
Morgenstern, J. COVID therapy evidence updates: molnupiravir, First10EM, January 19, 2022. Available at:
https://doi.org/10.51684/FIRS.124834
I have avoided COVID therapies for a while, because so many people are already covering the topic, and honestly I am a little sick of COVID. However, with the OMICRON wave, everyone seems to have questions about therapies for COVID, so a quick evidence review seems appropriate. This article will cover the evidence for molnupiravir in COVID-19.
A philosophical interlude
If this is the first post in this series that you are reading, it might be worth reading the philosophical interlude from part 1 of the series which explains why my conclusions sometimes differ from those of the Ontario Science Table and others.
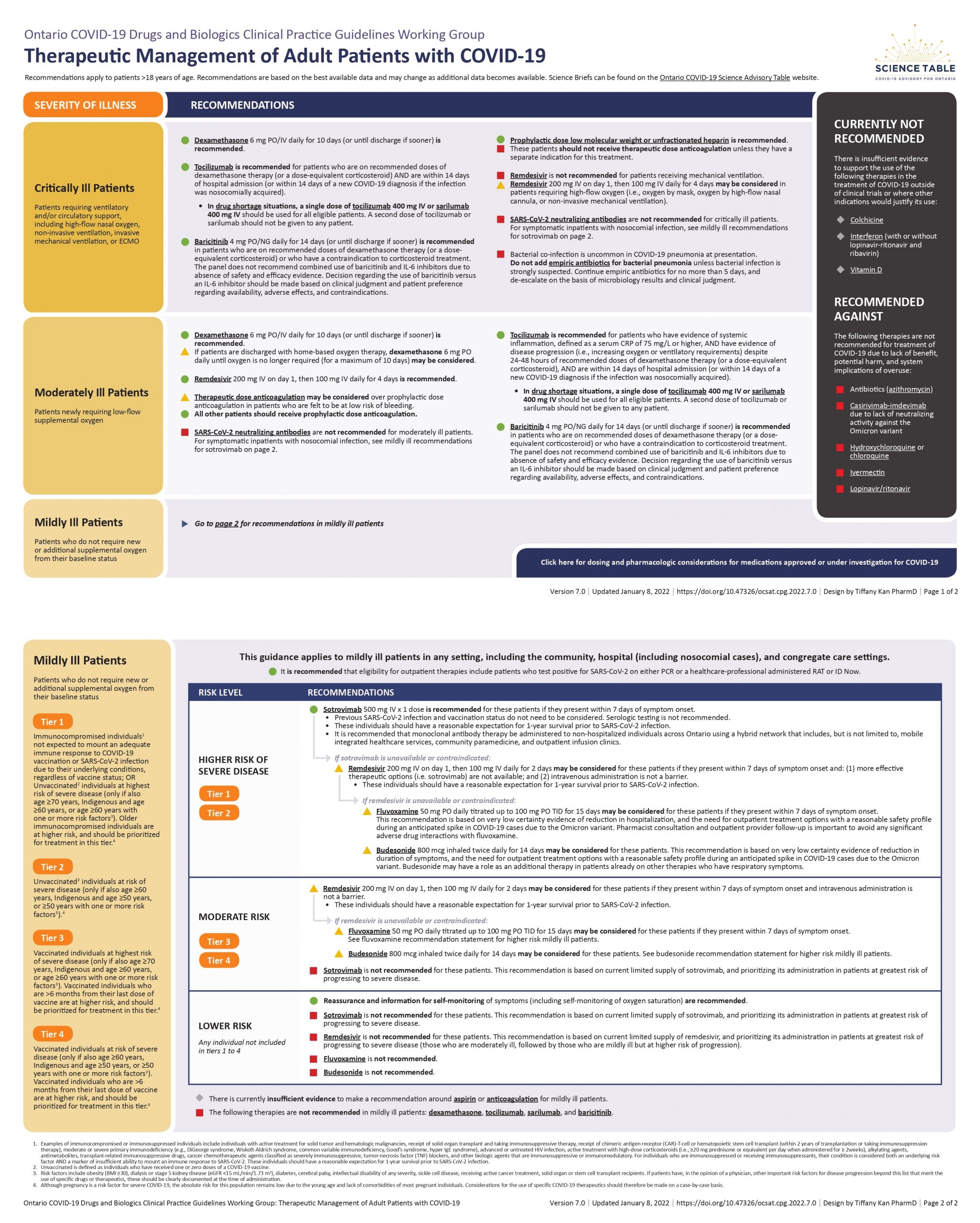
The Ontario Science Table recommendation
Not available in Canada, and so no recommendation at this time.
The evidence for molnupiravir
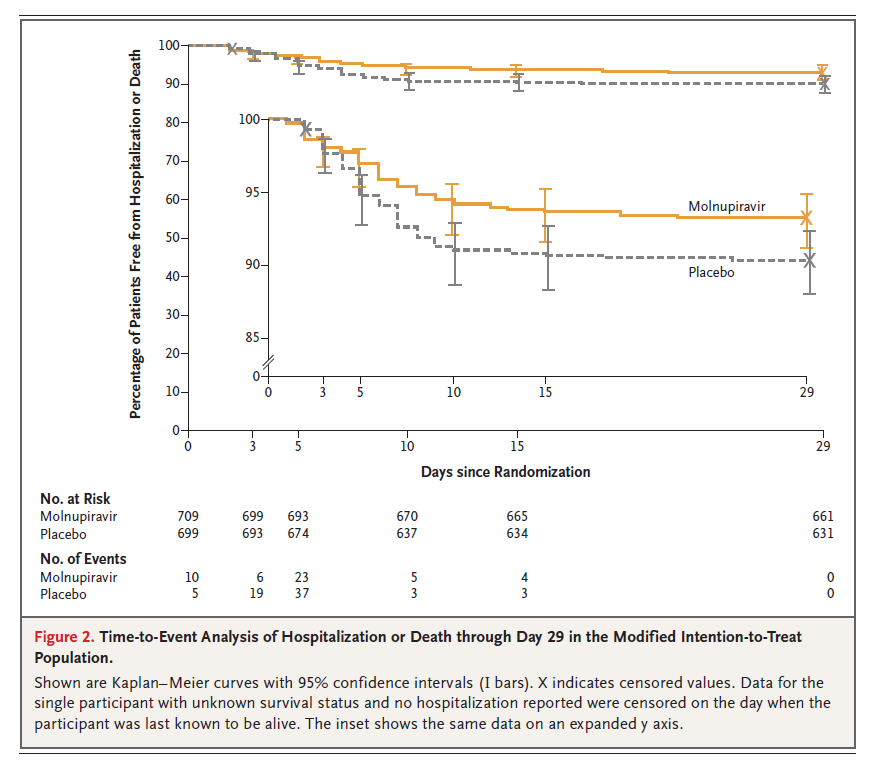
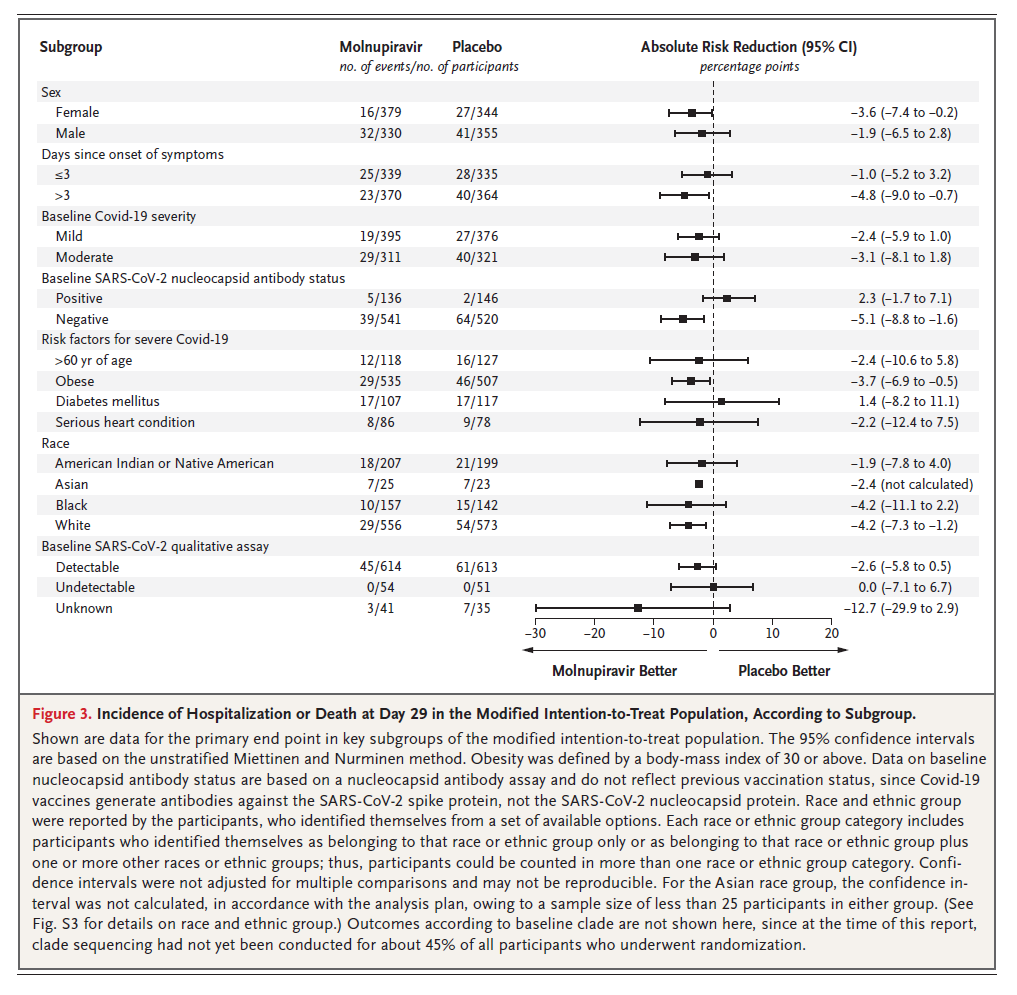
The MOVe-OUT trial was a phase-3, double-blind, placebo controlled RCT that enrolled unvaccinated adult outpatients with at least 1 risk factor for severe disease, presenting within 5 days of symptom onset with mild to moderate COVID-19. (Bernal 2021) They were randomized to 800 mg PO BID of mulnupiravir or placebo. The trial was stopped early at 50% of their target enrollment. The primary outcome was hospitalization or death at 29 days, and was decreased with mulnupiravir (6.8% vs 9.7%, 95% CI -5.9 to -0.1%). This result has a fragility index of 2. (The numbers are somewhat confusing, as they stopped the trial early but still enrolled another 700 patients after stopping the trial. I present the numbers from the full data set, rather than those used in the press releases.) There were more women randomized to mulnupiravir than placebo, and when that difference was adjusted for the benefit was not statistically significant. There was 1 death in the mulnupiravir group and 9 with placebo. Patients with evidence of previous COVID infection based on antibody testing actually look like they might have worse outcomes, which is bad news if we are trying to extrapolate these results to vaccinated patients. Adverse events look about the same in both groups.
I have seen it reported in a number of lay press outlets that two RCTs of molnupiravir in India were stopped for ‘no benefit’, but I have not seen these trials discussed anywhere in the scientific literature, and don’t see them in the usual trial registries I search. There are press releases about another Indian trial being positive, but it hasn’t been published anywhere yet. There are a few other ongoing RCTs listed on clinicaltrials.gov.
Comments
This will probably be a comment in every single post in this series, but results in unvaccinated patients probably don’t translate well to vaccinated patients. At very least, the benefits will be significantly smaller in vaccinated patients, but side effects should remain unchanged.
It is sometimes difficult to determine how the results of studies that look at hospitalization will apply to one’s own patients. Criteria for hospitalization vary drastically around the world. I frequently hear my American colleagues talking about admitting patients that I would have never even considered for an ED observation period. Therefore, in any given hospital, the hospitalization rate could be a lot less (in which case the results would be less impressive) or a lot more (in which case the benefit might be more impressive).
There is a lot of talk about molnupiravir’s mechanism of action and the potential for societal harm. It inserts itself into the virus’s RNA, causing errors that prevent viral replication. However, some people are worried that intentionally causing mutations is a bad thing and may lead to new variants. (Kozlov 2021) Considering how often mutations occur naturally, and the fact that viruses can’t mutate if you kill them, I would guess that this is not a significant risk, but I honestly have no idea. (People I consider much smarter than me seem to think this risk is real.)
Considering that this needs to be given within 5 days of symptom onset, health systems are going to have to invest in infrastructure to make this work. (Right now, we aren’t even testing most patients for COVID in Ontario.) It would be completely inappropriate to use emergency departments as the primary location for patients to access this medication, but given the track record of most healthcare systems, I worry that this is exactly what will end up happening.
The fact that other studies have been completed but not published leaves us with a significant risk of publication bias.
Bottom line
The evidence for molnupiravir is better than most other COVID-19 therapies (which is a poor standard). The benefit is small, but potentially important during a pandemic. That being said, it is still just a single study with borderline results, so we are nowhere close to 100% certainty that this medication actually works. Replication is always important. The overall clinical utility will be limited, being applicable only to high risk unvaccinated outpatients who can get tested and treated within 5 days of symptom onset.
Other FOAMed
Other First10EM COVID therapeutics updates can be found here
Ontario Science Table Recommendations
References
Jayk Bernal A, Gomes da Silva MM, Musungaie DB, Kovalchuk E, Gonzalez A, Delos Reyes V, Martín-Quirós A, Caraco Y, Williams-Diaz A, Brown ML, Du J, Pedley A, Assaid C, Strizki J, Grobler JA, Shamsuddin HH, Tipping R, Wan H, Paschke A, Butterton JR, Johnson MG, De Anda C; MOVe-OUT Study Group. Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients. N Engl J Med. 2021 Dec 16:NEJMoa2116044. doi: 10.1056/NEJMoa2116044. Epub ahead of print. PMID: 34914868 NCT04575597
Kozlov M. Merck’s COVID pill loses its lustre: what that means for the pandemic. Nature. 2021 Dec 13. doi: 10.1038/d41586-021-03667-0. Epub ahead of print. PMID: 34903873
Photo by Annie Spratt on Unsplash



{kind=link}
One thought on “COVID therapy evidence updates: molnupiravir”