
Morgenstern, J. The ongoing saga of normal saline versus balanced fluids, First10EM, January 31, 2022. Available at:
https://doi.org/10.51684/FIRS.124985
I have discussed the ongoing battle between normal saline and ‘balanced fluids’ many times in the past. First, there was the SPLIT trial, a double blind cluster RCT of 2200 ICU patients that showed no difference between saline and Plasma-Lyte 148. (Young 2015) Next, we had the SMART trial, an unblinded cluster RCT of 15,000 ICU patients, which showed a difference in their composite outcome of major adverse kidney events, but had numerous issues (and a fragility index of 0). (Semler 2018) The SALT-ED trial was performed simultaneously, and was an unblinded cluster RCT of 20,000 emergency department patients, and showed no difference in their primary outcome of hospital free days. (Self 2018) Finally, we covered the BaSICS trial, a double blind RCT of 11,000 ICU patients that showed no difference in mortality between normal saline and Plasma Lyte 148. (Zampieri 2021) I imagine most people are pretty bored with this topic, but there are still some people with very strong opinions. It is not uncommon to hear people claim that saline is killing patients, despite strong evidence to the contrary. So I guess we had better cover the 2 new publications in the New England Journal of Medicine: the PLUS trial and accompanying systematic review and meta-analysis.
The PLUS trial
Finfer S, Micallef S, Hammond N, Navarra L, Bellomo R, Billot L, Delaney A, Gallagher M, Gattas D, Li Q, Mackle D, Mysore J, Saxena M, Taylor C, Young P, Myburgh J; PLUS Study Investigators and the Australian and New Zealand Intensive Care Society Clinical Trials Group. Balanced Multielectrolyte Solution versus Saline in Critically Ill Adults. N Engl J Med. 2022 Jan 18. doi: 10.1056/NEJMoa2114464. Epub ahead of print. PMID: 35041780
The Methods
This was a multicenter double-blind RCT.
Patients
Adult ICU patients who were expected to need at least a 3 day ICU stay, in whom the treating physician believed fluid resuscitation was necessary, and also believe that saline and balanced fluids were equally appropriate.
Exclusions: patients with specific fluid requirements, who had “received disqualifying fluid resuscitation”, were at imminent risk of death, had a life expectancy less than 90 days, had traumatic brain injury, or were at risk for cerebral edema.
Intervention
Plasma-Lyte 148.
Comparison
Normal saline.
In both groups, fluids were provided in identical 1 L bags, and the same blinded fluid was used for all fluid requirements for 90 days after randomization.
Outcome
The primary outcome was death from any cause within 90 days of randomization.
The Results
They enrolled a total of 5037 patients. (The trial was originally designed to include 8800 patients based on their power calculation. Enrollment was stopped early, without looking at the data, because of the COVID pandemic.) The mean age was 62, 39% were female, 45% were admitted from the operating room, and 79% were receiving mechanical ventilation. The median volume of study fluid was just under 4 L over an average of about 6 days. There was significant crossover, with 63% of the Plasma-Lyte group receiving more than 500 mL of normal saline, but almost none of the saline group receiving Plasma-Lyte.
There was no difference in the primary outcome of all cause mortality (21.8% vs 22.0%, p=0.90).
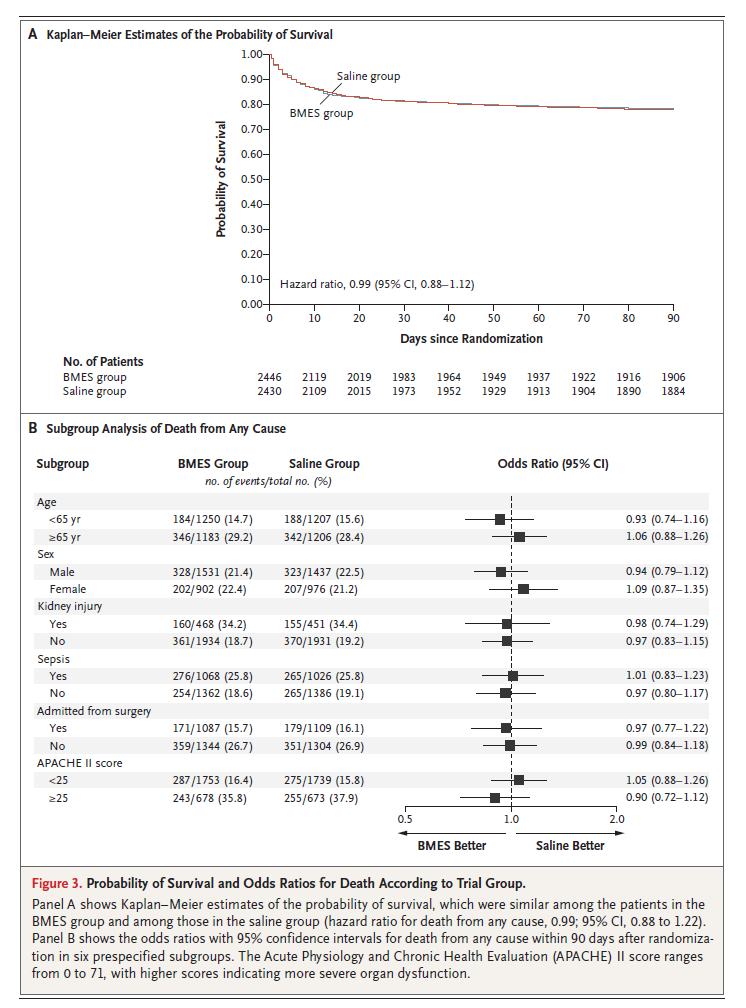
Normal saline had statistically but not clinically significant differences in pH (mean difference 0.01) and chloride (mean difference 2), but no difference in creatinine. Renal replacement therapy was also unchanged.

My thoughts
It always bothers me when trials allow clinicians to exclude patients because they think one of the treatments is better, when the whole point of the trial is clearing up existing equipoise. It creates a significant dilemma in extrapolation of the results, because a key subgroup of patients may have been excluded, but it is very difficult to identify. Maybe these clinicians were very good at identifying the patients that needed balanced fluids, and excluded them all from the trial. If so, will I be able to identify those same patients? What criteria were used? They don’t include a standard flow diagram in the publication, so I can’t tell how many patients were excluded for this reason.
There was also significant crossover between the groups. This is necessary in an ICU setting, as many of the medications being used are only compatible with normal saline. (Or at least, there is only data confirming compatibility for normal saline). If you were a true believer in balanced fluids, this use of normal saline could wash out a real difference. However, I personally doubt that small values of normal saline can do any harm. More importantly, this saline will be given to all your patients, so if it is enough to eliminate any value from balanced fluids, then there is no value in using balanced fluids.
Of course, the big question when looking at these studies is always: why should we consider normal saline as the standard? If you were already using a balanced fluid, there is absolutely northing in these trials that would convince you to switch to saline. However, Plasma-Lyte is significantly more expensive, and I think this data makes it very clear that the added expense is not worth it. From a resuscitation standpoint, I continue to use saline because drug compatibility issues can cause issues with the timeliness of interventions. For example, drugs that are listed in various sources as incompatible with Ringer’s lactate include: ceftriaxone, ciprofloxacin, diazepam, ketamine, lorazepam, nitroglycerin, phenytoin, and propofol. Because Ringer’s also contains calcium, blood products are also contraindicated. Although I imagine a lot of these contra-indications are myths, they lead to real world problems. I have been in multiple resuscitations where important medications were delayed because nurses were trying to sort out compatibility issues.
The second paper
Hammond NE, Zampieri FG, Di Tanna GL, et al. Balanced Crystalloids versus Saline in Critically Ill Adults — A Systematic Review with Meta-Analysis. NEJM Evidence. 2022; 1(2).
This is a systematic review and meta-analysis performed by the PLUS team to incorporate their data with the existing literature. They include 6 trials (encompassing 34,450 patient) that they count as having “a low risk of bias in all domains”. There are some big name researchers on this meta-analysis, but I have absolutely no idea how they decided that these trials were at a “low risk of bias”. They include both the SMART and SALT-ED trials, which were unblinded and not truly randomized. Both trials are at high risk of bias based on their design, and because of their size, weigh heavily on this analysis. Despite that, there is still no statistical difference between normal saline and balanced IV fluids for the primary outcome of mortality (RR0.93, 95% CI 0.76-1.15). They don’t include a funnel plot, but to my eyes the studies follow a very classic pattern where smaller and more biased trials show an effect, while larger and higher quality studies are clearly negative. This hints at possible publication bias. The two highest quality studies are the BASICS trial (with a RR of 0.97) and the PLUS trial (with a RR of 0.99), which clearly show no benefit.

There was also no difference in acute kidney injury (RR 0.96 95% CI 0.89-1.02) or renal replacement therapy (RR 0.95 95% CI 0.81-1.11). There were no differences in any of their secondary analyses or subgroups.
As I said, this data includes 2 trials I would consider to be at high risk of bias, and still finds no benefit despite including almost 35,000 patients. That sounds like a pretty definitive nail in this coffin to me.
I will note, Paul Young, who is an author on a number of these papers and one of the best critical care researchers in the world, has a different interpretation than I do. He looks at the PLUS numbers and the resultant meta-analysis, and says that “overall, it appears likely that balanced crystalloids reduce mortality overall and for ICU fluid therapy they should be the fluids of choice.” He bases this interpretation on the 95% confidence intervals that primarily lie on the side of harm. Although I agree that we shouldn’t be strictly dichotomous about trials (labeling them as positive or negative), I am concerned about including SMART and SALT-ED in the numerical estimate. Furthermore, all trials contain a variety of biases, and random chance means it is very unlikely to see a relative risk of 1 even when comparing identical therapies. With 35,000 patients in these studies, I think this data is most consistent with no difference at all (although I will admit that I cannot exclude a very small harm – or even a very small benefit – within those confidence intervals).
Bottom line
As we probably should have predicted, it is very unlikely that normal saline is killing patients. It is very unlikely that normal saline is damaging kidneys. The best available evidence suggests that any crystalloid fluid is reasonable. Normal saline remains my fluid of choice in most situations as balanced fluids have more medication incompatibilities that can complicate resuscitation and delay important therapies, but honestly I don’t think this choice matters too much at all.
If you want to make a difference on patient outcomes with your choice of IV fluids, I think the key is probably to give less of whatever you choose.
Other FOAMed
References
Finfer S, Micallef S, Hammond N, Navarra L, Bellomo R, Billot L, Delaney A, Gallagher M, Gattas D, Li Q, Mackle D, Mysore J, Saxena M, Taylor C, Young P, Myburgh J; PLUS Study Investigators and the Australian and New Zealand Intensive Care Society Clinical Trials Group. Balanced Multielectrolyte Solution versus Saline in Critically Ill Adults. N Engl J Med. 2022 Jan 18. doi: 10.1056/NEJMoa2114464. Epub ahead of print. PMID: 35041780
Hammond NE, Zampieri FG, Di Tanna GL, et al. Balanced Crystalloids versus Saline in Critically Ill Adults — A Systematic Review with Meta-Analysis NEJM Evidence. 2022; 1(2).
Self WH, Semler MW, Wanderer JP, et al. Balanced Crystalloids versus Saline in Noncritically Ill Adults. The New England journal of medicine. 2018; 378(9):819-828. PMID: 29485926 [free full text]
Semler MW, Self WH, Wanderer JP, et al. Balanced Crystalloids versus Saline in Critically Ill Adults. The New England journal of medicine. 2018; 378(9):829-839. PMID: 29485925 [free full text]
Young P, Bailey M, Beasley R, et al. Effect of a Buffered Crystalloid Solution vs Saline on Acute Kidney Injury Among Patients in the Intensive Care Unit: The SPLIT Randomized Clinical Trial. JAMA. 2015; 314(16):1701-10. PMID: 26444692
Zampieri FG, Machado FR, et al. Effect of Intravenous Fluid Treatment With a Balanced Solution vs 0.9% Saline Solution on Mortality in Critically Ill Patients: The BaSICS Randomized Clinical Trial. JAMA. 2021 Aug 10. doi: 10.1001/jama.2021.11684. PMID: 34375394 [free full text]
Photo by Maxime Gilbert on Unsplash


6 thoughts on “The ongoing saga of normal saline versus balanced fluids”
Possible you have the forest plot from the new NEJM Evidence SRMA study posted here, and not the one from the 2020 Ann Pharm study? Also your CI on mortality from that review seems off. Only extends to 1.01 in your forest plot, and 1.02 in the papers forest plot, in ylur text it’s much wider. Either way brilliant analysis as always. Now just have to figure out how to handle the Bayesian analysis silliness.
Weird – definitely was using the NEJM – not sure where that citation came from (I obviously do some copying and pasting)
The confidence interval I cite is the for the overall analysis – at the bottom of the figure. In their text, they focus on just the upper analysis of trials they consider to have low bias. However, their definition of low bias includes unblinded cluster randomized trials, which seems incorrect to me, so I would look at all the data, not just the subset they focus on.
Great point about bias assessment. I ignored the lower forest plot section, stupidly.
Something weird, though. Total of 440 subjects in that lower section (34/217 vs 40/213 deaths, almost identical at 16 vs 18%). Then, up top there’s >34,000 subjects. Maybe it’s a matter of variance from those lower studies, pulling things apart. But one wouldn’t think 400 subjects (1% of the total calculation), with no difference between groups, could possibly alter the CI so dramatically.
Anyway, one more genius post, very well done. And yes, PLEASE, let’s not allow ‘Bayesian’ verbiage to turn a p-value of 0.49 into an intervention that ‘likely reduces mortality’. That is where Paul Young’s comments are headed.
p.s. also note if Young was correct, and we accepted the premise 0.96 is an accurate RR and these numbers represent ‘the average benefit’ as the authors say, that average benefit would be roughly 0.07-0.08%, NNT of about 1400.
I think your analysis is reasonable. Although an argument can be made that the majority of these trials include ICU patients in whom the bulk of the fluid resuscitation already happened before entering the trial.
I have a different question: What fluids do you use in severely hypovolemic and acidotic – NAGMA and uremic – patients?
For most patients, I really don’t think the fluid choice matters. Kidneys are great at sorting things out. The only patients I think this could make a difference in are those with kidney problems. So the uremic patient who could have significant kidney failure would make me want to use a fluid with a closer match to physiology – which in my hospital is Ringer’s Lactate. However, even in these patients, the vast majority recover kidney function with the initial fluid resuscitation, and the electrolyte balance really probably doesn’t matter. (It is diluted in a relatively large amount of interstitial fluid, so even a very abnormal fluid like saline doesn’t actually change pH, chloride, or sodium numbers much.)