
Morgenstern, J. COVID therapy evidence updates: budesonide, First10EM, January 17, 2022. Available at:
https://doi.org/10.51684/FIRS.124758
I have avoided COVID therapies for a while, because so many people are already covering the topic, and honestly I am a little sick of COVID. However, with the OMICRON wave, everyone seems to have questions about therapies for COVID, so a quick evidence review seems appropriate. This article will cover the evidence for budesonide in COVID-19, and there will be a number of follow-up articles on other topics posted soon(ish).
A philosophical interlude
Throughout the pandemic, my friend Andrew Morris has been leading the working group for the Ontario Science Table providing recommendations on the therapeutic management of adult patients with COVID-19. The most recent version of their guidelines can be found here. Although I usually agree with Andrew on just about everything, I have found myself disagreeing with these guidelines on a number of occasions. I think these disagreements boil down to a difference in philosophy about the need for science and certainty during a pandemic, so I would like to start with some general philosophical thoughts before getting to the evidence.
Personally, I think we should be using the same standards for science now as we always do. I think others, including Andrew, believe that the potential benefits during a pandemic mean that we should accept more uncertainty, as there is an urgent need for action.
I believe Andrew would argue that, as our hospital systems crumble, any therapy that could possibly reduce hospitalizations or ICU use should be considered, even if the current evidence is imperfect. Although reasonable on its face, I think there are a number of problems with that argument.
All treatments cause harm. Any unproven treatment could actually end up increasing demands on hospital resources through adverse events, especially as use expands beyond the tightly controlled trial setting. For a variety of reasons, medical studies generally overestimate benefits and underestimate harms. This is why we demand (or at least we should) solid evidence of benefit before implementing new therapies. The same applies (or should) to COVID-19.
Empirically, throughout the history of medicine, most new potential therapies fail. It is hard to have a positive impact on the complex homeostasis that is human biology. We also know that a huge number of apparently positive trials are never replicated. If we have a problem in medicine, it is with overestimating the benefit of our purported therapies. The argument that novel therapies could reduce healthcare demands during a pandemic contains the hidden assumption that the therapy will work, which historically and empirically speaking, may be a bad assumption.
The problem of overestimating benefit is almost certainly magnified during the COVID pandemic. Around the world, scientists have thrown essentially any chemical they can think of at COVID-19. If we throw hundreds of potential drugs randomly towards a target, we shouldn’t be surprised that some hit the bullseye. The problem is that at least some of the options will hit the bullseye by chance alone. If 20 different drugs were tested in a single trial, and one happened to have a statistically significant result, we would know to be cautious. But that is exactly what is happening worldwide; the drugs just happen to be tested in separate trials. Since early 2020 it was obvious, given the sheer number of RCTs being run, that some COVID trials would be positive by chance alone.
When you combine the ongoing chance of harm from novel therapeutics with the increased risk of false positives during the COVID research frenzy, I think we need to maintain the same stringent scientific standards we always use to keep our patients safe.
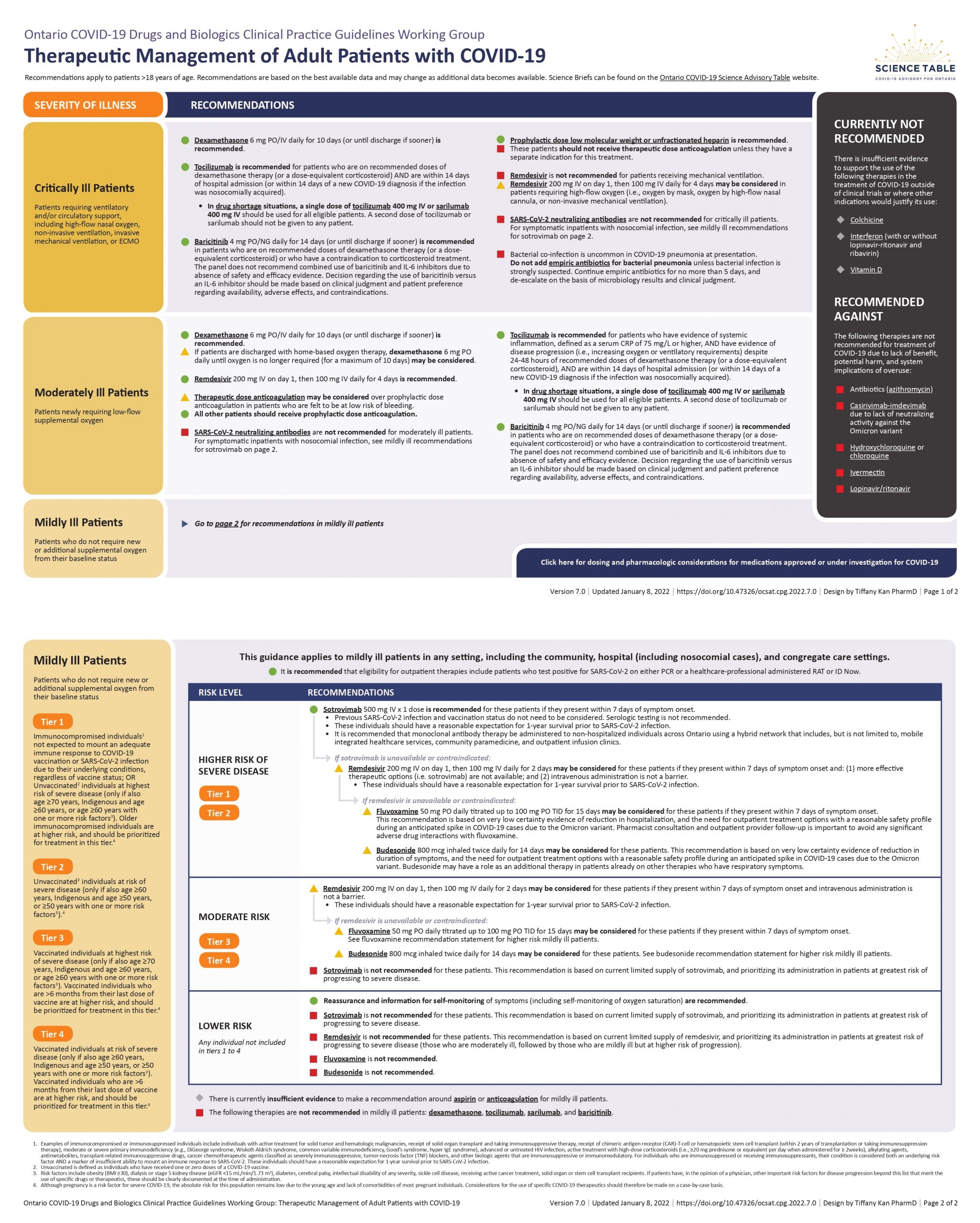
The Ontario Science Table recommendation
Budesonide is not recommended in moderate or critically ill patients (where we use systemic steroids).
Budesonide is not recommended in mildly ill patients with a low risk of deterioration.
Budesonide may be considered in mildly ill patients with moderate to high risk of deterioration (defined in the document), based on a low certainty of evidence.
(Full document available here)
The evidence for budesonide
Early in the pandemic, there was observational data that concluded that inhaled steroids were associated with an increased mortality from COVID in patients with asthma and COPD. (Schultze 2020) I argued at the time that this data was misleading. The association was almost certainly not causal, but instead the result of sicker patients receiving steroids. However, as a baseline when interpreting our RCTs, it is worth knowing that the observational data did not demonstrate a huge benefit from inhaled steroids.
The STOIC trial was a phase 2 open-label RCT that randomized 146 adult patients within 7 days of the onset of mild COVID-19 symptoms to 800 ug BID of inhaled budesonide or nothing. (Ramakrishnan 2021) Their primary outcome was a ‘COVID-19 related’ urgent care visit, emergency department assessment, or hospitalization, and was significantly reduced in the budesonide arm (15% vs 3%, p=0.009). The only objective outcome in the trial – proportion of days with an oxygen saturation less than 94% – was the same in both groups. There are a number of major problems with this trial that should make us very skeptical of the results. It was an unblinded trial with relatively subjective outcomes. The trial was stopped early (and not because of any pre-specified endpoints) which generally overestimates benefits, and leaves us with large confidence intervals. It was a very small trial, with only 11 events in the usual care arm and 3 in the treatment arm. They used a composite outcome which combines things of very different importance, and it appears to be somewhat different from the trial registry. Furthermore, they don’t even break down this composite outcome in the manuscript. I think only a single patient was admitted to hospital, but they don’t tell us which group that patient was in. More importantly, they use an inherently biased outcome. They didn’t look at ‘hospitalizations’ or ‘emergency department visits’. They only looked at those visits that the researcher thought were ‘COVID related’. That immediately eliminates any visits that could be related to medication side effects (which admittedly, with budesonide, should be pretty rare), and provides way too much subjectivity in an open label trial. Bottom line: I don’t trust the results of this trial at all. There are way too many sources of bias for the benefit to be believable.
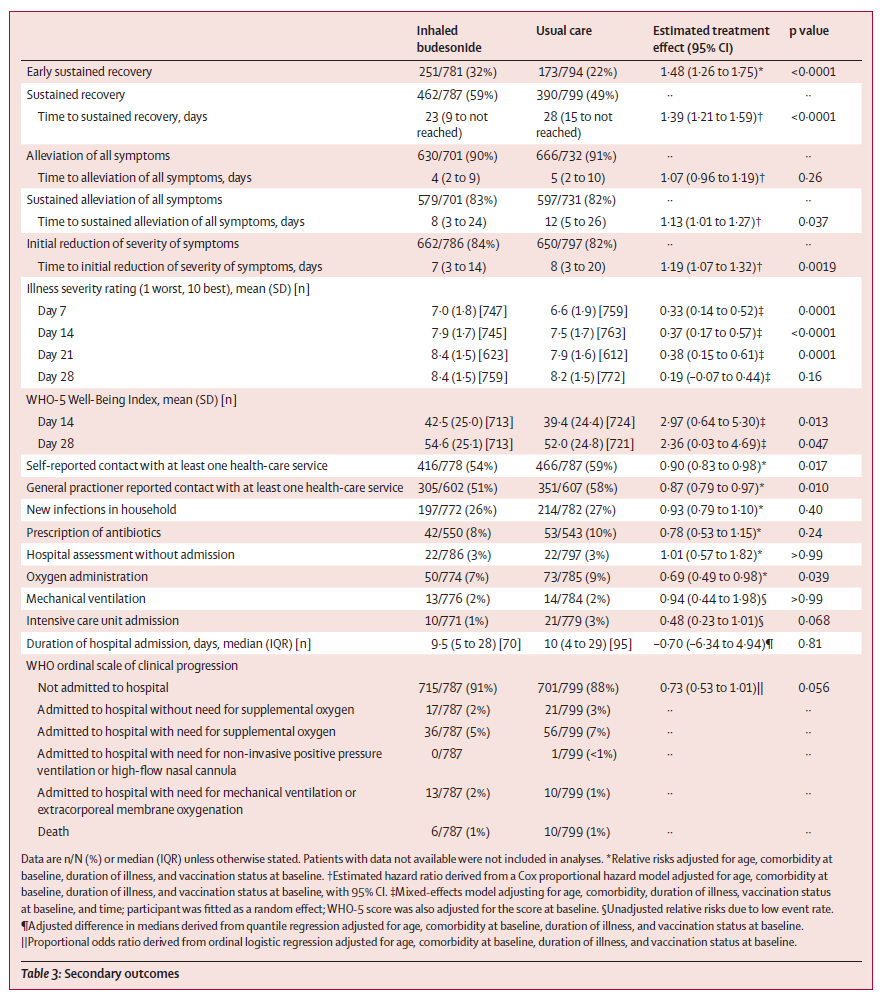
Budesonide was also studied as part of the adaptive platform PRINCIPLE trial in the UK. (Yu 2021) This is a multi-center open label RCT that randomized adults over 65 years of age, or over 50 years of age with co-morbidities, to inhaled budesonide (800 ug BID) or usual care. 1073 patients were randomized to budesonide. There were 2 primary outcomes (not ideal): self reported recovery and hospital admission or death due to COVID-19. The time to fist reported recovery was statistically better with budesonide (11.8 vs 14.7 days, absolute benefit 2.9 days, 95% CI 1.2-5.1 days). However, this was a subjective outcome in an unblinded trial, and so the benefit seen here is probably consistent with the expected placebo effect, rather than a real benefit from budesonide. Furthermore, this wasn’t the original planned primary outcome, but was added later after hospitalizations turned out to be lower than expected. In terms of hospitalizations due to COVID or death due to COVID, the other primary outcome, there was not a statistical difference between the two groups (6.8% versus 8.8%, ARR 2.0%, 95% CI -0.2 to 4.5%). Their Bayesian analysis suggests that there is likely a true statistical difference betwen the groups, but that has to be balanced against the many sources of bias in this trial that could example the difference. Looking down the long list of secondary outcomes, they all look very similar between the groups, even the bulk of the subjective symptom based outcomes. Again, the outcome of choice here was really bad. Allowing the researchers to choose which hospitalization and deaths were “due to COVID” in an unblinded trial is very problematic. It is also an outcome that no one cares about. We care about overall hospitalization and death rates, not just a subset. All cause mortality was identical in both groups. Unfortunately, this trial was also stopped early based on the statistically significant symptom results, increasing uncertainty about the more important clinical outcomes. Bottom line: For the original primary outcome, this was a negative trial, but hints at a possible benefit that should be followed up. We shouldn’t trust the minimal subjective symptom improvement in an open label trial. Therefore, once again, I don’t see any reason to prescribe budesonide at this time, based on this data.
Other comments
The patients in both of these trials were almost all unvaccinated. That is incredibly important to consider when trying to extrapolate these results, as vaccinated patients usually have milder symptoms and are less likely to be hospitalized. Therefore, for most of the patients I am seeing, the benefit (if any) will almost certainly be smaller than the purported benefit seen in these trials.
Bottom line
These trials are very unconvincing. The PRINCIPLE trial may have just ended up under-powered for important clinical outcomes, but it is still an open label trial at very high risk of bias. Based on these trials, I think it is unlikely that budesonide has any important benefit in COVID-19. It is a relatively safe medication, but there are still adverse events and costs associated with the drug. I do not prescribe it routinely, even for the higher risk groups that the Ontario Science table says it “may be considered”. However, in the occasional very symptomatic patient, I have tried it, knowing full well that I was probably just prescribing an expensive placebo.
Other FOAMed
Other First10EM COVID therapeutics updates can be found here
Ontario Science Table Recommendations
REBEL EM: The STOIC Trial: Inhaled Budesonide in the Treatment of Early COVID-19
REBEL Cast Ep103: Outpatient COVID-19 Therapy
References
Ramakrishnan S, Nicolau DV Jr, Langford B, Mahdi M, Jeffers H, Mwasuku C, Krassowska K, Fox R, Binnian I, Glover V, Bright S, Butler C, Cane JL, Halner A, Matthews PC, Donnelly LE, Simpson JL, Baker JR, Fadai NT, Peterson S, Bengtsson T, Barnes PJ, Russell REK, Bafadhel M. Inhaled budesonide in the treatment of early COVID-19 (STOIC): a phase 2, open-label, randomised controlled trial. Lancet Respir Med. 2021 Jul;9(7):763-772. doi: 10.1016/S2213-2600(21)00160-0. Epub 2021 Apr 9. Erratum in: Lancet Respir Med. 2021 Jun;9(6):e55. PMID: 33844996
Yu LM, Bafadhel M, Dorward J, Hayward G, Saville BR, Gbinigie O, Van Hecke O, Ogburn E, Evans PH, Thomas NPB, Patel MG, Richards D, Berry N, Detry MA, Saunders C, Fitzgerald M, Harris V, Shanyinde M, de Lusignan S, Andersson MI, Barnes PJ, Russell REK, Nicolau DV Jr, Ramakrishnan S, Hobbs FDR, Butler CC; PRINCIPLE Trial Collaborative Group. Inhaled budesonide for COVID-19 in people at high risk of complications in the community in the UK (PRINCIPLE): a randomised, controlled, open-label, adaptive platform trial. Lancet. 2021 Sep 4;398(10303):843-855. doi: 10.1016/S0140-6736(21)01744-X. Epub 2021 Aug 10. Erratum in: Lancet. 2021 Aug 18;: PMID: 34388395
Photo by Annie Spratt on Unsplash


{kind=link}
3 thoughts on “COVID therapy evidence updates: budesonide”
I totally agree with your “philosophical view” on this one.
Are you aware of this meta-analysis https://www.medrxiv.org/content/10.1101/2021.11.04.21265945v1.full.pdf+html by Todd Lee et al? It includes STOIC and PRINCIPLE, so it inherently suffers from the same bias. I don’t know the other trials (CONTAIN and Covid Pharma).
I had not seen this meta-analysis, probably because it hasn’t been published yet.
The other two RCTs included didn’t use budesonide, which is why I missed them for this summary. Both were negative based on the abstract. I don’t think outcomes will be different with different inhaled steroids though, so I will provide an updated blog post when I have time that covers all inhaled steroids.
Thanks for the comment
Very interesting.
Your way is very analytical and accurate.
Thanks for sharing your experience which is just amazing