
Morgenstern, J. Research Roundup (March 2022), First10EM, March 21, 2022. Available at:
https://doi.org/10.51684/FIRS.125952
Normal saline: The world’s worst murder weapon?
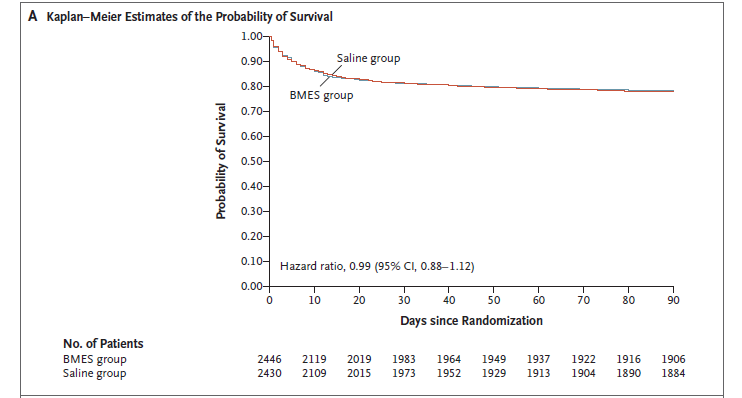
Finfer S, Micallef S, Hammond N, Navarra L, Bellomo R, Billot L, Delaney A, Gallagher M, Gattas D, Li Q, Mackle D, Mysore J, Saxena M, Taylor C, Young P, Myburgh J; PLUS Study Investigators and the Australian and New Zealand Intensive Care Society Clinical Trials Group. Balanced Multielectrolyte Solution versus Saline in Critically Ill Adults. N Engl J Med. 2022 Jan 18. doi: 10.1056/NEJMoa2114464. Epub ahead of print. PMID: 35041780
I have covered the debate about normal saline many times before, so this paper probably doesn’t require a lengthy summary. It is a multicenter double blind RCT that compared normal saline to Plama-Lyte 148 in 5037 adult ICU patients. Very predictably, there were no differences at all. The primary outcome was mortality, and was identical (21.8% vs 22.0%, p=0.90), as were the other clinical outcomes. Although there are some limitations to this trial (which you can read about in the full blog post), the results are entirely consistent with the existing data on the topic. A reasonable amount of saline in the average patient is just not increasing mortality. If you want to use something else, go for it, but this decision almost certainly doesn’t matter.
Bottom line: The well done RCT demonstrates no difference in mortality when using normal saline as compared to Plasma-Lyte 148 in adult ICU patients.
Hammond NE, Zampieri FG, Di Tanna GL, et al. Balanced Crystalloids versus Saline in Critically Ill Adults — A Systematic Review with Meta-Analysis. NEJM Evidence. 2022; 1(2).
This is a systematic review and meta-analysis published at the same time as the PLUS study. Despite including some lower quality studies, it confirms the above message: there is no difference between normal saline and balanced fluids as they are being used in these studies.
Toxicology: Why is there so much that I have never heard of?
Jang DH, Hoffman RS, Nelson LS. Attempted suicide, by mail order: Abrus precatorius. J Med Toxicol. 2010 Dec;6(4):427-30. doi: 10.1007/s13181-010-0099-1. PMID: 20563676
I love toxicologists, but they also tend to make me feel inadequate almost every time they say something. There are just so many things that I feel I should know as an emergency physician, but actually know nothing about. For example, have you ever seen a bracelet that looks like this?

I have, many times, but I had absolutely no idea that it is made up of seeds (the jequirity pea or arbus seeds) that are toxic, and in children a single seed can be deadly. I first came across this in a twitter thread describing a 3 year old girl presenting to the emergency department with vomiting and diarrhea, which was actually the result of her chewing on one of these bracelets. I am almost certain I would have misdiagnosed this presentation as gastroenteritis. This article was part of some follow-up reading, and is a case report of a young man who also presented to the emergency department with vomiting and diarrhea, but the final diagnosis was a suicide attempt using these seeds, which he was able to buy online. I had never heard of abrin before. It is related to ricin, with almost identical effects, except that abrin is about 75 times more toxic than ricin (which is already well known for its toxicity). Seems like a good choice for jewelry to me. Presentation will be nonspecific, with nausea and vomiting, but will eventually develop into convulsions, liver failure, and death. Treatment is only supportive. So, how comfortable are you with that patient that you sent home yesterday with the diagnosis of gastro?
Bottom line: OK, I will probably still never make this diagnosis in my life, but I think it is important for us to keep in mind how easy it is to get toxic substances off the internet. Toxicology should always be on the differential diagnosis, and I know toxicologists love chatting about abrin toxicity at 4am.
No, pain is not a ‘vital sign’
Davis S, Ju C, Marchandise P, Diagne M, Grant L. Impact of Pain Assessment on Canadian Triage and Acuity Scale Prediction of Patient Outcomes. Ann Emerg Med. 2022 Feb 17:S0196-0644(22)00014-2. doi: 10.1016/j.annemergmed.2022.01.014. Epub ahead of print. PMID: 35184870
This is a retrospective cohort that compared the standard Canadian Triage Acuity Scale (CTAS) score from 229,774 patients to one that dropped the inclusion of the pain score. (About 60% of the cohort reported pain, and therefore had a pain score included as part of their triage score.) There was actually a very slight negative correlation between pain scores and clinical outcomes, such that patients reporting higher pain scores were less likely to be admitted to hospital, admitted to ICU, or die (although numbers are essentially identical in both groups). The conclusion of the study is that, “the removal of the pain scale from CTAS did not reduce its ability to predict hospital admission, ICU consultation, or the 72-hour mortality.” I imagine anyone working clinically could have predicted this, as we have seen the wide variety of patients presenting with 11/10 pain. I actually think that the discussion about pain scores is complex. Obviously, the ‘pain is a vital sign’ campaign was an awful, biased, industry funded campaign to sell drugs which ultimately killed a lot of people. It should serve as a major warning against industry involvement in medicine, but for some reason many physicians are still willing to act as if pharmaceutical companies have patient interests and not just profits in mind. Conversely, “pain out of proportion” is routinely listed as a feature of some of our most feared diagnoses. That would indicate pain, and the reaction to it, is an important clinical data point. However, those conditions are rare enough that the effect would be easily washed out in a cohort of over 200,000 patients. On the other hand, the lack of signal reminds us of the complete lack of specificity of the pain score, because otherwise ‘pain out of proportion’ could be an indication for imaging every single shift. Furthermore, although our primary goal in emergency medicine is identification and remedying of life threats, we really are in the business of alleviating suffering. Therefore, if all else is equal, it probably makes sense for me to see the patient in 10/10 pain, even if other patients might have been waiting longer. Triage is not a simple process, and there will never be a single attribute that can be used to perfectly categorize patients. I believe triage nurses have the most difficult job in the entire hospital, and anything we can do to reduce their workload, such as decreasing the number of mandatory questions they have to ask, is a great addition in my eyes. My guess is that the best approach is to remove the pain score from the mandatory list of questions triage nurses ask, but encourage them to communicate it to us as part of their clinical assessment as they see fit.
Bottom line: The pain score does not seem to add any predictive value to the Canadian triage score.
If a tree falls in the forest, or if an MI causes no bad outcomes
O’Fee K, Deych E, Ciani O, Brown DL. Assessment of Nonfatal Myocardial Infarction as a Surrogate for All-Cause and Cardiovascular Mortality in Treatment or Prevention of Coronary Artery Disease: A Meta-analysis of Randomized Clinical Trials. JAMA Intern Med. 2021 Dec 1;181(12):1575-1587. doi: 10.1001/jamainternmed.2021.5726. PMID: 34694318
This is a slightly esoteric topic that may not seem to have immediate clinical consequences. However, I think it is an important concept to understand in medicine. Many of our diseases are defined in such a way that they don’t mean what they think they mean. This article is about non-fatal MI. I have talked about this concept at length, such as in my articles about heparin and the series on stress testing. In general, we worry about MIs because we worry that patients might die. When you remove mortality from the equation, and define something as “non fatal MI”, it becomes a lot less clear exactly what it means. Really, it just means that the patient had a rise and fall in their troponin. It is no more important than a lab value, but calling it an “MI” makes it sound incredibly important, and so we feel compelled to do something about it. (The same probably happens in many disease states, such as subsegmental PEs or pneumothoraces only visible on CT.) This is a meta-analysis that looks at RCTs that included at least 1000 patients and had at least 24 months of follow-up. They end up with a massive sample of over 1 million patients, and it turns out that non-fatal MI is not associated with all cause or cardiovascular specific mortality. It also wasn’t associated with future revascularization. In other words, it is not a good surrogate outcome. Personally, this interests me because of its research implications for heparin and stress testing, where often the only claimed benefit is a decrease in ‘non fatal MI’. However, I think there are wider clinical implications that need to be considered. When you are counseling patients about their “MI” because of a rise in troponin, do you know what the true implications of this diagnosis are? (Of course, we don’t know at the time that the patient fits into the ‘nonfatal’ category, which makes this all the more complicated.)
Bottom line: “Nonfatal MI” may not have the clinical implications that you thought it did.
The best bad news
Trueger NS. The Best Bad News. JAMA Neurol. 2022; doi:10.1001/jamaneurol.2021.5113
I don’t have a lot to say about this article, aside from suggesting you read it. The article begins: “ “I’m sorry to have to tell you this,” said the man on the phone, “but they found cancer.” “That’s the best news I’ve heard in a year,” I replied.” It is an article written by a fellow emergency doctor, and a friend from the Twitter and FOAMed worlds, about his journey through a rare and disabling diagnosis. Seth is a great writer, and I think this article provides every clinician with lots to reflect upon.
Don’t prescribe tramadol. Seriously.
Xie J, Strauss VY, Martinez-Laguna D, Carbonell-Abella C, Diez-Perez A, Nogues X, Collins GS, Khalid S, Delmestri A, Turkiewicz A, Englund M, Tadrous M, Reyes C, Prieto-Alhambra D. Association of Tramadol vs Codeine Prescription Dispensation With Mortality and Other Adverse Clinical Outcomes. JAMA. 2021 Oct 19;326(15):1504-1515. doi: 10.1001/jama.2021.15255. PMID: 34665205
The appropriate approach to tramadol prescribing is very clear: just don’t do it. For my Canadian audience, where tramadol use is essentially unheard of, this paper won’t be of much value. However, in other places in the world, tramadol is still handed out like candy, so there is probably some value in keeping up with the literature. This is a very large, propensity-matched database study out of Spain. They included adult patients with at least 1 year of follow-up data available, and a prescription for either tramadol or codeine. (Perhaps the biggest limitation of this study is that the comparison is codeine, another opioid that there is just no logical reason to use.) As compared to codeine, tramadol prescriptions were associated with a higher risk of all cause mortality (13.00 vs 5.61 per 1000 person-years; HR, 2.31 95%CI 2.08-2.56). Despite the fact that the active metabolites of tramadol directly bind to opioid receptors, some people still refer to it by the physiologically nonsensical name of a “weak opioid”. In terms of opioid abuse and dependence, tramadol was statistically the same as codeine, although it looks like it could be worse (hazard ratio 1.91, 95% CI 0.72-5.08). Of course, codeine is not the comparison we really want to see, as some people also consider it a ‘weak opioid’. The comparison we would really want to see is to morphine, but that will have to wait for another paper. There was already absolutely no reason to prescribe tramadol, and this paper demonstrating an association with increased all cause mortality doesn’t help.
Bottom line: Don’t prescribe tramadol.
Emergency medicine: is less more?
Atkinson P, McGeorge K, Innes G. Saving emergency medicine: is less more? CJEM. 2022 Jan;24(1):9-11. doi: 10.1007/s43678-021-00237-1. Epub 2022 Jan 17. PMID: 35038157
This is an article that many readers will have read already, as it is one of the most widely shared emergency medicine articles I have ever encountered. Unfortunately, it says things that every emergency physician already knows. Patients don’t choose to come to the emergency department. They come because we are frequently the only location they can receive care in a timely manner. (Or they come because they are told to, as we are the default location for every specialty to send their patients to receive care after hours when they are at home.) Demand for emergency care has risen dramatically over my career, and this paper cites a report that anticipates ED visits will grow by 40% more over the next 20 years in Canada. However, the demand placed on emergency departments is generally generated outside of our walls: poor access to primary care, unmanaged chronic disease, poorly staffed long term care, and lack of hospital beds for admitted patients. These are all factors outside of our immediate control. The emergency department stands as the safety net for a broken health system, but then people look at our wait times, and our overcrowding, and think that the emergency department needs fixing. In fact, in large part, we are a victim of our own success. We are overrun with patients precisely because we have proven we are more than capable of caring for them. No matter what your problem, we will look after you in the emergency department, and we will do a damn good job of it. These authors argue it is time to fix the culture of medicine that sees the emergency department as a catch-all dumping ground. “The ED is the wrong place for most patients.” They argue we need to clarify the primary mission of emergency departments. They argue that patients deserve the right care from the right providers. That means that primary care should be delivered by primary care physicians and post-operative care should be delivered by surgeons. Unfortunately, in order for this to change, patients need timely access to these services. Change won’t be easy, and I imagine there will be some debate about this article, but I think it is a must-read for everyone in our field (and hopefully many outside as well).
Bottom line: This is one of the most important emergency medicine papers of the decade. Unfortunately, we aren’t the ones who need to read it. We need hospital administrators and leaders in other specialties to read these words, because it is the system outside of the emergency department that is broken, and although we take pride in propping the entire system up, cracks are starting to show.
Rate control showdown
Jafri SH, Xu J, Warsi I, Cerecedo-Lopez CD. Diltiazem versus metoprolol for the management of atrial fibrillation: A systematic review and meta-analysis. Am J Emerg Med. 2021 Oct;48:323-327. doi: 10.1016/j.ajem.2021.06.053. Epub 2021 Jun 30. PMID: 34274577
We have covered the beta-blocker versus calcium channel blocker in atrial fibrillation debate many times in the summaries, and there has always been a clear winner. Just as a bit of spaced repetition, or for those new to the summaries, this is a systematic review and meta-analysis that looked for RCTs comparing diltiazem to metoprolol for the management of afib. They only include 3 RCTs with a grand total of 150 patients, which may be explained by their decision to limit their search to just diltiazem and metoprolol rather than all beta-blockers and calcium channel blockers. Either way, the results fit exactly with what we know. Diltiazem is significantly better at achieving rate control in the emergency department (HR 2.05, 95% CI 1.4-3). No differences were noted in their primary safety outcome of blood pressure at 15 minutes. Obviously, there are some very significant limitations to a meta-analysis that only included 150 patients. Considering how common this presentation is, it is somewhat surprising the data isn’t better. There may be reasons other than rate control to choose a beta-blocker, as they are indicated for the long term management of CAD and CHF, which many of these patients will have. However, if you want to have a chance to discharge the patient from the emergency department, diltiazem is the clear choice. (In fact, the only reason that I would choose metoprolol is if I wanted the patient to be admitted, because metoprolol essentially always results in a failure of rate control and a necessary admission). Although I am fairly certain diltiazem is the superior agent in terms of success of rate control, the fact that this systematic review is so small is a good reminder of the paucity of data, and the fact that even our most fervent beliefs are susceptible to newer and better science.
Bottom line: In terms of rate control in the ED, calcium channel blockers are probably better than beta-blockers. However, speed of rate control may not be the most important thing to your patient, and if they are going to be on a beta-blocker long term anyway, it might be worth starting with one, even if it means a higher chance of needing a hospital admission.
Did you know misinformation was a problem during COVID?
Parker L, Byrne JA, Goldwater M, Enfield N. Misinformation: an empirical study with scientists and communicators during the COVID-19 pandemic. BMJ Open Sci. 2021 Nov 25;5(1):e100188. doi: 10.1136/bmjos-2021-100188. PMID: 35047703
There are so many different articles that I could have chosen that discuss the problem of misinformation during COVID. I probably have a soft spot for this one, as it takes an empirical ethics approach using qualitative methodology, which is exactly what I focused on for my master’s degree. I may also like it because the researchers interviewed identified a list of issues that I have been ranting about for years (most of which can be found in my EBM bibliography). One issue with misinformation during the pandemic has simply been bad science, with a proliferation of fraud and low quality highly biased studies. These researchers discuss some reasons for poor science, including the pressure to publish, commercial influences, and poor research practices (such as p-hacking). The second theme that they felt increased misinformation was inadequate access to science, including publication bias, paywalls, an inefficient or broken peer review system, and poorly written (jargony) academic manuscripts. Finally, they identify the problem of poor science literacy, which clearly extends well into trained professionals such as physicians. If you are interested in this topic, their table 3 going over suggested solutions is pretty reasonable, and addresses many of the topics I have discussed and will continue to discuss about science in general.
Bottom line: We need to completely overhaul the way science works and is discussed in medicine.
On that topic: Yes, masks work
Andrejko KL, Pry JM, Myers JF, et al. Effectiveness of Face Mask or Respirator Use in Indoor Public Settings for Prevention of SARS-CoV-2 Infection — California, February–December 2021. MMWR Morb Mortal Wkly Rep. ePub: 4 February 2022. DOI: http://dx.doi.org/10.15585/mmwr.mm7106e1
This is a low quality COVID study, which is somewhat ironic considering the last paper. However, sometimes observational data can be valuable, as long as you are cautious in your interpretations, and fit the data in with everything else we know on a topic. At very least, you will see this paper referenced everywhere, and should probably know what it really says. This is a case control study, which matched patients in California who had positive molecular COVID tests to patients with negative tests. They called patients for an interview within 48 hours, and a major limitation is that the interviewer was not blinded to the test status of the patient. (This seems like a pretty big mistake, as it doesn’t seem like it would have been too hard to do this study blinded). They enrolled about 1600 patients, which is only about 10% of those they tried calling. The interviews focused on exposures and mask wearing. Recall bias, response bias, expectation bias, and many other forms of bias can easily find their way into these retrospective interviews. About 5% of patients reported never wearing a face mask, while 60-70% reported always wearing a face mask in indoor settings. Always using a face mask was associated with a significantly lower chance of having COVID (adjusted OR 0.44 95% CI 0.24-0.82). As might be expected, cloth masks were worse than surgical masks, which were worse than respirators (KN95s or N95s). Obviously, there are a lot of limitations to this data. I can imagine a million possible confounders. People who wear N95s are probably more cautious in all their activities. People who wear N95s are probably more scientifically literate, and more up to date on the realities of COVID. That being said, we know that COVID is an airborne disease, and we have pretty good data that suggests N95s are better than surgical masks. This data would never stand alone, but it is a reasonable real world demonstration of the science we already have.
It is so very very depressing that shortly after I wrote this summary, many jurisdictions in the world decided to declare COVID over and drop all precautions, including mask mandates. COVID has provided a never ending insight into the stupidity of our leaders, and I am somewhat sick of it.
Bottom line: Despite the major weaknesses in this data, the results are probably true. As long as community levels of COVID are high, masks should be worn at all times when in indoor public spaces, and respirators are almost certainly the best choice (although cost considerations are not considered in that). Personally, I wear an N95 at all times when I am indoors in public.

Cheesy Joke of Month
What prize do you give someone who hasn’t moved a muscle in over a year?
A trophy



4 thoughts on “Research Roundup (March 2022)”
Wait, in Canada you send patients you start on Cardizem for afib with RvR home? What do you do, transition them to oral meds in the ED??? This blows my mind. Standard practice in the US (at least everywhere I’ve worked) is to start on a Cardizem drip and admit to the cardiac progressive/step-down unit. They’ll go home in a few days once they’ve been transitioned to oral meds and cardiology is satisfied with their medication regime. The only time I have ever sent someone with afib with RvR home from the ED is if I’ve electrically cardioverted them, they’ve maintained a sinus rhythm, they’re otherwise healthy, and I’ve talked with their cardiologist and started them on anticoagulation if they aren’t on it already. That’s like……. maybe 5% of afib with RvR patients.
I still mostly cardiovert – but even when rate controlling, the goal is discharge. No benefit of drips over bolus. I just bolus diltiazem 10-15mg once or twice, and if that is working given them an oral dose right away, with the plan to discharge them on oral plus or minus anticoagulation. (But, to be fair, given than I almost always cardiovert, this doesn’t happen all that often, as patients required rate control have sort of self selected as more complex and potentially needing admission.)
In residency, I worked with a lot of people who would give an oral dose of diltiazem, send the patient home to sleep with the HR still in the 140s, and have them come back to the ED in the morning for a recheck. 30-40% were in sinus on that recheck, and the vast majority of the rest were rate controlled. I never adopted this practice, but it seemed pretty effective.
I struggle to understand why suddenly the results of a very low quality study are “probably true”…I think we should be very careful in scientific speech, and, in my opinion, the word “probably” doesn’t reflect a truthful conclusion…
Anyway, I love all your critical appraisal and philosophical thinking. I just think that in this particular topic you were a bit biased (as we all are for some topics), and it’s all even more evident in this sequence, after the previous study.
I hope you don’t see this comment as an offense, just as an opportunity to openly discuss a scientific question!
Peace,
Bernardo
Thanks Berndardo… I think you are referring to the comments on the Afib? I say probably true not based on this very weak data, but based on the numerous other studies covered over the last 10 years (and that I am pretty sure I heard from decades before that on EMA). Without having done a systematic review myself, my sense is that every study ever done shows the same thing: faster HR reduction with calcium channel blockers. The consistency, even in lower quality studies, leads my to say “probably” – but it certainly could be a biased remembering of the prior literature.