just in pay, but also in academic promotions and other leadership positions. The fundamental underlying question is the cause of that gap. If the gap is entirely based on choices made by individual women, there may not be any inequity at all. (We would still have to consider why choices are being made, as choices are rarely as free as they seem, and inequity could still exist in choices that seem fair at first glance.) My take, reading this literature, is that the gaps we are seeing are a complex mix of multiple factors, and that it would be a mistake to think that the gaps we are seeing are entirely based on individual choices.
My guess is that the biggest factor is the choice to become a parent, which has much bigger impacts on women than men, but it would be interesting to compare the impacts to those experienced in same sex couples. In itself, this doesn’t necessarily create inequity (even if it does result in difference in pay or promotions), but I think it varies greatly depending on local circumstances. Some groups have great parental leave options, flexible shifts allowing for childcare, accommodations for breastfeeding, etc. Other groups have none of this. I don’t know the exact policy that is ‘fair’, but I think it is clear that some policies can still create inequity, even if it is triggered by a personal choice.
However, I think there are many other factors at play here, and at least some of likely represent true inequity. (For example, in my city, there were two emergency departments that were incredibly well known for never hiring women. It has changed recently, but there were exactly 0 females on staff in very large departments. Those are incredibly egregious examples of discrimination, which can be traced to a single problematic chief, but if such egregious examples can exist in modern medicine, I find it hard to believe that subtler forms of implicit bias aren’t also at play in some decisions.)
In terms of where we should spend our time and effort, that is a very good question. Some of the gender equity stuff should take almost no effort or time, such as transparency in salaries and promotion criteria. Other efforts may lead to diminishing returns. I certainly don’t have the answers, and wouldn’t prescribe any kind of agenda. It is an issue I care about, but seeing as I have written more than 350 blog posts over the years, and the issue has only come up once, I also don’t think I am over-prioritizing it. (In fact, I am sure there are members of the emergency medicine community who would argue that I have under-prioritized it.)
I really appreciate the conversation. This is not a topic with a simple answer, and there are clearly a wide range of opinions. I think there is a lot of value in the conversation, and I do think that your criticism of my language is very fair. (I will continue to use lack of sleep due to caring for an infant as an excuse for as long as I can milk it.)
All the best
Justin