
Morgenstern, J. Fluvoxamine for COVID?, First10EM, November 8, 2021. Available at:
https://doi.org/10.51684/FIRS.123107
Might we have an effective pill for the outpatient management of COVID-19? One might have assumed that this post was going to be about molnupiravir, as it has now been weeks since we saw incredibly enthusiastic press releases about this apparent ‘miracle cure.’ Unfortunately, that data still has not been released (which makes me very suspicious about the value of molnupiravir, because data that good could be published in an instant.) Instead, we see another repurposed medication trying to make headway against COVID – fluvoxamine. I know COVID has left many people feeling depressed, but I was surprised to hear that fluvoxamine might be beneficial in the treatment of outpatients with COVID-19. Let’s look through the study, to see if the outcomes are as good as reported.
The paper
Reis G, Dos Santos Moreira-Silva EA, Silva DCM, et al. Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial. Lancet Glob Health. 2021 Oct 27:S2214-109X(21)00448-4. doi: 10.1016/S2214-109X(21)00448-4 PMID: 34717820 NCT04727424
The Methods
The TOGETHER trial is a randomized, adaptive platform trial that has looked at a number of potential treatments for high risk adult outpatients with COVID-19 across 11 centers in Brazil.
Patients
These are adults with acute COVID-19 (less than 7 days from symptoms onset) being treated as an outpatient, and with at least 1 high risk feature:
- Diabetes
- Hypertension on at least 1 medication
- Cardiovascular disease
- Symptomatic lung disease
- Obesity
- Transplant
- Stage IV chronic kidney disease or dialysis
- Immunosuppressive therapy
- Active cancer
- Age over 50
- Unvaccinated status
Exclusions included a negative COVID test, vaccination against COVID, dyspnea due to other respiratory disease, current use of SSRI, uncontrolled psychiatric condition, and positive pregnancy test. (If you decide to start prescribing fluvoxamine, there are many other exclusion criteria listed on clinicaltrials.gov that do not make it into the manuscript.)
Intervention
Fluvoxamine 100mg orally twice a day for 10 days.
Comparison
Placebo.
Outcome
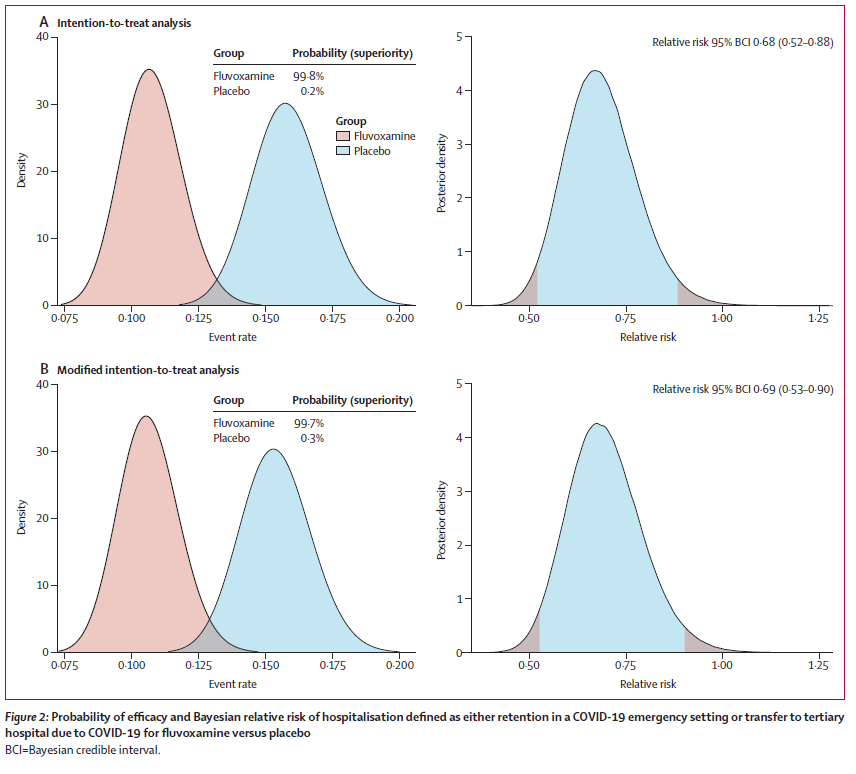
The primary outcome was a composite endpoint of admission to hospital due to COVID-19-related illness, or observation in the emergency department for more than 6 hour due to COVID-19-related illness, within 28 days of randomization.
The Results
They included 1497 patients.The median age was 50, and 58% were women. There is a reasonable mix of comorbidities, although obesity rates are high (50%) and vaccination rates really low (6%).
There was a decrease in their primary outcome with fluvoxamine (16% vs 11%, RR 0.69, 95% Bayesian credible interval 0.52-0.88). This would give a number needed to treat of approximately 20 to prevent one 6 hour ED observation or hospitalization from COVID-19, if real.
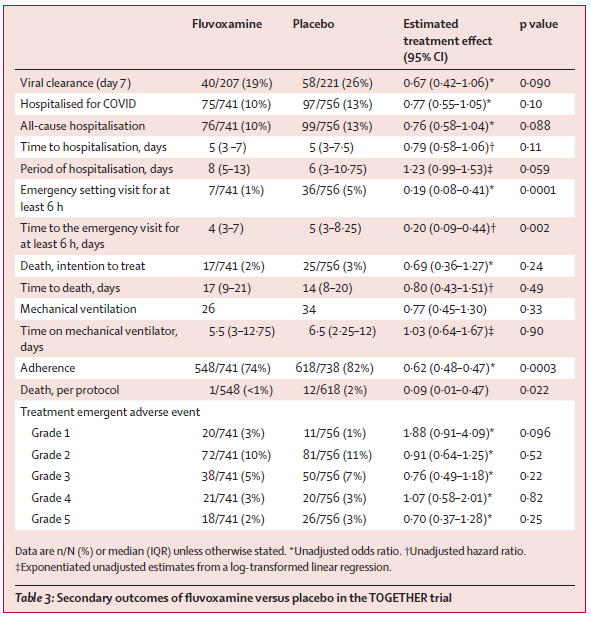
There was no change in mortality (2% vs 3%, p=0.24).
Hospitalizations were not statistically different between the groups (10% vs 13%, p=0.1). There was a statistically significant difference in the number of patients who were observed in the emergency department for 6 hours (1% vs 5%, p=0.0001).
There was no difference in viral clearance at day 7, mechanical ventilation, number of days ventilated, or number of days hospitalized.
84 participants stopped fluvoxamine and 64 participants stopped placebo owing to issues of tolerability. The difference was statistically significant.
My thoughts
It would be great news if fluvoxamine decreased hospitalizations or improved other outcomes from COVID-19. It is a cheap and widely available medication, and we don’t really have any practical, effective outpatient treatments for COVID at this point. Like many of the agents being tested against COVID, fluvoxamine may mechanistically act as an anti-inflammatory, and may also have anti-viral tests, but as we have seen over and over again, petri dish results don’t count for much. There is one prior RCT of fluvoxamine against COVID. It was small, and had significant flaws, but it did demonstrate a statistically significant decrease in (primarily subjective) clinical deterioration with fluvoxamine. (Lenze 2020)
On my first pass through this paper, I was willing to leave a little optimism in my conclusion. However, the more times I read through the manuscript, the less I trust the results. There are a number of significant problems with this paper that should limit your confidence in the results, and leave me relatively convinced that a follow-up study would be negative.
There are issues with generalizability. All patients received ‘standard care’ in addition to the study drug. This might be problematic, as the trial took place in Brazil, and my understanding is that a lot of treatments that we wouldn’t consider ‘standard’ in North America were used routinely throughout the pandemic in Brazil. Unfortunately, this manuscript does not discuss other medications that patients received.
Generalizability is further limited by the vaccination status of participants. (This was somewhat confusing, as vaccination status was included in both the inclusion and exclusion sections, which seems somewhat contradictory. I think this is because they changed their inclusion criteria part way through the trial.) However, the important point is that almost no one in this trial was vaccinated, which will limit the applicability of these results in other settings. I think this is an incredibly important distinction to consider, as we are talking about treating patients healthy enough to be treated as an outpatient. Vaccinated outpatients are expected to have good outcomes. (Vaccination decreases the rate of hospitalization and death.) Therefore the potential benefit will be significantly smaller in a vaccinated population, but with all the same risks.
(This is a topic we are going to have to grapple with if COVID becomes endemic, as it is expected to do. Once endemic, the morbidity and mortality of COVID should be much lower than during the pandemic. Evidence gathered during the pandemic will therefore probably overestimate benefits in a post-pandemic world. There will be no appetite for it, but scientifically, we really should be repeating these RCTs in a few years to see if the results hold up.)
One of the big red flags in this study was that they changed the primary outcome, and they did so to add a seemingly meaningless endpoint. Based on the registry, I believe the original primary outcome was need for hospitalization. The current primary outcome combines hospitalization with the need for a 6 hour observation in the emergency department. I have no idea why a 6 hour observation would be an important negative outcome, even with their justification that the threshold for hospitalization was higher due to the pandemic. If anything, this sounds like a positive outcome. These patients were observed and it was determined that the patients were well enough to go home. Why would you combine that with hospitalization? And why would you prescribe a drug to prevent ED observations? Unfortunately, when they break up the composite outcome, there was not a statistical difference in hospitalization, and only a statistical difference in ED observations. Therefore, the entire ‘benefit’ reported here may not be so beneficial at all.
(ED visits are also much more likely to be biased than hospitalization. One could imagine that the SSRI made symptoms more tolerable, or made patients more drowsy, so that they didn’t show up to the emergency department, but were still just as sick.)
Unfortunately, the primary outcome gets even worse. They did not look at the rate of hospitalization. They looked at the rate of hospitalization due to COVID-19. This is the equivalent of using disease specific mortality, and completely biases the results from the outset. If a patient was admitted for suicidal ideation, it wouldn’t count towards this outcome. If a patient was admitted with serotonin syndrome, it wouldn’t count towards this outcome. It is a completely subjective measure that allows the researchers to completely exclude the harms of treatment and retain only the benefit, which is clearly unacceptable. In this case, it appears that the researchers got lucky, because all cause hospitalization was essentially identical to COVID-specific hospitalization, but this is a very biased study design.
I find their manuscript difficult to follow, but I think their primary statistical analysis also introduces bias. It seems that in order to be included in the intention to treat analysis, you had to have received the full 10 days of treatment before your outcome (hospitalization) was counted. There was a ‘modified intention to treat analysis’ that included patients who had received 24 hours of treatment prior to their primary outcome. Again, it didn’t seem to matter in this trial, but this design is likely to be biased in favour of any treatment. Admissions for adverse events are more likely soon after the therapy is started. By ignoring outcomes that occur in the early phases of treatment, you downplay potential harms. Again, based on the numbers they present, it doesn’t seem like this happened, but it isn’t clear exactly what numbers make it into table 3, and the trial methodology seems problematic to me.
I don’t think this study passes our usual bar for accepting a new therapy. Whether that bar should change during a pandemic is a matter of debate, but I think probably not.
There are numerous reasons to think these results might not be replicable in a follow-up study, aside from the baseline fact that very few of our medical trials are replicable. Within this same trial, many different agents were tested against COVID (the rest of which were negative). If these results were all written up within the same manuscript, we would probably demand statistical adjustment for multiple hypothesis testing, but because they are broken into separate publications, we forget about the fragility of our statistics when we take a shotgun approach to hypothesis testing. I wrote about this problem at the beginning of the pandemic. If we test enough hypotheses, some will be positive by chance alone. COVID has set the perfect stage for false positive results. We are literally testing hundreds of hypotheses all at the same time. Even if all are completely wrong, we would expect that some would be positive by chance alone. (This is probably made worse by adaptive study designs, which don’t have a set endpoint, but instead check their data multiple times to determine if a statistical threshold has been met. These are interesting designs, but this practice was always considered p-hacking in the past, and needs some kind of adjustment if it is going to be used.) The human tendency will be to jump on a treatment as soon as we see a ‘positive’ RCT, but we need to keep in mind the fragility of these statistics. Replication is the key to science, and no treatment should become standard based on a single RCT.
Of the many tested treatments, I think fluvoxamine is among the most likely to be a false positive. At least some of the other agents started their lives as antivirals or immune modulators. If I had asked you in 2019 how likely it is that an SSRI would have a clinically important benefit in the management of a viral illness, I think you would have guessed pretty close to 0%. Therefore, even if you are overwhelmed by these results, Bayesian reasoning will tell us that it is still much more likely that fluvoxamine doesn’t work than it does.
And I am not sure how anyone could be overwhelmed by these results. There was no change in morality. The change in the composite primary outcome was driven primarily by a decrease in 6 hour emergency visits, which is barely even an important clinical outcome.
Bottom line
This blinded, multicenter RCT concludes that fluvoxamine decreases the risk of a 6 hour ED observation or hospital admission from COVID-19, but there are numerous reasons to doubt that outcome, and even if true, it is not clear that this truly represents a patient important benefit that outweighs the harms of treatment.
Other FOAMed
REBEL EM: The TOGETHER Trial: COVID-19 and Fluvoxamine Take Two
REBEL EM: COVID-19 Update: An Interesting Study on Serotonin Antagonism
References
Lenze EJ, Mattar C, Zorumski CF, Stevens A, Schweiger J, Nicol GE, Miller JP, Yang L, Yingling M, Avidan MS, Reiersen AM. Fluvoxamine vs Placebo and Clinical Deterioration in Outpatients With Symptomatic COVID-19: A Randomized Clinical Trial. JAMA. 2020 Dec 8;324(22):2292-2300. doi: 10.1001/jama.2020.22760. PMID: 33180097; PMCID: PMC766248
Reis G, Dos Santos Moreira-Silva EA, Silva DCM, et al. Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial. Lancet Glob Health. 2021 Oct 27:S2214-109X(21)00448-4. doi: 10.1016/S2214-109X(21)00448-4 PMID: 34717820 NCT04727424



6 thoughts on “Fluvoxamine for COVID?”
Thank you for this thorough writeup!
One q: in the paper they justify adding the “6 hour in ED” outcome as they were so overrun that they didn’t have hospital beds, and patients were essentially receiving all their care in these COVID emergency centres. Do you think that helps rationalize this as a valid proxy outcome for hospitalizations, or is it still too difficult to parse out “would have been admitted if they could”? Thanks!
Thanks for the question
That justification doesn’t make a lot of sense to me. If the patient was sick enough to need hospitalization, they wouldn’t have been better 6 hours later. If anything, it raises questions about their criteria for hospitalization. Perhaps a large number of the hospitalized patients could also have just been sent home? That is the problem with subjective outcomes. With no change in the more objective outcomes like mortality, it makes these outcomes really hard to believe.
If the researchers really thought that the pandemic had changed the standard of care, they should have been explicit in describing that in the paper. If these patients with 6 hour observations had oxygen saturations in the 80s, and they decided to still send them home, that would be important information to know. However, as the paper is presented, there is absolutely no information, so the best guess is that the brief observation is a completely inconsequential outcome.
And thank you for the reply!
Not that it really changes most of your points, but the endpoint was at LEAST 6 hours in ED:
“Our primary outcome is hospitalisation defined as either retention in a COVID-19 emergency setting for more than 6 h or transfer to tertiary hospital due to COVID-19. … Specialised emergency settings were developed to respond to the Brazilian epidemic and we considered prolonged observation and treatment in these settings as equivalent in importance to hospitalisation as many patients who typically would be hospitalised were prevented from doing so owing to hospital over-capacity. In our trial, 87% of all primary outcome events eventually resulted in transfer to a tertiary hospital.”
You are absolutely right though, they should still have been far more detailed in describing specific severity criteria which would have been far more relevant than the ED observation time (ie anything that could be generalized to other countries in terms of requiring admission).
Thanks again for the writeup!
I agree.. I should have made that more explicit
It is possible that these patients were observed for days in the ED but never admitted. However, if that was the case, I sort of assume they would have told us. At very least, the paper probably should have included the median length of observation.
Not as surprised as you were that there was no change in morality, as you note in your final paragraph. Antidepressants are good, but they don’t make you good (or bad, I guess).