
Morgenstern, J. COVID therapy: There is still no evidence for nirmatrelvir/ritonavir (Paxlovid), First10EM, January 22, 2022. Available at:
https://doi.org/10.51684/FIRS.124914
I have avoided COVID therapies for a while, because so many people are already covering the topic, and honestly I am a little sick of COVID. However, with the OMICRON wave, everyone seems to have questions about therapies for COVID, so a quick evidence review seems appropriate. This article will cover the evidence for nirmatrelvir/ritonavir (paxlovid) in COVID-19.
It is going to be a very short article. There is no evidence at all. At least, none available for the general medical or scientific communities to review.
Despite press releases hyping this medication months ago, the EPIC-HR trial that evaluated this drug combination has not been published anywhere yet, even in pre-print. I find that concerning. If the results were as good as the press releases claim, this would have been accepted into the New England Journal of Medicine the very same day. It is a big red flag that this study has not been published, and suggests to me some significant issues with the methods or results.
We do know a few things about the trial based on a non-peer reviewed press release by the company. We know the trial was stopped early, with less than half of the planned participants. We know that the composite outcome of death and hospitalization was reported to be lower in the nirmatrelvir/ritonavir group (7.0% vs 0.8%). We know there were 10 deaths in the placebo group as compared to 0 in the treatment group. (Pfizer press release available here.) However, all these numbers are based on a press release from the company trying to sell us the drug, with literally billions of dollars at stake.
There is no way that people should be clamoring to get this drug or willing to pay massive amounts of money for it until we see real data supporting its use. Unfortunately, that is not how governments work, and we have already seen governments around the world send dump trucks full of money to Pfizer’s campus just to be put on a waiting list for this drug.
I hope the results are as good as advertised. I really do. I really hope this doesn’t turn into yet another multi-billion dollar waste like the Tamiflu fiasco. But the delay in publication really makes it seem like we may have once again allowed the wool to be pulled over our eyes.
You can find more information about this drug in the regulatory submissions:
Some of the data in these documents looks promising, but we are still missing key information. I am optimistic the published data will show a benefit, but I anticipate there will be problems with the trial that aren’t yet obvious.
Hopefully I will be able to replace this post with an update in the near future, and hopefully my cynicism about the inner workings of drug companies turns out to be wrong this one time.
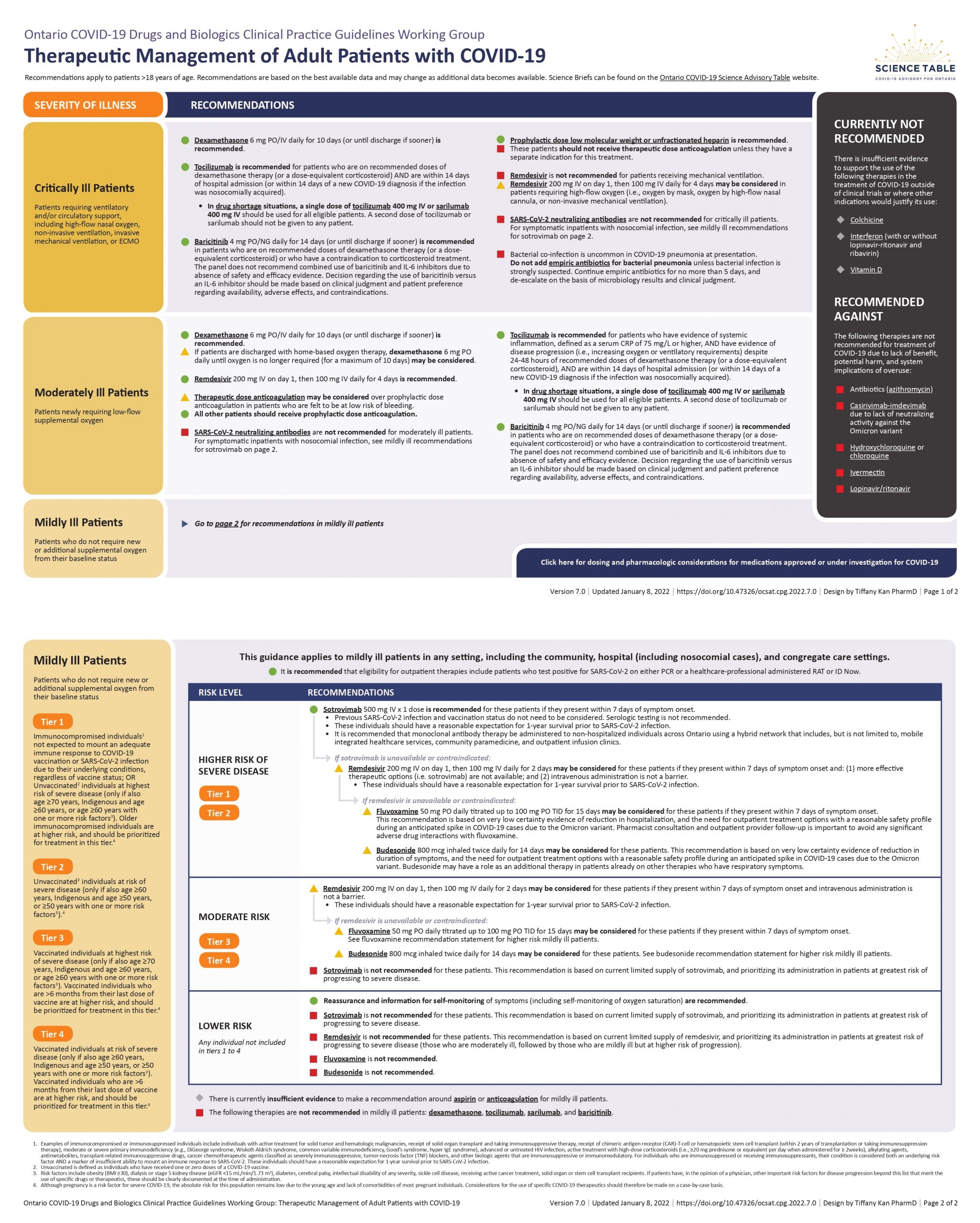
The Ontario Science Table recommendation
Not recommended in moderate to severely ill patients.
In high risk mildly ill patients, it is recommended as a second line only if sotrovimab and remdesivir are unavailable or contraindicated. This is noted to be an interim recommendation pending publication of the trials, and with the most small print of any recommendation this group has made.
(Recomendations available here)
Bottom line
We should not be recommending, prescribing, or purchasing a drug until the data supporting it is seen by the scientific world.
Other FOAMed
Other First10EM COVID therapeutics updates can be found here
Ontario Science Table Recommendations
ALiEM: Oral Antivirals for Treatment of Mild-Moderate COVID-19 Infection
References
Do you count a Pfizer press release as a reference?
Photo by Annie Spratt on Unsplash


{kind=link}
6 thoughts on “COVID therapy: There is still no evidence for nirmatrelvir/ritonavir (Paxlovid)”
But if it works and you do not prescribe then many will die .
It is a bit risk .
Everything is travelling so fast it is hard to do huge trials .
Which if following the treatment / placebo model are severe cruelty with placebos dying .
I think the problem is that you are assuming it is more likely to work than not, when in fact it is much more likely to be the other way around
Ok
We have to wait
It is being rolled out
I’d take it if I was immunosuppressed and at risk
Many drug interactions can be adjusted .
With Omicron some unvaccinated are very ill and have passed .
I think this needs to be put a little more simply.
I, an emergency doctor, have produced a drug and tested it. It’s called Zakimab. In the 4000 people who got it, 1 died. In 4000 people who didn’t get it, 72 died. Obviously my drug works phenomenally.
I will be selling it for $20 a dose. Please let me know if you want to be added to the waitlist.
—basically what Pfizer have done, except instead of a little comment on a blog post, it’s an advert in a newspaper.
Is this the trial? https://pubmed.ncbi.nlm.nih.gov/35172054/