I have been working on a deep dive into steroids for community acquired pneumonia for a long time. The content of that evidence review was just recorded as an episode of the EM Cases Journal Jam, which will be out soon. My focus was on steroids for community acquired pneumonia, but it is 2020, so of course we have to talk about COVID. While we wait for the main Journal Jam episode, I thought I would publish the quicker review on steroids for the treatment of COVID-19. (Plus, if I sit on this write up for even another week, it will likely become obsolete.)
By now, everyone knows about dexamethasone and the RECOVERY trial, but there are a few other RCTs, so let’s do a quick recap.
The RECOVERY trial
- A pragmatic, open-label, multi-centre RCT from 176 hospitals in the United Kingdom
- 6425 hospitalized patients
- Dexamethasone 6 mg daily up to 10 days versus usual care
- Mortality was lower in the dexamethasone group (21.6% vs 24.6%; OR 0.83; 95% CI 0.74-0.92, P<0.001)
There are a few key things to know about this trial. The benefit seems to be primarily among the sickest patients. Patients who weren’t on oxygen and those who had fewer than 7 days of symptoms didn’t seem to benefit. The trial isn’t blinded which significantly increases the risk of bias. You can read more about this trial in the main post.
The CoDEX trial (Tomazini 2020)
- An investigator-initiated, multicenter, randomized, open-label, clinical trial in 41 intensive care units (ICUs) in Brazil
- 299 adult ICU patients with COVID-19 receiving mechanical ventilation and within 48 hours of meeting the criteria for severe ARDS
- Dexamethasone 20 IV daily for 5 days followed by 10 mg IV daily for 5 days (or until ICU discharge) was compared to standard care.
- Dexamethasone results in more days free from mechanical ventilation in the first 28 days (6.6 vs 4.0 days, difference 2.26, 95% CI 0.2-4.38, p=0.04)
- The difference in mortality was not statistically significant (56% vs 62%, p=0.85).
The trial isn’t close to being powered for a mortality difference, but the 6% difference between groups could be important. That being said, this is a much smaller benefit than we saw in the RECOVERY trial, and the outcomes are much worse overall. They discuss this somewhat in the paper and it may be a function of the ability of Brazil’s medical system to cope with the COVID pandemic.
35% of the standard care group actually received at least 1 dose of steroids, which would bias the results towards the null hypothesis.
The p value of 0.04 is way overrepresented in the medical literature, which doesn’t mean anything specific for this trial, but the number of trials with this number is basically impossible.
The CAPE COVID trial (Dequin 2020)
- This is embedded in the larger ongoing RCT looking at hydrocortisone in community acquired pneumonia (the CAPE COD trial)
- A multicenter, randomized, placebo controlled trial from 9 ICUs in France
- 149 adult COVID patients with acute respiratory failure, and 1 of 4 markers of severity (mechanically ventilated, PaO2:FiO2 less than 300, pulmonary severity index less than 13)
- A continuous infusion of low dose hydrocortisone (200 mg/day for 7 days, followed by 100 mg/day for 4 days, then 50 mg/day for 3 days) was compared to placebo.
- There was not a statistically significant difference in mortality, but it happened in 15% of the treatment group and 27% of the placebo group (p=0.057)
- There was also not a statistical difference in the other primary outcome of treatment failure at 21 days (42% vs 51%, p=0.29)
This is a ‘negative trial’, but is clearly too small to help us much. There are large differences between the groups, which – if real – would be clinically important. The trial was stopped early.
A big plus is that this was a placebo controlled trial, but steroids can still have effects that can result in clinical unblinding, creating potential confounders in the data. (This will be a bigger point when we come back to the data on steroids for community acquired pneumonia.)
You aren’t supposed to have more than 1 primary outcome. Mortality is the main outcome for the bigger CAP trial, but they added treatment failure for the COVID sub-trial.
They stopped their trial early, based on the logic that the results of the RECOVERY trial made this trial unethical. I think that is a big mistake. I have discussed it at length elsewhere on the blog, but a single trial cannot define truth, and therefore cannot eliminate equipoise. Furthermore, these trials are looking at different agents in somewhat different contexts. Stopping this trial early just means that we will forever be in the dark when treating patients, and that might really matter. If we run out of dexamethasone, are we really sure that hydrocortisone is as good? In this scenario, my guess is yes – but we really need to stop this practice of terminating trials just because 1 trial reported promising results, especially when those trials have significant flaws like a lack of blinding. It is bad for patients.
The REMAP-CAP trial (Angus 2020)
- REMAP-CAP is an ongoing, international, multicentre, open-label, pragmatic, adaptive platform trial designed to look at different treatment options for community acquired pneumonia. That platform was adapted to randomize patients with COVID to different doses of hydrocortisone at 121 clinical sites in Australia, Canada, France, Ireland, the Netherlands, New Zealand, the United Kingdom, and the United States.
- 614 adult ICU patients with severe COVID-19 requiring respiratory or cardiovascular support.
- There were 3 treatment arms: hydrocortisone 50mg IV every 6 hours for 7 days, hydrocortisone 50mg IV every 6 hours only while there were signs of overt shock, and no hydrocortisone.
- There were no statistical difference in mortality. 30% of the fixed dose group, 26% of the shock-only treatment group, and 33% of the control group died. Based on their Bayseian assumptions, they think there is a 54% chance that fixed dose hydrocortisone is better than standard care and a 62% chance that shock only treatment is better than standard care.
- Treatment failure was not statistically different. The median organ support free days was 0 in all groups.
A big problem with this trial is that hospitals could decide locally if there was equipoise, and therefore 21% of sites refused to randomize patients to the control group. I think this gives you a general sense of the belief in the community that steroids will work, which is likely to introduce significant bias in all these open label trials.
Like the last trial, they changed their primary outcome from mortality to “respiratory and cardiovascular support-free days up to day 21”. I think this is a problem, as it is a much more subjective outcome in an open label trial.
15% of the ‘no steroid’ group did receive at least 1 dose of hydrocortisone.
I am a big fan of presenting the results of Bayesian calculations, but those calculations are based on assumptions about the priors that I am missing when reading the article.
This trial was also stopped early based on the results of the RECOVERY trial, which again seems like a mistake.
Ongoing trials
There are a few RCTs that are ongoing or haven’t been published yet. I will update this post as new trials are published.
DEXA-COVID NCT04325061
Steroids-sARIO NCT04244591
COVID STEROID NCT04348305
COVIDICUS NCT04344730
Plus a few trials on the Chinese trial registry (I think, because I can’t read the registry)
Meta-Analysis
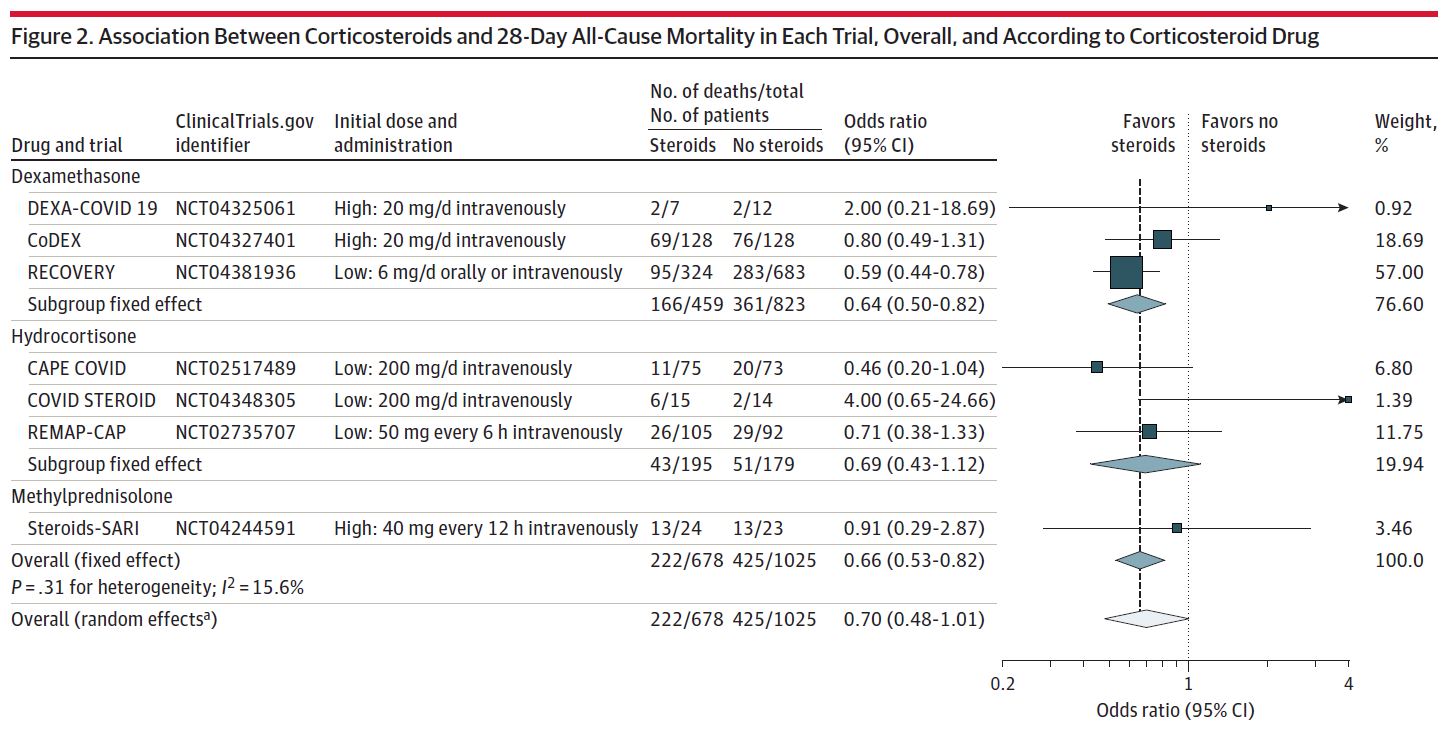
There is a really interesting meta-analysis that includes data from the 4 studies discussed above, but also included preliminary data from the ongoing trials. (WHO REACT group 2020) They included any trial that enrolled critically ill patients with COVID-19 and compared steroids to no steroids. They include data from 7 RCTs and a total of 1703 patients. The steroids prescribed were dexamethasone, hydrocortisone, or methylprednisolone. Combined, steroids were associated with a lower mortality (odds ratio 0.66, 95% CI 0.53-82). The results look similar for all steroids, but are only statistically significant for dexamethasone.
Discussion
There is a lot of optimism for steroids. I think that is well represented in the fact that 1 in 5 hospitals would not randomize a COVID-19 patient to a no steroid group, even though there was no evidence of benefit at the time. Given that 3 out of 4 of these trials were open label, we need to be very careful about the role that optimism may have played in shaping these results.
The fact that these trials are open label is a problem, but confounding could have been an issue even if they were blinded. Steroids change a lot of clinical parameters. They will pretty consistently improve vital sign numbers, and we use those vital signs to make a lot of decisions, including prognostic decisions that can influence withdrawal of care. We like to think that death is a pretty objective outcome, but we have to remember how much control we have over death in modern ICUs. In most ICU studies that report it, the vast majority of patients die after a decision to withdraw care. If that decision is influenced by the therapy being studied, we might be looking at a self-fulling prophecy.
Although I think most of the bias in these trials is likely to make the results look more favourable than they really are, there was a significant amount of crossover between the groups. In particular, a lot of patients in the control group ended up getting steroids anyway. Thus, the comparison is between steroids for everyone and steroids for some, which would diminish any true benefit from steroids.
It is a shame that all the trials except RECOVERY were stopped early. It leaves them under-powered. It means that both trials of hydrocortisone were ‘negative’ despite promising numbers. It leaves us with questions. Is hydrocortisone as good as dexamethasone? Exactly which patients need to be treated? What are the harms? Completing these studies would have provided a tremendous benefit. Instead, we will now experiment on our patients without the benefit of systematically following the results.
Bottom line
Unlike so many of these evidence reviews, this one has a positive conclusion. Steroids decrease mortality in sick COVID patients. I think we can be moderately certain about that conclusion based on the available results. There are still a lot of questions, but for now it seems like any steroid is likely to work. Steroids should be given to sick patients – usually defined as those requiring oxygen.
Other FOAMed
Dexamethasone for COVID: The RECOVERY trial
REBEL EM – It’s Raining Steroids in COVID-19: REMAP-CAP, CoDEX, & CAPE COVID
References
Angus DC, Derde L, Al-Beidh F, Annane D, Arabi Y, Beane A, et al. Effect of Hydrocortisone on Mortality and Organ Support in Patients With Severe COVID-19: The REMAP-CAP COVID-19 Corticosteroid Domain Randomized Clinical Trial. JAMA. 2020 Oct 6;324(13):1317-1329. doi: 10.1001/jama.2020.17022. PMID: 32876697; PMCID: PMC7489418.
Dequin PF, Heming N, Meziani F, Plantefève G, Voiriot G, et al; CAPE COVID Trial Group and the CRICS-TriGGERSep Network. Effect of Hydrocortisone on 21-Day Mortality or Respiratory Support Among Critically Ill Patients With COVID-19: A Randomized Clinical Trial. JAMA. 2020 Oct 6;324(13):1298-1306. doi: 10.1001/jama.2020.16761. PMID: 32876689
RECOVERY Collaborative Group, Horby P, Lim WS, Emberson JR, Mafham M, et al. Dexamethasone in Hospitalized Patients with Covid-19 – Preliminary Report. N Engl J Med. 2020 Jul 17:NEJMoa2021436. doi: 10.1056/NEJMoa2021436. Epub ahead of print. PMID: 32678530
Tomazini BM, Maia IS, Cavalcanti AB, Berwanger O, et al; COALITION COVID-19 Brazil III Investigators. Effect of Dexamethasone on Days Alive and Ventilator-Free in Patients With Moderate or Severe Acute Respiratory Distress Syndrome and COVID-19: The CoDEX Randomized Clinical Trial. JAMA. 2020 Oct 6;324(13):1307-1316. doi: 10.1001/jama.2020.17021. PMID: 32876695
WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group, Sterne JAC, Murthy S, Diaz JV, et al. Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis. JAMA. 2020 Oct 6;324(13):1330-1341. doi: 10.1001/jama.2020.17023. PMID: 32876694
Morgenstern, J. Steroids for COVID-19, First10EM, December 7, 2020. Available at:
https://doi.org/10.51684/FIRS.52196



4 thoughts on “Steroids for COVID-19”