
Morgenstern, J. COVID-19 is spread by aerosols (airborne): an evidence review, First10EM, November 30, 2020. Available at:
https://doi.org/10.51684/FIRS.52248
In early April, I wrote a long post covering all the science I could find about aerosols and droplets. The basic summary was that this is an area of medicine with lots of misconceptions, poor assumptions, and incomplete science. There was good evidence that previous coronaviruses were spread by aerosols. There was good evidence that influenza is spread by aerosols. Overall, it seemed very likely that SARS-CoV-2 or COVID-19 was being spread by aerosols, but the science was pretty weak. There is still a lot we don’t know, but as I update the evidence 6 months later, it is pretty clear that aerosols play an important, and unfortunately still widely ignored, role in the transmission of COVID-19.
Dispelling some misconceptions
There are still many who argue strongly against the role of aerosols in transmission of COVID-19. In general, I think these arguments clash with science and have significant logical inconsistencies. Before getting to the evidence that COVID-19 is spread by aerosols, let’s dispel a few widely held misconceptions.
COVID-19 has a low Ro
One main argument against aerosol spread points to the Ro, with the assumption that airborne diseases will always spread easily, and therefore have a high Ro. The argument is often framed as, “this disease doesn’t look like measles, and therefore cannot possibly be airborne.” This is bad logic, as infectivity and mechanism of transmission are separate concepts. Some pathogens require higher numbers to reliably cause infections, which will result in a lower Ro no matter how the infection is transmitted. “While many airborne infections are highly contagious, this is not, strictly speaking, part of the definition.” (Tellier 2019)
The logic here is clearly faulty. The argument being used has the basic format: “X is a Y. Z is not like X. Therefore Z cannot be a Y.” This is somewhat like saying “a horse is a mammal, therefore that dog cannot be a mammal because they don’t look the same.”
This logic is especially problematic in the context of aerosol spread because there are other diseases with good evidence of aerosol spread, such as influenza, that look nothing like measles, but a lot like COVID-19. In fact, the prototypical airborne pathogen is tuberculosis, and tuberculosis has an Ro between 1-3 (exactly like COVID-19). (Ma 2018)
Furthermore, the statement that ‘COVID looks nothing like measles’ is probably untrue. On average, disease transmission is low, but if you look at super-spreaders, COVID-19 starts to look a lot like measles.
Therefore, the arguments based on Ro are both illogical and inconsistent with science. If anything, the Ro of COVID-19 looks exactly like other known airborne diseases (such as tuberculosis), and so this would be an argument in favour of airborne spread.
Most transmission is short distance
The equally fallacious corollary to the Ro argument is that “if COVID-19 is transmitted through aerosols, we should see a lot of infections occurring over long distances”. Although it is true that aerosols will disperse much further than droplets, it is faulty logic to define the mode of transmission by the distance of transmission. The concentration of infectious particles falls dramatically with distance, even when those infectious particles are carried by aerosols. They are spread out through 3 dimensional space, and therefore decrease exponentially with distance. Although aerosols can transmit disease over long distances, they are much more likely to transmit disease over a short distance. (Chen 2020)
This illogical step is so ingrained in the infectious diseases literature that most studies just assume droplet spread if there was close contact. This illogical assumption undermines a great deal of the existing infectious disease literature.
As an interesting historical analogy, for decades it was thought that tuberculosis was transmitted through droplets and fomites, because it occurred most often after close contact. We now know that tuberculosis can only be transmitted through aerosols. (Jimenez 2020)
The existing science refutes the assumption that close contact suggests droplet spread. At the typical conversational distance of about 1 meter, exposure to aerosols is about 2000 times greater than exposure to droplets. (Chen 2020)
The bottom line is that short range disease transmission is definitely consistent with aerosol transmission, and distance cannot be used to define mode of transmission.

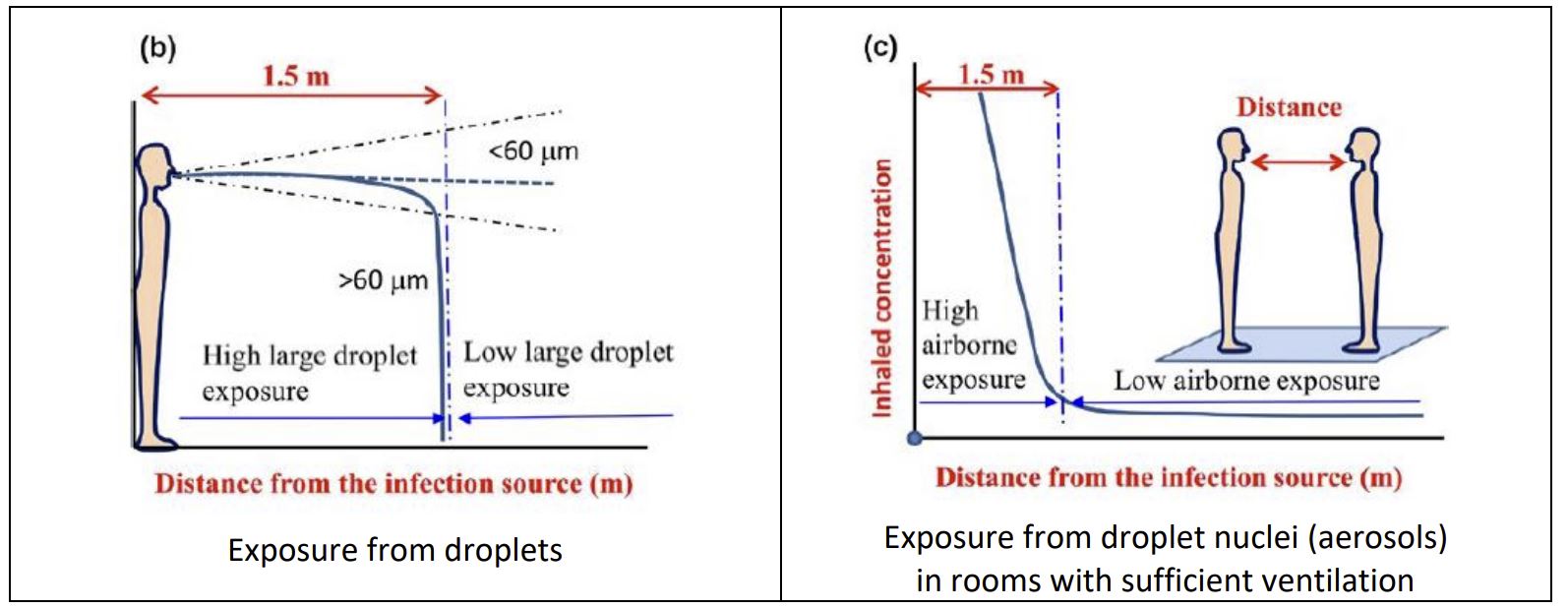
So why don’t we see a lot of long range transmission of COVID-19? The primary explanation is simple dilution. The further you are from a patient, the more dilute aerosols become. Risk of aerosol transmission drops off dramatically with increasing distance.
The importance of dilution of aerosols is evident in everyday life. You can smell cigarette smoke when you are standing 8 meters away from a smoker, but it is nothing like the obnoxious fumes present if you were standing right next to them. Similarly, cigarette smoke is much worse indoors than out. Imagine each smoke molecule as a virus. You are obviously at much higher risk 1 meter away than you are at 8 meters. (But that doesn’t make smoke a droplet.)
Dilution doesn’t prevent exposure to the virus, but it makes it less probable. With dilution of aerosols, the primary driver of infection is the intrinsic infectivity of the pathogen. If infection occurs after exposure to only a few viral particles, we should expect to see more long range transmission despite the dilution. If larger exposures are required, we will see fewer infections. This is the primary difference between measles and COVID-19.
One final note about long range transmission: we really don’t know how common it is in COVID-19. Identification of long range transmission is incredibly difficult unless there are a very small number of cases. With a small outbreak of measles cases, it is easier to determine exactly where individuals were, and identify airborne transmission. For the vast majority of COVID-19 cases, we do not know how the individual became ill, and so could easily be overlooking long range transmission (especially when the possibility of aerosol transmission is dismissed out of hand in some circles). In fact, there seems to be pretty good evidence of long range transmission in many of the super-spreader events discussed below.
Our current approach is working
Another argument occasionally used to dismiss aerosols as a mode of transmission is that our current PPE approach seems to be working in hospitals. First, I would point out that healthcare workers are contracting COVID-19 at a rate that is far higher than the general population, so this argument is pretty weak. Furthermore, as will be explored further below, there are many other factors that significantly dilute aerosols in most hospitals, like excellent ventilation, good distancing, and masking of both patients and providers. Although not quite as good as N95s, well fitting surgical masks will still filter out as much as 80% of infectious aerosols. (Makison Booth 2013) Combined with the low infectivity of SARS-CoV-2, these factors keep us relatively safe even when we stubbornly ignore the science that suggests aerosols are very important in the transmission of COVID-19.
Particle size
Many of the arguments against the aerosol spread of COVID-19 rely on incorrect assumptions about particle size. I went into this at length in the first post, so won’t repeat myself here. The basic summary is that particles of sizes that many articles refer to as droplets actually remain airborne for prolonged periods, and are therefore better classified as aerosols for the purposes of transmission. Just be careful when reading articles, because many don’t define these terms. When I use the term aerosol here, I am referring to any droplet that remains suspended in the air for longer that a few seconds, whatever the size, because that is the feature that matters for infection control.
The lack of definitive proof
Some of the arguments against aerosol transmission simply assume droplet transmission and demand “definitive proof” for aerosol transmission. I won’t attempt a treatise on the philosophy of science here, but that is an unreasonable bar.
One version of this argument states that viable SARS-CoV-2 has never been isolated from the air, and therefore we cannot definitively prove airborne transmission. This demand is unreasonable. Measles and tuberculosis are both known to be airborne, and no one has been able to isolate viable pathogens for either from the air. (Jimenez 2020) Furthermore, this is probably an outdated argument, as multiple studies actually have identified viable SARS-CoV-2 in the air. (Lednicky 2020; Santarpia 2020a)
The specifics of whether or not viable virus has been cultured from air samples is irrelevant. The point is that unfair standards are being used when comparing aerosols and droplets. There is no definitive proof that SARS-CoV-2 spreads through large droplets. (Jimenez 2020) It is crazy to require such stringent proof of aerosol transmission, while simultaneously just assuming droplet transmission is occurring. The same standards must be required for both claims. We are unlikely to have ‘definitive proof’ of either claim. Our decisions must be made based on the preponderance of the evidence.
There is good evidence that COVID-19 spreads through aerosols
Although there is no “smoking gun”, the evidence that COVID-19 spreads through aerosols is relatively strong. Below I outline the various converging areas of science that convince me that aerosols are a major route of SARS-CoV-2 transmission.
Animal data
The animal data is not perfect, but suggests aerosol spread. Animal studies definitely show that SARS-COV-2 can be transmitted ‘through the air’, but most of these studies have done an inadequate job of distinguishing between aerosols and droplets. (Richard 2020; Sia 2020)
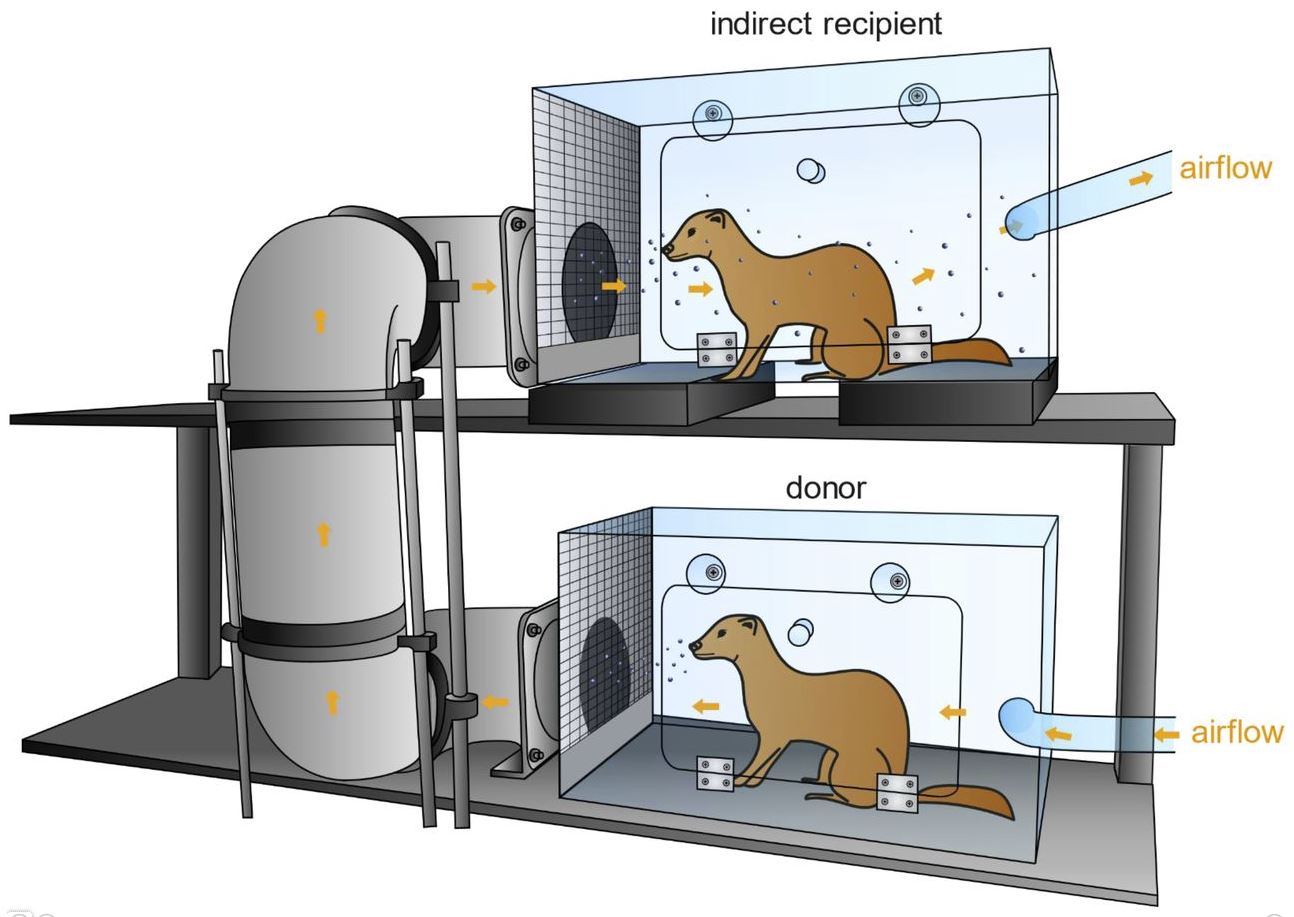
In the original post, I discussed research in ferrets that pretty definitely showed that influenza can be spread through aerosols. A similar study has now been replicated using both SARS-CoV1 and SARS-CoV-2. Healthy ferrets were placed in a cage that was above infected ferrets (as droplets should not rise against gravity) and the cages were connected with pipes that had a series of 90 degree bends (as droplets should not make the turns). In the SARS-CoV-1 pairings, all 4 healthy ferrets subsequently tested positive. In the SARS-CoV-2 pairings, 2 of the 4 ferrets tested positive. Thus, the infection spread through the air, around corners, and against gravity, which is inconsistent with droplet transmission, but describes aerosol transmission perfectly. However, the set-up is somewhat artificial, as there were high air flow rates between the cages. It would have been more convincing if they were left with relatively stagnant air. (Kutter 2020) (It is amazing to me that for such a controversial and important subject, this experiment has not been replicated.)
In a similar study in mice, SARS-CoV-2 was transmitted through aerosols, but required longer exposures than transmission by close contact. (Bao 2020) As discussed above, long range aerosol transmission should require longer exposure as the total viral exposure per time is lower.
Although there is no perfect study, the animal studies certainly suggest COVID-19 is aerosol spread.
COVID-19 super-spreaders
The strongest evidence for aerosol transmission of COVID-19 is probably the epidemiologic data. Everyone knows about “super-spreader” events at this point. These cases are so common that most aren’t subject to scientific reporting. Every week, we hear news reports of gatherings that led to very large numbers of new infections. Although it is essentially impossible to prove the route of transmission during these events, this type of large scale transmission has always been assumed to be airborne in the past, and that certainly makes the most sense.
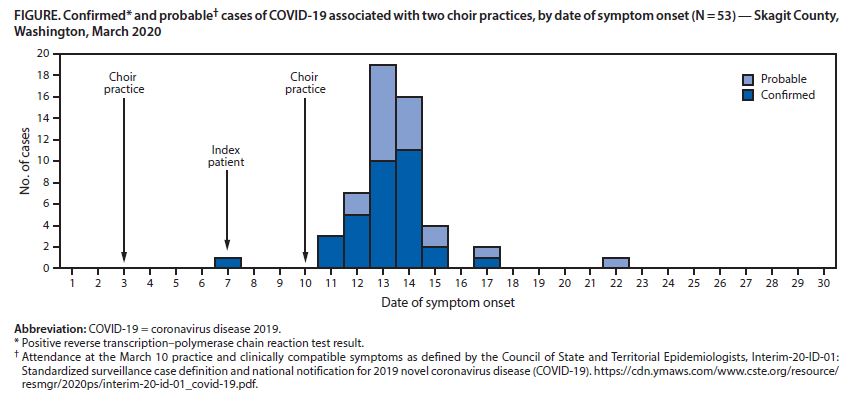
There are too many examples to cover them all, but let’s review a few. The most famous example is probably the choir practice that occurred in Skagit County, Washington in March 2020. 61 people attended a choir practice on March 10th, one of whom had COVID-19. Of the remaining 60, 52 (87%) subsequently contracted the disease (32 were confirmed by PCR and the rest diagnosed clinically). The chairs in the room were only 6-10 inches apart, but most people were further than a few meters from the index patient for most, if not all, of the night. COVID-19 was already a known entity at the time, so some precautions were in place (mostly in keeping with droplet/contact spread). There was no reported physical contact between any of the attendees and most attendees left immediately after the practice. Although the exact mechanism of transmission cannot be confirmed, the incredibly high attack rate simply doesn’t make sense with contact or droplet spread, and the pattern looks exactly like other airborne diseases. (Hamner 2020; Jimenez 2020)
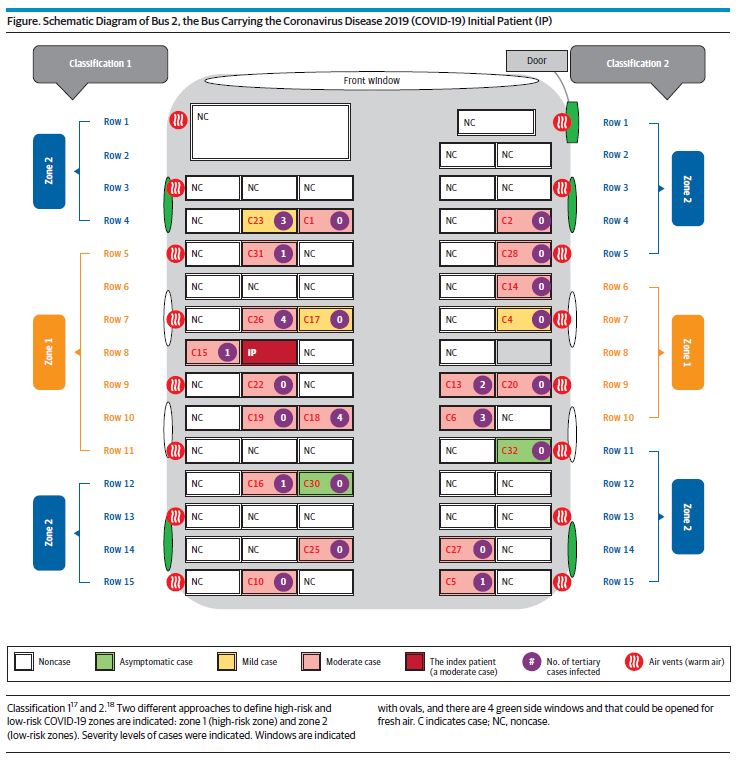
A similar case occurred after an asymptomatic individual took a 50 minute bus ride to and from a religious ceremony, and then developed cough, fever, and chills the evening after the event. Of the 68 individuals on the bus, 24 (35%) were diagnosed with COVID-19. The passengers didn’t change seats or move during the ride, and the infections were relatively evenly spread throughout the bus – a pattern more consistent with airborne spread than droplet. A second bus to the same event acted as a ‘control’ and no passengers were diagnosed with COVID-19. The authors conclude that this event provides “very strong evidence of aerosol transmission”. (Shen 2020)
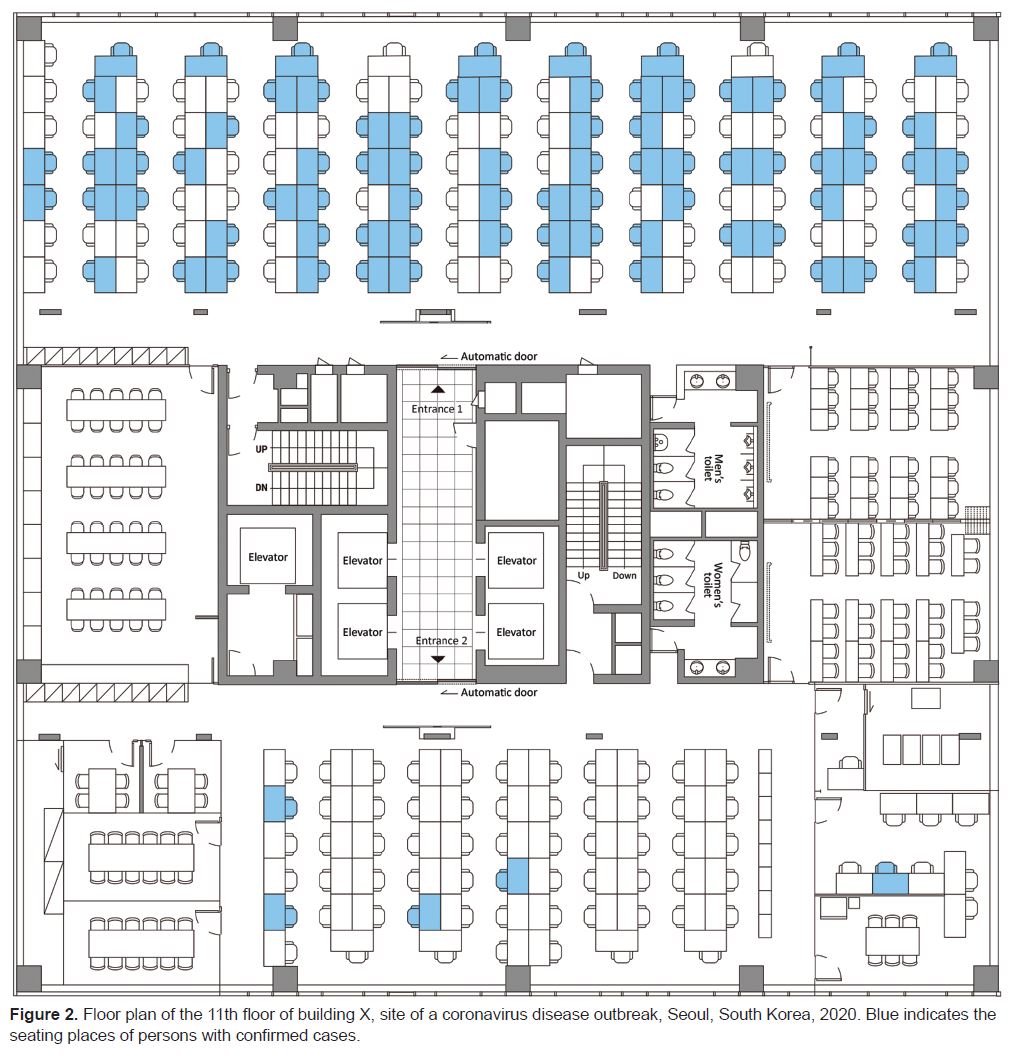
An outbreak in an office building in Korea paints a similar picture. On March 9, they identified a cluster of cases from the building and closed it down. Testing was offered to everyone, and 1,143 (99.8%) accepted. The pattern of exposure again seems to suggest aerosol spread. The outbreak was centered on the 11th floor. Of individuals from other floors who would have been exposed to droplet/contact spread in the lobby and elevators, 3 individuals (0.3%) tested positive for COVID-19. On the 11th floor, 94 individuals (44%) tested positive. The 11th floor is divided in half, but with shared bathrooms, elevators, and lobby. The vast majority of positives were from half of the floor, but on that side the positives are equally distributed, in a pattern more suggestive of aerosol spread than droplet spread, although we don’t know exactly how individuals interacted. The ventilation of the building is not described. (Park 2020)
I find these epidemiologic reports incredibly enlightening. They are clearly indirect evidence. They rely on numerous assumptions. However, on a whole, they seem to provide relatively strong support for the concept that COVID-19 is transmitted through aerosols. There are many more reports of super-spreader outbreaks than I can cover, but they all suggest the same thing: aerosols transmission of COVID-19. (Cai 2020, Li 2020, Almilaji 2020; Bays 2020; Günther 2020; Wallace 2020; Charlotte 2020)
The superspreaders highlight an important issue with COVID-19: the risk of transmission is not evenly distributed. Many infected individuals will not spread the disease at all. One modelling study estimated that 10% of patients are responsible for 80% of disease transmission. (Endo 2020) Another study suggests that 8% of infected individuals are responsible for 60% of secondary cases, while 70% of infected people don’t pass the disease on to anyone else. (Laxminarayan 2020) Another epidemiologic study from Hong Kong reached similar conclusions: 19% of people were responsible for 80% of transmission. (Adam 2020)
The uneven distribution of disease transmission is why simply comparing the Ro among diseases can be misleading, and why many people have heard of “k” or the dispersion factor as a second essential concept. (Kupferschmidt 2020) If instead of looking at population averages, you focus on the smaller number of individuals who are spreading the disease widely, COVID-19 starts to look a lot more like a classic airborne disease.
As I discussed above, the infectivity and mode of transmission are different concepts. The number of people being infected does not prove the mechanism of transmission. However, these super-spreader events are very difficult to explain based on droplet transmission, but easy to explain based on aerosols.
The transmission pattern of COVID-19 may be the strongest indication that aerosols play a significant role in the spread of disease.
Ventilation as a risk factor
Poor ventilation is widely accepted as a risk factor for COVID-19. That being said, with the exception of a few case reports, I haven’t found any studies specifically linking ventilation to the spread of SARS-CoV-2.
Ventilation is a known risk factor for many similar viruses. Inadequate ventilation was identified as a risk factor for the transmission of SARS. (Li 2005) A systematic review found that there is “strong and sufficient evidence to demonstrate the association between ventilation, air movements in buildings and the transmission/spread of infectious diseases such as measles, tuberculosis, chickenpox, influenza, smallpox and SARS.” (Li 2007) Poor ventilation in college dorms has also been associated with increases in seasonal acute respiratory illnesses. (Zhu 2020)
By definition, droplets fall rapidly to the ground and therefore are basically unaffected by ventilation. If ventilation impacts disease transmission, it is strong evidence that the disease is spread by aerosols, as aerosols are the only vector significantly altered by ventilation. This simple fact seems to be overlooked by many governing bodies, resulting in conflicting recommendations. For example, the WHO states that COVID-19 is only spread through droplets but simultaneously emphasizes the need for ventilation in the control of the disease. That doesn’t make sense.
Ventilation is important in the spread of SARS-CoV-1. Ventilation is important in the spread of seasonal respiratory illnesses, which include numerous other coronaviruses. Ventilation really only impacts aerosols, and so this is strong evidence that aerosol transmission is important in the spread of these diseases. We have no reason to believe that the transmission of SARS-CoV-2 is different from these other coronaviruses, so although the evidence is indirect, it again suggests that COVID-19 is transmitted through aerosols.
Indoors versus outdoors
The spread of COVID-19 is more likely in indoors settings. In a review of 318 COVID-19 outbreaks in China, all 318 occurred in an indoor setting. (Qian 2020) A similar study from Japan looked at 110 cases among 11 clusters, and the odds of transmission in an indoor setting was 19 times higher than in an outdoor setting, and the odds of a super-spreader even was 33 times higher indoors than outdoors. (Nishiura 2020) (This ratio will be partly explained by the fact that large gatherings are more likely to occur in indoor settings. It would be interesting to see a study adjust for this fact.)
The preponderance of indoor spread cannot be easily explained if transmission is occurring through droplets. Droplets fall to the ground rapidly, and therefore are mostly unaffected by dilution and breezes in the outdoor setting. The rapid fall of droplets does not provide sufficient time for ultraviolet light to inactivate the virus. When someone sneezes next to you, the chance of a droplet contacting your mucous membranes is unchanged whether you are inside or out. Droplets should be equally infectious indoors and out. In fact, droplets should probably be more infectious outdoors, because masks are more frequently worn inside than out. The fact that COVID-19 transmission occurs so much more frequently in indoor settings is further evidence of the importance of aerosols.
PPE (in)efficacy
Sadly, the one type of research we need most is also the type of research that is most lacking. (Perhaps limited by the stubborn insistence from some circles that COVID-19 is only spread through droplets). How do infection rates vary with different forms of PPE? Unfortunately, as far as I can tell, no one has done studies directly comparing hospitals or countries that are routinely practicing under airborne precautions to those that are not. However, as I previously discussed, there is lots of evidence that healthcare workers are contracting COVID-19 far more often than they should be. There was also some evidence that suggests much lower rates of healthcare worker infections in hospitals that are routinely using N95s or PAPRs. (Koh 2020; Liu 2020) If this holds true, it is yet another line of evidence that COVID-19 spreads through aerosols.
Presymptomatic transmission
This is not a topic I have seen widely discussed, but droplet production is strongly associated with symptoms (coughing and sneezing). Asymptomatic individuals produce far fewer droplets. The fact that asymptomatic spread is clearly playing an important role in COVID-19 is another line of evidence that suggests aerosols are an important mechanism of transmission.
Other evidence
As I reviewed in the initial post, we have known from very early on that SARS-CoV-2 can be found in airborne samples, can survive in aerosols, and can be found in places like air ducts that can’t be reached by droplets. (Guo 2020, Santarpia 2020b, Ong 2020, Liu 2020; Van Doremalen 2020; Fears 2020) Furthermore, some studies have specifically identified viable virus in the air more than 2 meters from the patient. (Lednicky 2020) This data is weak, but parallels all the other lines of evidence that together make it very clear that aerosols are involved in the transmission of COVID-19.
Aug 2021 update: A new study took samples from 23 COVID positive patients while breathing, talking, and singing, and found that 85% of the expired viral load was found in fine aerosols less than 5 um in size. In other words, almost all of the COVID viral particles you will be exposed to are found in aerosols. (Coleman 2021)
When are aerosols formed?
“Aerosol generating procedures” have probably received far too much attention. As I covered in the original aerosol post, aerosols are generated by talking, and are produced in much larger quantities when patients are coughing, have high minute ventilations, or airway collapse. (Tellier 2009; Asadi 2019; Morawska 2006; Fiegel 2006; Wilson 2020) A study measuring aerosol generation while talking concludes that “there is a substantial probability that normal speaking causes airborne virus transmission in confined environments.” (Stadnytskyi 2020) Another study found viable SARS-CoV-2 in the air more than 2 meters from patients in hospital rooms, again leading the authors to conclude that “patients with respiratory manifestations of COVID-19 produce aerosols in the absence of aerosol-generating procedures that contain viable SARS-CoV-2, and these aerosols may serve as a source of transmission of the virus”. (Lednicky 2020) Intubation is one of the highest risk procedures we perform, but a single cough produces as many as 500 times more aerosols than the act of intubation. (Brown 2020)
Aerosols are constantly present. The focus on only a handful of procedures is a dangerous distraction. Inserting a urinary catheter was associated with an increased risk of contracting SARS (RR 5.00 95% CI 2.44-1.023). (Loeb 2004) Being present during an ECG (OR 3.52) and inserting a peripheral IV (RR 3.24) were also associated with an increased rate of transmission of SARS. (Loeb 2004; Raboud 2010) None of these activities are “aerosol generating” but all were found to be high risk.
When combined with the fact that healthcare workers are contracting COVID at a much higher rate than the general population, this data tells us that we need to change our approach. Choosing PPE based on procedures doesn’t seem to be well supported by science. We need to acknowledge the importance of aerosols in all patients, and be particularly wary of coughing and respiratory distress.
Management of aerosols
Hopefully everyone is convinced that we need to take aerosols seriously. I cannot cover every aspect of the science of aerosol management. There are already many experts publishing extensively on the topic, and I think we should just listen to them. (For example, read anything by Jose-Luis Jimenez or Shelly Miller, among many others.) However, the news that COVID-19 is spread through aerosols seems to provoke such pessimistic reactions that I want to briefly cover what it means for management.
First of all, the fact that COVID-19 is aerosol spread makes me very optimistic. Looking at the state of the world in November 2020, it is pretty clear that we are failing in our attempts to manage this disease. If we were already doing everything in our power to fight this pandemic, it would be incredibly depressing. However, the fact that we have been completely ignoring the important role that aerosols are playing in the spread of this disease means that we have an opportunity to improve. That is excellent news.
Thankfully, there are a lot of basic, low cost interventions that anyone can implement, even if major medical institutions choose to ignore this science. Avoid crowded places. Avoid close proximity to others. Avoid poorly ventilated environments. When meeting with others, do it outdoors as much as possible. If you need to be indoors or in close contact with others, do so for as short as possible. Wear a mask when indoors (including vehicles and other enclosed spaces) and avoid misguided souls who aren’t wearing masks. Refrain from activities that significantly increase aerosols production, such as singing, loud talking, or heavy breathing (exercise) in indoor environments. If you have to be in an enclosed space with someone (such as in a car), open the windows to increase ventilation.
The current suggestions, such as physical distancing and mask wearing are good, but they aren’t enough. They remain necessary, but aren’t sufficient. The fact that SARS-CoV-2 is aerosol spread shouldn’t stop any of our current efforts. Instead, we should be looking at the extra precautions we can add to stem the spread of this disease.
Ventilation and filtration
Most “super-spreader” or large transmission events have occurred in indoor settings. The simple public health measure of reducing large indoor gatherings is essential in combating COVID-19. However, the shutdown of indoor venues has had a significant impact on many people’s lives. We need to open businesses, but we need to do so safely. Similarly, those of us working in healthcare who are confined indoors with sick COVID patients also need to be kept safe. A focus on ventilation is essential.
I will not pretend to be an expert on ventilation. There are many aspects to consider, but the most basic is ensuring adequate air exchanges, so that contaminated air is sufficiently replaced with fresh air. The CDC recommends 6-12 air changes per hour and a minimum of 12 is generally required for hospital negative pressure rooms. (CDC 2019; Li 2007) However, the efficacy of ventilation is dependent on the number of people in the room. A better metric may be liters exchanged per second per person (L/p/s) – which measures the same airflow, but adjusts for the number of people in the space (and therefore the total number of aerosols being produced). Recommendations target at least 10 L/s/p, but ideally 20-25 L/s/p to prevent aerosol spread of COVID-19. (REHVA 2020)
One problem is that ventilation is difficult for the average person to assess. If my local barbeque joint is full of conspiracy theorists who refuse to wear masks, the decision is easy to shop somewhere else. However, how am I supposed to know whether a restaurant has adequate ventilation? One interesting proposal is to use carbon dioxide levels as a surrogate measure of adequate ventilation. The concept is well described in this article. There are cheap (approximately $150) CO2 monitors that could give us a real time indication of ventilation. The ambient concentration of carbon dioxide is about 410 parts per million. A concentration above approximately 800 that is an indication that you are rebreathing exhaled air and therefore other people’s aerosols. (Rudnik 2003) It is not a perfect surrogate. Filtration could effectively remove all aerosols, but leave the CO2 level unchanged. However, it is a reasonable concept that could potentially increase the safety of indoor dining dramatically. (To be clear, although this is a promising theory, there is no evidence that these monitors actually decrease transmission, but they might be worth trying. The potential return on investment is massive.)
Air filtration also makes sense. I have seen many claims that suggest that the excellent filtration in modern aircraft is the primary reason we have seen so few outbreaks on airplanes. I have not reviewed the evidence on filtration specifically, but again there are many experts to guide us if we are willing to accept aerosol spread and ask for their help.
If you want more information, there are some very in depth reviews on ventilation, filtration, and indoor air flow patterns that can get you started. (Lipinski 2020; Jayaweera 2020)
Upper room UV light
Germicidal ultraviolet light is another interesting topic on which I have barely scratched the surface. Using a tuberculosis model and animal testing, upper room UV light was show to decrease the rate of infection by approximately 80% in a simulated hospital setting. (Mphaphlele 2015) Laboratory studies have indicated that UV light is effective at inactivating both SARS and influenza, so it should theoretically work against COVID-19 as well. (Darnell 2004; McDevitt 2012) Interestingly, high intensity ultraviolet light has been suggested to manage measles outbreaks as far back as 1978. (Riley 1978) There is also a CDC/NIOSH guideline on ultraviolet germicidal irradiation for the management of tuberculosis in healthcare settings. I do not yet know the science well enough to know where and when UV light should be implemented, but once we accept that evidence that aerosols are important in the spread of COVID-19, it is another potential tool at our disposal.
Masks
The role of masks in reducing the transmission of COVID-19 is a massive topic that will need its own blog post in the future. However, the acknowledgement of aerosol transmission of COVID-19 does necessitate at least a few comments about the role of masks.
Although it is true that N95s filter more aerosols than surgical masks, it is a misconception that surgical masks are useless against aerosols. A well fitting surgical mask will filter the majority of the larger (>1 micron) aerosols that are thought to be transmitting COVID-19. (Jimenez 2020; Shakya 2017; Makison Booth 2013) In one study of live patients with acute respiratory illnesses, surgical masks were shown to block 100% of seasonal coronavirus droplets and aerosols, although the efficacy was lower for other viruses. (Leung 2020)
Surgical masks are not 100% effective, but that doesn’t make them ineffective. Remember, the concentration of aerosols drops dramatically with distance. When combined with decent ventilation and the relatively low infectivity of SARS-CoV-2, an 80% effective surgical mask may be enough for most situations (and is certainly better than no mask).
Of course, the fact that COVID-19 is aerosol spread means that N95s are going to be important in high risk scenarios, especially in health care. It still isn’t clear exactly when N95s are needed, but the rate of infections in healthcare workers indicates that we probably should be using them more often than we currently are.
Unfortunately, the N95 is a limited resource. In an ideal world, we would use N95s for all patients with suspected COVID-19. That was our approach to SARS and MERS. Unfortunately, the world in 2020 is not ideal, and the supply of PPE is not endless. The appropriate response to this problem is to acknowledge that COVID-19 is aerosol spread and ensure that healthcare workers have appropriate PPE. That should be an absolute top priority for all hospitals and all levels of government. However, in the meantime, we have to decide what to do with our limited supply.
There are no perfect answers. In many places, people are wearing the same N95 for entire shifts, day after day. Many places are reusing or reprocessing N95s that are designed to be disposable. The evidence that this is safe is scant, at best.
I think the science of aerosols can guide us. All patients are producing aerosols, so we need to abandon the outdated ‘aerosol generating procedure’ paradigm. However, we must also acknowledge that, although healthcare workers are getting sick far more than they should be, the absolute rate is still low. By now, we have all been exposed to SARS-CoV-2 while not wearing an N95, but very few of us actually contracted the virus. The infectivity of SARS-CoV-2 is relatively low. Surgical masks, although imperfect, are still pretty good. Hospitals generally have excellent ventilation. Brief patient encounters keep our total aerosol exposure low, and when we are in patient rooms, a small amount of physical distancing significantly decreases aerosol exposure.
These factors combine to mean that, for the average patient, a surgical mask and “droplet precautions” may be adequate. It will not be perfect. The occasional healthcare worker will still get sick, but the rate will be very low. Although I don’t think any healthcare worker should get sick at work, this small risk is probably much better than the risk we would face after running out of N95s.
So how should we decide when to wear an N95? The aerosol generating procedure paradigm doesn’t work. Procedures don’t produce aerosols, patients do. However, the factors discussed above provide a framework that can guide our decisions. Aerosols are most concentrated close to the patient. Coughing patients and those in respiratory distress produce far more aerosols. Total exposure is correlated with time.
Therefore, if I have a patient in respiratory distress, and I have to spend a long time in close contact with the patient (such as while placing a central line), I will definitely wear full airborne PPE, whether or not there is technically an ‘aerosol generating procedure’ occurring. However, for a 3 minute assessment of a patient with mild coryza, most of which I can do from across the room, the risk is low enough that I will wear droplet precautions and preserve those precious N95s for when I truly need them.
Putting it together
Almost everyone now admits that aerosols play a role in the transmission of SARS-CoV-2, even in the absence of aerosol generating procedures. However, many still debate or downplay the magnitude of aerosol transmission. Based on this extensive review of the literature, I think it is very clear that aerosols play a considerable role in the transmission of COVID-19, and that we are unlikely to prevail against this pandemic unless we acknowledge that fact.
The arguments against aerosol transmission are logically fallacious and conflict with available science. The Ro of a disease does not define its mechanism of transmission, but even if it did, the Ro of COVID-19 is very similar to that of the prototypical airborne disease of tuberculosis. Aerosol transmission is much more likely to occur over short distances, but even if aerosol transmission was defined by long distance spread, there are countless super-spread events that seem to fit the mold.
Many lines of research all support the important role of aerosols in the transmission of COVID-19. There is animal data that strongly suggests airborne spread. The epidemiology of super-spreaders is explained far better by aerosol than droplet transmission. The role of ventilation in preventing disease transmission suggests aerosols. The fact that infections predominantly occur indoors suggests aerosol spread. Presymptomatic transmission suggests aerosols. The preponderance of the evidence is clearly on the side of aerosol transmission.
In contrast, there is almost no evidence for droplet transmission. That claim has not been based on science. It is based on opinion and historical medical momentum. The conversation about aerosols and droplets has been rather biased from the outset. Many refuse to acknowledge the possibility of aerosol transmission unless there is definitive proof, but simultaneously accept droplet transmission, which has even less evidence than aerosols.
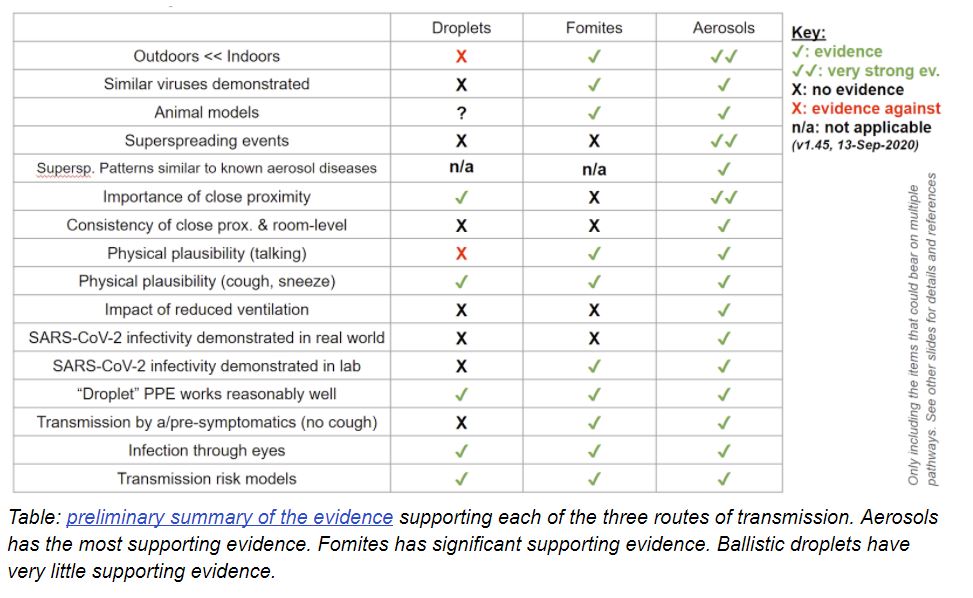
This table from Jose-Luis Jimenez provides a nice summary of the many types of evidence, and demonstrates that the evidence for aerosol spread is far stronger than the evidence for any other type of transmission.
We are repeating old mistakes, but with worse consequences. In conversations about COVID-19, measles is held up as the prototypical example of an airborne illness. Ironically, we had this same debate about measles, and tuberculosis before that. This article about measles from 1985 states that “most public health authorities believe that the primary mode of transmission is by large respiratory droplets which remain suspended in air for short time intervals. Successful transmission in this manner requires close contact between susceptible individuals and a source patient, usually within 1 m (3 ft).” (Bloch 1985) Sound familiar? The evidence for this claim was essentially identical to the evidence currently being used to claim that COVID-19 is only spread through droplets.
We can no longer keep our heads in the sand. The evidence is clear. Aerosols play a significant role in the transmission of COVID-19.
I think this is a good development. Currently, we are losing the battle. However, the fact that we have been ignoring the science around aerosols means that we have a path forward. If we start to manage aerosol transmission appropriately, there is a chance we can get this pandemic under control.
The basic steps forward are simple. We need to continue following the current recommendations about physical distancing, hand washing, and masks. In addition, we need to be cognizant of the factors that drive aerosol spread: crowds and long times spent in poorly ventilated environments. We need to acknowledge the limitations of the current approach. There is no such thing as a ‘2 meter rule’ – the farther apart the better. We will need to improve our indoor spaces, with a focus on ventilation, filtration, and potentially ultraviolet light decontamination systems.
These are still relatively blunt tools. A key aspect of disease transmission in COVID-19 is the existence of super-spreaders. The majority of secondary cases arise from a relatively small number of individuals. This is clearly a feature of aerosol spread, and our focus on droplets and contact have left us blind to the root causes of this phenomenon. We understand some of the basics (varying viral load, varying aerosol emission, and circumstances that increase aerosol exposure), but too much is still unknown. We need effective interventions to stop these super-spreader outbreaks, and the path to those interventions lies with accepting that aerosol spread is important in the transmission of COVID-19.
Addressing this problem in healthcare settings will be more difficult. We should aim for an adequate supply of PPE, so that all encounters with patients suspected of COVID-19 can be performed with appropriate aerosols precautions. In the meantime, we will have to think carefully about the factors that increase risk. We need to abandon the ‘aerosol generating procedure’ paradigm, as all COVID-19 patients produce aerosols. We need to focus on patients with respiratory complaints, and prioritise providers that need to spend prolonged periods at the bedside.
Bottom Line
Aerosol transmission plays a very important role in the spread of COVID-19. It is essential that we acknowledge the science on this issue if we are going to have any success against this pandemic.
Other reviews
The idea that COVID-19 is spread by aerosols is not a fringe position I made up while wearing a tinfoil hat. Here are some other reviews on the topic you can read.
Fennelly KP. Particle sizes of infectious aerosols: implications for infection control. Lancet Respir Med. 2020 Sep;8(9):914-924. doi: 10.1016/S2213-2600(20)30323-4. Epub 2020 Jul 24. PMID: 32717211 [free full text]
- “The studies reviewed in this paper consistently show that humans produce infectious aerosols in a wide range of particle sizes”
- “Data are accumulating that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes COVID-19, is transmitted by both small and large particle aerosols”
- “These data suggest that health-care workers should be protected from these potentially infectious aerosols when working in close proximity to patients.”
Morawska L, Milton DK. It is Time to Address Airborne Transmission of COVID-19. Clin Infect Dis. 2020 Jul 6:ciaa939. doi: 10.1093/cid/ciaa939. Epub ahead of print. PMID: 32628269 [free full text]
- An open letter to the WHO from 239 scientists
- “Studies by the signatories and other scientists have demonstrated beyond any reasonable doubt that viruses are released during exhalation, talking, and coughing in microdroplets small enough to remain aloft in air and pose a risk of exposure at distances beyond 1–2 m from an infected individual”
- “We are concerned that the lack of recognition of the risk of airborne transmission of COVID-19 and the lack of clear recommendations on the control measures against the airborne virus will have significant consequences”
Prather KA, Wang CC, Schooley RT. Reducing transmission of SARS-CoV-2 Science. 2020; 368(6498):1422-1424. [free full text]
- “A large proportion of the spread of coronavirus disease 2019 (COVID-19) appears to be occurring through airborne transmission of aerosols produced by asymptomatic individuals during breathing and speaking.”
- “Aerosol transmission of viruses must be acknowledged as a key factor leading to the spread of infectious respiratory diseases. Evidence suggests that SARS-CoV-2 is silently spreading in aerosols exhaled by highly contagious infected individuals with no symptoms.”
Public Health Agency of Canada Evidence Brief
- “The available empirical and modeled evidence indicates there is some risk of SARS-CoV-2 virus laden aerosol and droplet dispersion at distances beyond two meters, while epidemiological evidence implicates airborne transmission of SARS-CoV-2 to have occurred in some indoor settings”
If you think there is good scientific evidence for droplet transmission, important studies that I have missed, or any problems with this article, please comment below. The goal of performing an extensive review of the literature is to find the answer that is most likely to be true. I don’t care whether COVID-19 is droplet or aerosol spread. I care that we use the best available science to guide our actions, and will happily adjust as new data becomes available.
April 2021 Update: One of the last standing arguments against the airborne spread of COVID is that the virus had not been cultured from aerosol samples (although the same is true for many other airborne diseases). That is no longer true. Lednicky and colleagues (2021) cultures viable SARS-CoV-2 from multiple patient rooms in the absence of any aerosol generating procedures. The science was already incredibly clear that this is an airborne disease, but this is just another nail in the coffin. Link to paper.
November 2021 Update: A pre-print systematic review concludes that there is “evidence of long-distance airborne transmission of SARS-CoV-2 in indoor community settings”. (Palmer 2021) This is not new to anyone, but long range spread is clearly airborne transmission. Sadly, as of November 2021, despite overwhelming evidence, many places (including Canada) continue to insist that this disease is only spread through large droplets, completely undermining infection control efforts.
Other FOAMed
Aerosols, Droplets, and Airborne Spread: Everything you could possibly want to know
Aerosol and Surface Distribution of SARS-CoV-2 (COVID-19)
There is a great summary table of all the evidence for airborne transmission for COVID, SARS, MERS, measles, influenza, chickenpox, and tuberculosis that can be found here. Side by side, it is clear that there is actually better evidence for COVID being airborne (and influenza for that matter) than there is for measles.
References
Adam DC, Wu P, Wong JY, et al. Clustering and superspreading potential of SARS-CoV-2 infections in Hong Kong Nat Med. 2020; 26(11):1714-1719.
Almilaji O, Thomas P. Air recirculation role in the infection with COVID-19, lessons learned from Diamond Princess cruise ship. medRxiv 2020;2020.07.08.20148775.
Asadi S, Wexler AS, Cappa CD, Barreda S, Bouvier NM, Ristenpart WD. Aerosol emission and superemission during human speech increase with voice loudness. Sci Rep. 2019;9(1):2348. Published 2019 Feb 20. doi:10.1038/s41598-019-38808-z PMID: 30787335
Bao L, Gao H, Deng W, Lv Q, Yu H, Liu M, Yu P, Liu J, Qu Y, Gong S, Lin K, Qi F, Xu Y, Li F, Xiao C, Xue J, Song Z, Xiang Z, Wang G, Wang S, Liu X, Zhao W, Han Y, Wei Q, Qin C. Transmission of Severe Acute Respiratory Syndrome Coronavirus 2 via Close Contact and Respiratory Droplets Among Human Angiotensin-Converting Enzyme 2 Mice. J Infect Dis. 2020 Jul 23;222(4):551-555. doi: 10.1093/infdis/jiaa281. PMID: 32444876
Bays DJ, Nguyen MH, Cohen SH, Waldman S, Martin CS, Thompson GR, Sandrock C, Tourtellotte J, Pugashetti JV, Phan C, Nguyen HH, Warner GY, Penn BH. Investigation of Nosocomial SARS-CoV-2 Transmission from Two Patients to Health Care Workers Identifies Close Contact but not Airborne Transmission Events. Infect Control Hosp Epidemiol. 2020 Jul 3:1-22. doi: 10.1017/ice.2020.321. Epub ahead of print. PMID: 32618530
Bloch AB, Orenstein WA, Ewing WM, Spain WH, Mallison GF, Herrmann KL, Hinman AR. Measles outbreak in a pediatric practice: airborne transmission in an office setting. Pediatrics. 1985 Apr;75(4):676-83. PMID: 3982900
Brown J, Gregson FKA, Shrimpton A, Cook TM, Bzdek BR, Reid JP, Pickering AE. A quantitative evaluation of aerosol generation during tracheal intubation and extubation. Anaesthesia. 2020 Oct 6:10.1111/anae.15292. doi: 10.1111/anae.15292. Epub ahead of print. PMID: 33022093
Cai J, Sun W, Huang J, Gamber M, Wu J, He G. Indirect Virus Transmission in Cluster of COVID-19 Cases, Wenzhou, China, 2020. Emerg Infect Dis. 2020 Jun;26(6):1343-1345. doi: 10.3201/eid2606.200412. Epub 2020 Jun 17. PMID: 32163030
CDC Centers for Disease Control and Prevention. Guidelines for Environmental Infection Control in Health-Care Facilities. US Dept of Health and Human Services Centers for Disease Control and Prevention. 2003. Updated July 2019.https://espanol.cdc.gov/infectioncontrol/pdf/guidelines/environmentalguidelines-P.pdf
Charlotte N. High Rate of SARS-CoV-2 Transmission due to Choir Practice in France at the Beginning of the COVID-19 Pandemic [Internet]. Epidemiology; 2020. Available from: http://medrxiv.org/lookup/doi/10.1101/2020.07.19.20145326
Chen W, Zhang N, Wei J, Yen H, Li Y. Short-range airborne route dominates exposure of respiratory infection during close contact Building and Environment. 2020; 176:106859-.
Coleman KK, Tay DJW, Sen Tan K, Ong SWX, Son TT, Koh MH, Chin YQ, Nasir H, Mak TM, Chu JJH, Milton DK, Chow VTK, Tambyah PA, Chen M, Wai TK. Viral Load of SARS-CoV-2 in Respiratory Aerosols Emitted by COVID-19 Patients while Breathing, Talking, and Singing. Clin Infect Dis. 2021 Aug 6:ciab691. doi: 10.1093/cid/ciab691. Epub ahead of print. PMID: 34358292
Darnell ME, Subbarao K, Feinstone SM, Taylor DR. Inactivation of the coronavirus that induces severe acute respiratory syndrome, SARS-CoV Journal of Virological Methods. 2004; 121(1):85-91.
Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and Surface Distribution of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospital Wards, Wuhan, China, 2020 [published online ahead of print, 2020 Apr 10]. Emerg Infect Dis. 2020;26(7):10.3201/eid2607.200885. doi:10.3201/eid2607.200885 PMID: 32275497
Endo A; Centre for the Mathematical Modelling of Infectious Diseases COVID-19 Working Group, Abbott S, Kucharski AJ, Funk S. Estimating the overdispersion in COVID-19 transmission using outbreak sizes outside China. Wellcome Open Res. 2020 Jul 10;5:67. doi: 10.12688/wellcomeopenres.15842.3. PMID: 32685698; PMCID: PMC7338915.
Fears SC, Klimstra WB, Duprex P, Hartman A, Weaver SC, Plante KS, et al. Persistence of severe acute respiratory syndrome coronavirus 2 in aerosol suspensions. Emerg Infect Dis. 2020 Sep. https://doi.org/10.3201/eid2609.201806
Fiegel J, Clarke R, Edwards DA. Airborne infectious disease and the suppression of pulmonary bioaerosols. Drug Discov Today. 2006;11(1-2):51–57. doi:10.1016/S1359-6446(05)03687-1 PMID: 16478691
Guenther, Thomas and Czech-Sioli, Manja and Indenbirken, Daniela and Robitailles, Alexis and Tenhaken, Peter and Exner, Martin and Ottinger, Matthias and Fischer, Nicole and Grundhoff, Adam and Brinkmann, Melanie, Investigation of a superspreading event preceding the largest meat processing plant-related SARS-Coronavirus 2 outbreak in Germany (July 17, 2020). Available at SSRN: https://ssrn.com/abstract=3654517 or http://dx.doi.org/10.2139/ssrn.3654517
Hamner L, Dubbel P, Capron I, et al. High SARS-CoV-2 Attack Rate Following Exposure at a Choir Practice — Skagit County, Washington, March 2020. MMWR Morb Mortal Wkly Rep 2020;69:606–610. DOI: http://dx.doi.org/10.15585/mmwr.mm6919e6
Jayaweera M, Perera H, Gunawardana B, Manatunge J. Transmission of COVID-19 virus by droplets and aerosols: A critical review on the unresolved dichotomy. Environ Res. 2020 Sep;188:109819. doi: 10.1016/j.envres.2020.109819. Epub 2020 Jun 13. PMID: 32569870
Jimenez JL. COVID-19 Data Dives: Why Arguments Against SARS-CoV-2 Aerosol Transmission Don’t Hold Water – Medscape – Jul 30, 2020. Available at: https://www.medscape.com/viewarticle/934837?src=uc_mscpedt&faf=1#vp_1
Koh FH, Tan MG, Chew MH. The fight against COVID-19: disinfection protocol and turning over of CleanSpace® HALO™ in a Singapore Hospital. Updates Surg. 2020 Jun;72(2):311-313. doi: 10.1007/s13304-020-00809-3. Epub 2020 May 27. PMID: 32462609
Kupferschmidt K. Why do some COVID-19 patients infect many others, whereas most don’t spread the virus at all? Science. 2020; [article]
Kutter JS, de Meulder D, Bestebroer TM, et al. SARS-CoV and SARS-CoV-2 are transmitted through the air between ferrets over more than one meter distance. bioRxiv 2020;2020.10.19.345363. Preprint: https://www.biorxiv.org/content/10.1101/2020.10.19.345363v1.article-metrics
Laxminarayan R, Wahl B, Dudala SR, et al. Epidemiology and transmission dynamics of COVID-19 in two Indian states. Science 2020;eabd7672.
Lednicky JA, Lauzardo M, Fan ZH, Jutla A, Tilly TB, Gangwar M, Usmani M, Shankar SN, Mohamed K, Eiguren-Fernandez A, Stephenson CJ, Alam M, Elbadry MA, Loeb JC, Subramaniam K, Waltzek TB, Cherabuddi K, Morris JG Jr, Wu CY. Viable SARS-CoV-2 in the air of a hospital room with COVID-19 patients. medRxiv [Preprint]. 2020 Aug 4:2020.08.03.20167395. doi: 10.1101/2020.08.03.20167395. Update in: Int J Infect Dis. 2020 Sep 16;: PMID: 32793914
Lednicky JA, Lauzardo M, Fan ZH, et al. Viable SARS-CoV-2 in the air of a hospital room with COVID-19 patients International Journal of Infectious Diseases. 2020; 100:476-482. [full text]
Leung NHL, Chu DKW, Shiu EYC, Chan KH, McDevitt JJ, Hau BJP, Yen HL, Li Y, Ip DKM, Peiris JSM, Seto WH, Leung GM, Milton DK, Cowling BJ. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat Med. 2020 May;26(5):676-680. doi: 10.1038/s41591-020-0843-2. Epub 2020 Apr 3. Erratum in: Nat Med. 2020 May 27;: PMID: 32371934
Li Y, Huang X, Yu IT, Wong TW, Qian H. Role of air distribution in SARS transmission during the largest nosocomial outbreak in Hong Kong. Indoor Air. 2005 Apr;15(2):83-95. doi: 10.1111/j.1600-0668.2004.00317.x. PMID: 15737151
Li Y, Leung GM, Tang JW, Yang X, Chao CY, Lin JZ, Lu JW, Nielsen PV, Niu J, Qian H, Sleigh AC, Su HJ, Sundell J, Wong TW, Yuen PL. Role of ventilation in airborne transmission of infectious agents in the built environment – a multidisciplinary systematic review. Indoor Air. 2007 Feb;17(1):2-18. doi: 10.1111/j.1600-0668.2006.00445.x. PMID: 17257148
Li Y, Qian H, Hang J, et al. Evidence for probable aerosol transmission of SARS-CoV-2 in a poorly ventilated restaurant. medRxiv 2020;2020.04.16.20067728.
Lipinski T, Ahmad D, Serey N, Jouhara H. Review of ventilation strategies to reduce the risk of disease transmission in high occupancy buildings International Journal of Thermofluids. 2020; 7-8:100045-.
Liu M, Cheng SZ, Xu KW, Yang Y, Zhu QT, Zhang H, Yang DY, Cheng SY, Xiao H, Wang JW, Yao HR, Cong YT, Zhou YQ, Peng S, Kuang M, Hou FF, Cheng KK, Xiao HP. Use of personal protective equipment against coronavirus disease 2019 by healthcare professionals in Wuhan, China: cross sectional study. BMJ. 2020 Jun 10;369:m2195. doi: 10.1136/bmj.m2195. PMID: 32522737
Liu Y, Yu ZN, et al. Aerodynamic Characteristics and RNA Concentration of SARS-CoV-2 Aerosol in Wuhan Hospitals during COVID-19 Outbreak. 2020. Preprint, not peer reviewed, here.
Loeb M, McGeer A, Henry B, et al. SARS among critical care nurses, Toronto. Emerg Infect Dis. 2004;10(2):251–255. doi:10.3201/eid1002.030838 PMID: 15030692
Ma Y, Horsburgh CR, White LF, Jenkins HE. Quantifying TB transmission: a systematic review of reproduction number and serial interval estimates for tuberculosis. Epidemiol Infect. 2018 Sep;146(12):1478-1494. doi: 10.1017/S0950268818001760. Epub 2018 Jul 4. PMID: 29970199
Makison Booth C, Clayton M, Crook B, Gawn JM. Effectiveness of surgical masks against influenza bioaerosols. J Hosp Infect. 2013 May;84(1):22-6. doi: 10.1016/j.jhin.2013.02.007. Epub 2013 Mar 14. PMID: 23498357
McDevitt JJ, Rudnick SN, Radonovich LJ. Aerosol Susceptibility of Influenza Virus to UV-C Light Appl. Environ. Microbiol.. 2012; 78(6):1666-1669.
Morawska L. Droplet fate in indoor environments, or can we prevent the spread of infection?. Indoor Air. 2006;16(5):335–347. doi:10.1111/j.1600-0668.2006.00432.x PMID: 16948710
Mphaphlele M, Dharmadhikari AS, Jensen PA, Rudnick SN, van Reenen TH, Pagano MA, Leuschner W, Sears TA, Milonova SP, van der Walt M, Stoltz AC, Weyer K, Nardell EA. Institutional Tuberculosis Transmission. Controlled Trial of Upper Room Ultraviolet Air Disinfection: A Basis for New Dosing Guidelines. Am J Respir Crit Care Med. 2015 Aug 15;192(4):477-84. doi: 10.1164/rccm.201501-0060OC. PMID: 25928547
Nielsen, P. V., & Liu, L. (2020). The influence of air distribution on droplet infection and airborne cross infection. Department of Civil Engineering, Aalborg University. DCE Technical Memorandum No. 77 Available at: https://vbn.aau.dk/ws/portalfiles/portal/332256833/The_influence_of_air_distribution_on_droplet_infection_and_airborne_cross_infection.pdf
Nishiura H, Oshitani H, Kobayashi T, et al. Closed environments facilitate secondary transmission of coronavirus disease 2019 (COVID-19) [Internet]. Epidemiology; 2020. Available from: http://medrxiv.org/lookup/doi/10.1101/2020.02.28.20029272
Ong SWX, Tan YK, Chia PY, et al. Air, Surface Environmental, and Personal Protective Equipment Contamination by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) From a Symptomatic Patient JAMA. 2020
Palmer JC, Duval D, Tudge I, et al. Airborne transmission of SARS-CoV-2 over distances greater than two metres: a rapid systematic review. medRxiv 2021;2021.10.19.21265208. https://www.medrxiv.org/content/10.1101/2021.10.19.21265208v1
Prather KA, Wang CC, Schooley RT. Reducing transmission of SARS-CoV-2 Science. 2020; 368(6498):1422-1424. Available here: https://science.sciencemag.org/content/368/6498/1422
Qian H, Miao T, Liu L, Zheng X, Luo D, Li Y. Indoor transmission of SARS-CoV-2. Indoor Air. 2020 Oct 31. doi: 10.1111/ina.12766. Epub ahead of print. PMID: 33131151
Raboud J, Shigayeva A, McGeer A, et al. Risk factors for SARS transmission from patients requiring intubation: a multicentre investigation in Toronto, Canada. PLoS One. 2010;5(5):e10717. Published 2010 May 19. doi:10.1371/journal.pone.0010717 PMID: 20502660
REHVA. REHVA COVID-19 guidance document. How to operate HVAC and other building service systems to prevent the spread of the coronavirus (SARS-CoV-2) disease (COVID-19) in workplaces. November 17, 2020. Available at: https://www.rehva.eu/fileadmin/user_upload/REHVA_COVID-19_guidance_document_V4_23112020_V2.pdf
Richard M, Kok A, de Meulder D, Bestebroer TM, Lamers MM, Okba NMA, Fentener van Vlissingen M, Rockx B, Haagmans BL, Koopmans MPG, Fouchier RAM, Herfst S.
Riley EC, Murphy G, Riley RL. Airborne spread of measles in a suburban elementary school. Am J Epidemiol. 1978 May;107(5):421-32. doi: 10.1093/oxfordjournals.aje.a112560. PMID: 665658.
SARS-CoV-2 is transmitted via contact and via the air between ferrets. Nat Commun. 2020 Jul 8;11(1):3496. doi: 10.1038/s41467-020-17367-2. PMID: 32641684
Rudnick SN, Milton DK. Risk of indoor airborne infection transmission estimated from carbon dioxide concentration. Indoor Air. 2003 Sep;13(3):237-45. doi: 10.1034/j.1600-0668.2003.00189.x. PMID: 12950586
Santarpia JL, Herrera VL, Rivera DN, et al. The Infectious Nature of Patient-Generated SARS-CoV-2 Aerosol [Internet]. Infectious Diseases (except HIV/AIDS); 2020. Available from: http://medrxiv.org/lookup/doi/10.1101/2020.07.13.20041632
Santarpia JL, Rivera DN, et al. Transmission Potential of SARS-CoV-2 in Viral Shedding Observed at the University of Nebraska Medical Center. 2020. Preprint here.
Shakya KM, Noyes A, Kallin R, Peltier RE. Evaluating the efficacy of cloth facemasks in reducing particulate matter exposure. J Expo Sci Environ Epidemiol. 2017 May;27(3):352-357. doi: 10.1038/jes.2016.42. Epub 2016 Aug 17. PMID: 27531371.
Shen Y, Li C, Dong H, Wang Z, Martinez L, Sun Z, Handel A, Chen Z, Chen E, Ebell MH, Wang F, Yi B, Wang H, Wang X, Wang A, Chen B, Qi Y, Liang L, Li Y, Ling F, Chen J, Xu G. Community Outbreak Investigation of SARS-CoV-2 Transmission Among Bus Riders in Eastern China. JAMA Intern Med. 2020 Sep 1:e205225. doi: 10.1001/jamainternmed.2020.5225. Epub ahead of print. PMID: 32870239
Sia SF, Yan LM, Chin AWH, Fung K, Choy KT, Wong AYL, Kaewpreedee P, Perera RAPM, Poon LLM, Nicholls JM, Peiris M, Yen HL. Pathogenesis and transmission of SARS-CoV-2 in golden hamsters. Nature. 2020 Jul;583(7818):834-838. doi: 10.1038/s41586-020-2342-5. Epub 2020 May 14. PMID: 32408338
Stadnytskyi V, Bax CE, Bax A, Anfinrud P. The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission. Proc Natl Acad Sci U S A. 2020 Jun 2;117(22):11875-11877. doi: 10.1073/pnas.2006874117. Epub 2020 May 13. PMID: 32404416
Tellier R. Aerosol transmission of influenza A virus: a review of new studies. J R Soc Interface. 2009;6 Suppl 6(Suppl 6):S783–S790. doi:10.1098/rsif.2009.0302.focus PMID: 19773292
Tellier R, Li Y, Cowling BJ, Tang JW. Recognition of aerosol transmission of infectious agents: a commentary. BMC Infect Dis. 2019 Jan 31;19(1):101. doi: 10.1186/s12879-019-3707-y. PMID: 30704406
van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, Tamin A, Harcourt JL, Thornburg NJ, Gerber SI, Lloyd-Smith JO, de Wit E, Munster VJ. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N Engl J Med. 2020 Apr 16;382(16):1564-1567. doi: 10.1056/NEJMc2004973. Epub 2020 Mar 17. PMID: 32182409; PMCID: PMC7121658.
Wallace M, Hagan L, Curran KG, et al. COVID-19 in correctional and detention facilities—United States, February–April 2020. MMWR Morb Mortal Wkly Rep 2020; 69: 587–90.
Wei J, Li Y. Airborne spread of infectious agents in the indoor environment. Am J Infect Control. 2016 Sep 2;44(9 Suppl):S102-8. doi: 10.1016/j.ajic.2016.06.003. PMID: 27590694
Yu IT, Xie ZH, Tsoi KK, Chiu YL, Lok SW, Tang XP, Hui DS, Lee N, Li YM, Huang ZT, Liu T, Wong TW, Zhong NS, Sung JJ. Why did outbreaks of severe acute respiratory syndrome occur in some hospital wards but not in others? Clin Infect Dis. 2007 Apr 15;44(8):1017-25. doi: 10.1086/512819. Epub 2007 Mar 9. PMID: 17366443
Zhang R, Li Y, Zhang AL, Wang Y, Molina MJ. Identifying airborne transmission as the dominant route for the spread of COVID-19. Proc Natl Acad Sci U S A. 2020 Jun 30;117(26):14857-14863. doi: 10.1073/pnas.2009637117. Epub 2020 Jun 11. Erratum in: Proc Natl Acad Sci U S A. 2020 Oct 13;117(41):25942-25943. PMID: 32527856
Zhu S, Jenkins S, Addo K, Heidarinejad M, Romo SA, Layne A, Ehizibolo J, Dalgo D, Mattise NW, Hong F, Adenaiye OO, Bueno de Mesquita JP, Albert BJ, Washington-Lewis R, German J, Tai S, Youssefi S, Milton DK, Srebric J. Ventilation and laboratory confirmed acute respiratory infection (ARI) rates in college residence halls in College Park, Maryland. Environ Int. 2020 Apr;137:105537. doi: 10.1016/j.envint.2020.105537. Epub 2020 Feb 3. PMID: 32028176
Morgenstern, J. COVID-19 is spread by aerosols (airborne): an evidence review, First10EM, November 30, 2020. Available at:
https://doi.org/10.51684/FIRS.52248



90 thoughts on “COVID-19 is spread by aerosols (airborne): an evidence review”
Thanks for the review and all of the tireless work that went into this. It’s excellent. I completely agree about the evidence for aerosol spread.
I am disappointed at your stance on N95 mask usage. I think we as healthcare workers should not be responsible for rationing our safety equipment. Firefighters don’t do it, paramedics don’t do it, those working in laboratories creating vaccines don’t do it, we shouldn’t have to either, especially 8 months into the pandemic. Instead, the rhetoric should be to acknowledge aerosolized spread and protect our healthcare workers with the best PPE like we would other aerosolized infections like TB as you discuss. I don’t quite follow this line of thinking (“Although I don’t think any healthcare worker should get sick at work, this small risk is probably much better than the risk we would face after running out of N95s.”) If we don’t have enough N95s, this is a government problem and our policies should not be based around supply of PPE available. It should be around the science, as you discussed. Do we even know if we will run out of N95s if we encourage people to wear them with COVID patients or those coughing, in resp distress etc.? How is running out of N95s worse than continuing to not wear them when they’re actually indicated? The focus should not be on how to ration equipment, it should be on how to stay safe. Improving ventilation, eliminating hallway medicine, wearing adequate PPE and having policies that support people like our triage nurses, cleaners, physicians etc. who are encountering suspected COVID patients daily or cleaning rooms that have housed COVID patients for hours need policies to protect them. This starts with us standing up and acknowledging aerosol spread, as you have done, but it also goes along with us supporting the best PPE to protect against aerosol spread–N95s or higher.
Thanks for the comment.
I mostly agree with you, but I think there is a pragmatic component. People are always very anxious about this – but 9 months in, it is very clear that the absolute risk of seeing a COVID patient in incorrect PPE is very low. (We have all been doing it). N95s definitely need to be used more liberally. It’s crazy to me that nurses often spend long periods at the bedside of known COVID patients in respiratory distress on high flow oxygen with only a surgical mask. However, I do think it is possible to take this too far. The kid with the sniffles in the assessment center certainly could be COVID, and people certainly could demand N95s for that scenario, but I think right now that would be harmful, as we need the supplies elsewhere.
Dr Morgenstein you forgot to mention Face Shields and Goggles as essential elements with gloves and gowns in PPE .
Also in some older hospital homes and offices Windows can be open diluting the air .
In Australia there are the older trams where windows can be open and fresh air flows in at the stops not so with the new tightly window closed trams though the Airconditioning might be good .
Trains and Subways are terrible windows cannot be opened air con has not been tested .
Meetings outside as in visiting the Elderly in Outdoor Spaces depends on weather temperature and winds but there can be screens .
As regards ventilation safety indoors new buildings will need to factor this in but renovations are achievable and just as in aircraft ventilation systems can be improved but rapid PCR or daily antigen tests might also help here .
This is fantastic.
Thank you so much for sharing the details of your research review – well-written and helpful. I’m not in the medical profession and have been trying to understand recent studies about COVID-19 transmission, your article will help me explain to friends and family.
“They are spread out through 3 dimensional space, and therefore decrease exponentially with distance.”
They decrease with the cube of the distance but since we’re very rarely in a fully 3-D space (ceiling and floor are often close by) they could decrease with the square of the distance. Either way, “exponentially” is not correct.
Is there a very specific use of “exponentially” that you are referring to? The square of the distance and the cube of the distance are both exponents, and so very literally describe “exponentially”.
“Exponentially” has recently come to be used to mean something like “surprisingly rapidly” but it has a specific meaning. E.g. 2^x rather than x^2. In the context of COVID19, some things are literally exponential some things are not not. So for example if left unchecked, the infections grow exponentially (e.g. doubling every 2 weeks, 2^w).
https://en.wikipedia.org/wiki/Exponential_growth
The most famous example of the difference is the story of the man who asked for his reward to be 1 grain of rice on the first square of a chess board, then each square should have double the previous. The king agreed but the 64th square of the board would contain more rice than there is matter in the universe.
Compare that to 64 squared – 4096.
So for example, gravity, heat, light, sound all fall off as distance^2 because they are spreading out in 3-D space.
And with those examples, I realize I made an error in my first comment. In 3-D COVID aerosol will drop off as 1 with the *square* of the distance (just like sound, light etc) but a confined 3-D space with a floor and ceiling is effectively 2-D so it will drop off linearly with the distance (assuming the infected person is sticks around for a little). So actually it’s very far from exponential drop-off.
I am not an expert here, so I may be wrong, but I think you are conflating “exponentially” with “exponential growth”. I never said exponential growth – or in this case decline. I used the word “exponentially” because the fall off occurs somewhere between the power of 2 and 3, as you say. “Exponential” here refers to the exponent and fits with the dictionary definitions I am seeing, and seems to be the best way to describe the phenomenon. Do you have a suggestion for a better word?
Exponential does not just mean that there is an exponent. Constant terms have an exponent of 0 and linear terms have an exponent of 1 and squares have an exponent of 2 etc, there’s always an exponent. Also square roots have an exponent of .5 and a very slow-growing definitely would not say “exponentially” for square-root growth.
WP’s entry on exponential growth has a section on Other Growth Rates https://en.wikipedia.org/wiki/Exponential_growth#Other_growth_rates because they are not the same.
Here’s another good page on it
https://www.reddit.com/r/incremental_games/comments/2ztcfk/linear_polynomial_exponential_and_more_growth/
And it say “Linear, Polynomial (degree >=2) and Exponential are by far the most common used growth rates for incrementals.”. As you can see they put degree >= 2 into Polynomial growth which is distinct from Exponential growth. Just having an exponent does not make it exponential.
Specifically, in this case, when you consider a room to be more 2-D than 3-D, the volume of virus reaching you drops off linearly with the distance. Which is not even exponential in the colloquial sense. Aerosol modelling is much more complex than this since you have evaporation and deposition on surfaces plus the infected person continues to pump more and more into the air and it really depends on the room, in a small enough room with an infected person breathing constantly, the entire room may be roughly equally loaded with virus and it really doesn’t matter how far away you are, only how long you stay.
Anyway, if this wasn’t an article presenting scientific research, I wouldn’t bother saying anything. If you don’t want to take my word for it, please find your closest mathematician or physicist.
I forgot to address the “exponentially” vs “exponential growth”. Something can be growing exponentially (exponential growth) or decreasing exponentially (exponential decay). In both cases the mean is that we are not dealing with a fixed exponent, like x^2 or x^(-3). They are polynomial growth and decay (respectively). For it to be growing/decaying exponentially you need the input (e..g distance, time, mass) to be in the power. E.g. compound interest (growing exponentially) or radioactive decay (decaying exponentially).
Excellent article. Please keep this topic going. And perhaps a specific one regarding singing as I observe many folks doing that, thinking 2m will protect them. There is no doubt of aerosol transmission, and even many meters distant. 2m rule is only adequate indoors if people are wearing masks. Another example is in Korean Journal Medical Science (Kwon), transmission after 5 minutes exposure at 6.5 meters.
https://jkms.org/DOIx.php?id=10.3346/jkms.2020.35.e415
Well done! You have an impressive literature review, and I agree with your reasoning. If we now switch to a pandemic/public health perspective, simple observation tells us “What we’re doing now isn’t working,” which implies, “We should be doing something else.”
We now know Super Spreader Events (SSEs) are the main transmission path. SSEs combine 6 factors which create the SSE:
1 Unknown, infected person with high aerosol generation
2 Large number of people
3 Not Masked
4 Close proximity
5 Long Time
6 Poor Ventilation
The first 5 are all Human Behavior issues, and as such we can exhort, we can encourage, but we cannot compel adherence.
However, #6 is an Engineering issue, which we can determinatively influence.
For example, it’s proven difficult to impossible to prevent high rates of transmission among low income workers in Los Angeles. They are working in places that expose them to risk, and typically also living in high density situations. If they don’t work they don’t eat.
It’s also almost impossible to close all bars and restaurants, because there is no income replacement scheme in place for the owners or workers. If they don’t work, they don’t eat.
Althouse, Wenger, and Hu showed that Covid19 transmission can be controlled by only controlling SSEs. If there are few enough SSEs, chains of infection die out because most people infect no one, while the few can’t infect many.
Since we’ve failed to reduce SSEs by exhorting people to avoid SSEs, we need to change something. The most obvious is the ventilation factor. From ASHRAE, Shelly Miller and others we know that increasing ventilation indoors reduces risk of infection. The problem is doing this cost effectively. Reworking a building’s HVAC system to bring in more outside air or filter more effectively can be cost prohibitive. However there is a cheap, fast solution which is also good enough to make a difference.
The solution is the lowly box fan/MERV13 filter arrangement for about $50. A typical box fan moves about 500 cfm with a MERV 13 filter attached, and stops 85% of relevant particles for a CADR of ~400. While this is not as ‘good’ as a HEPA filter at 99.5%,it’s also much less expensive and the HEPA CADR is typically only 100 CFM. At 5 air changes per hour the 400 CADR will clear about 4800 cf, or a 20x30x8 room. At 10 air changes, it will clear 20x15x8.
If we put one of those fan/filter rigs in every 300sf of a restaurant or bar, they can reopen. It’s not zero risk, but it’s a lot better than what’s happening now. We can afford to give these to every crowded low income household. We can mandate them in factories, jails, nursing homes and dormitories. Also hospital break rooms and cafeterias.
Now we just have to convince the governors!
https://journals.plos.org/plosbiology/article?id=10.1371/journal.pbio.3000897
https://www.texairfilters.com/how-a-merv-13-air-filter-and-a-box-fan-can-help-fight-covid-19/
Thanks for an excellent review that I continue to return to. Can you comment on the protocol changes you anticipate once frontline workers have been all vaccinated? Will the Protected Code Blue be adjusted once we have a higher level of immunity but disease still exists in the community. In particular our concern of aerosol generating during Bag Valve Mask Ventilation and need for Negative Pressure rooms for intubation. I believe our positive experience with masking (due to lack of Flu and common virus this year) will have us continuing to mask long after COVID is circulating but i”m hoping to be able to avoid anterooms and noisy AIIR soon.
I am honestly not sure what threshold will be required to safely return to our historical practices (or whether our historical practices can really be considered safe). I think the key is getting control of COVID in the community. Having medical staff vaccinated will not be enough if COVID is still running rampant in the community, so the role of vaccines will really be to get the pandemic under control. The best way to keep healthcare providers safe is to eliminate COVID from the community, and that needs to be our goal.
The problem is that this is definitely not going to be the last respiratory illness that we have to deal with, so we need to keep all the lessons we have learned close at hand, and perhaps more important, really spend the next 6 months focusing on what aspects of infection control really matter what which don’t.
Vaccines will get the pandemic under control when 2/3 of the population is immune, which will be about 6 months and 600,000 deaths from now.
IF we merely filter the virus carrying particles out of the air, we can reduce transmission immediately. When Japan told its citizens to avoid crowded indoor spaces without masks, they dramatically reduced transmission within 6 weeks.
In the US at least 30% of people are not following recommendations, because they don’t want to, or can’t. Since only 10% of infected people cause 80% of infections, having 60% of the population following guidelines isn’t much help.
We need something more akin to air bags and guard rails than exhorting people to drive safer.
Peter J Liepmann,
You wrote “When Japan told its citizens to avoid crowded indoor spaces without masks, they dramatically reduced transmission within 6 weeks.” but this did not happen. Japan was telling people to avoid crowded indoor spaces from very early on but by April, R was over 2 and exponential growth was very clear. They called a 5-6 week state of emergency which caused a massive shutdown (all voluntary but still a very large effect, many large stores were shuttered for 5 weeks). This massively reduced cases.
Between masks, weak contact tracing (compared to e.g. South Korea, NZ, Aus) and public behaviour, Japan stayed out of the red until the winter but now it’s in a bad state (nothing compared to the UK in terms of raw numbers but ICUs are full, every day, there’s a news story about someone dying at home after 2 days waiting to be hospitalised etc).
Fergal,
Thanks for making my point for me. Japan DIDN’T do well with voluntary restrictions. Neither has anyone else. And in the US, many people are ignoring restrictions, so they’re not effective.
Japan did very well early on, then relaxed everything, opened everything, in the summer, readmitted foreign students, removed quarantine restrictions, relied on voluntary responsibility, etc., etc.
““We noted many COVID-19 clusters were associated with heavy breathing in close proximity, such as singing at karaoke parties, cheering at clubs, having conversations in bars, and exercising in gymnasiums,” the researchers, including Dr. Yuki Furuse of Kyoto University, wrote in the journal.
The study coincidentally warned that infections are becoming prevalent among younger generations and that they may be spreading the virus without realizing it.
Analyzing 22 probable cases where clusters not related to hospitals originated, the researchers found that half of those infected were between the ages of 20 and 39 — a demographic younger than the age distribution for all COVID-19 cases reported in Japan.
“We also noted probable primary COVID-19 case-patients appear to transmit the virus and generate clusters even in the absence of apparent respiratory symptoms, such as cough,” the researchers wrote.
The number of newly reported cases in Japan has been steadily increasing since the nationwide state of emergency was lifted on May 25 and the country gradually returned to a semblance of normalcy.” https://www.japantimes.co.jp/news/2020/06/27/national/japanese-cluster-study-3cs-warning-coronavirus/
*********************
You’re absolutely right, “The 3 “C’s” ” haven’t helped them much . And it was the decreased interaction from the Emergency that dropped their cases in April. I’m not sure where I saw that business about dropping cases w 3 C’s.
So thanks for making the point- voluntary cooperation doesn’t work well for anyone.
My big point is, we should look at measures that don’t require cooperation, like increased ventilation since enough people are ignoring restrictions to make them moot.
Not sure what your overall thesis is but I would point out that literally everything in Japan has been voluntary. Even the state of emergency had no teeth, it was all social pressure (and some financial compensation with varying degrees of difficulty of access). It actually seems like when the govt say “state of emergency” it just gives license to people to comply, e.g. companies that previously refused work-from-home can no longer deny it, people can decline “invitations” to after-work drinks etc. The SOE also gave license for people to attack and stigmatise businesses that stayed open.
So I actually think that in Japan voluntary stuff works but that’s in a cultural context where what appears voluntary is often not.
BTW, quarantine was not relaxed, there has never been any real quarantine in Japan. The only forceful measure was preventing legal-resident non-citizens from entering the country for an extended period which destroyed the lives and livelihoods of many foreign residents and had questionable impact on the infection stats. They are finally looking at some real penalties for breaking quarantine but it’s politically difficult (as usual, penalties now exists for non-citizens who can now lose their visa if they break quarantine but citizens bear no consequences).
As for “reported cases in Japan has been steadily increasing since the nationwide state of emergency was lifted on May 25” that was true in June when that article was written but actually Japan maintained a stable infection rate for a good chunk of the year. I believe that’s a mix of weather (so outdoors and open doors), improved tested and tracing (nowhere near Korea who had a very similar dynamic but with far low unknown-route-of-infection cases and a far lower baseline of infection).
Personally, I look at South Korea for inspiration. They have dropped a lot of their very invasive tracing stuff and are just doing an awesome job of providing testing to anyone who wants it and then doing the legwork on tracing. They did add some restrictions recently to squash the spike but it was the first time in months. I think voluntary restrictions work well there because they can see that they are the *last* tool in the box, the govt there has done an awesome job without impinging on people and so when they do ask for it, people cooperate. In most other countries, people cooperated well with the first lockdowns because they thought they were buying time for a comprehensive govt response. When their govts squandered that time, compliance dropped.
And all that said, I do agree that systemic fixes that don’t rely on humans are always a good idea but for example in countries where people spend a lot of time in each-others houses (another advantage Japan has, that’s not really a thing) it seems to require individual responsibility/compliance and it’s unclear that systemic fixes that only cover public spaces will be enough to get R < 1.
Firstly, I have to admit, I’m commenting before finishing the article – and I’m very unlikely to chase down all the references.
There’s certainly food for thought here; but in a couple of places, the question seems to be ‘Is this distribution of infection more likely to be die to droplet transmission or aerosol transmission’, when they clearly aren’t the only two options.
Looking at the transmission on the bus – the inferences drawn are based on the idea that only one infected person got on the bus, and infected the others who tested positive. That seems pretty unlikely to be demonstrable to me (though, as I say, I haven’t chased down the reference).
Also, the idea that the other bus was a ‘control’ is simply not the case. Even if the situation of the ‘transmission’ bus was completely as supposed above, the control would need to be one infected individual getting on the other bus, with some notional barrier that prevents aerosol but not droplet transmission.
You are correct that there are no perfect studies, but the same is true for all modes of transmission. The key is to assess the preponderance of the evidence, which is much stronger for aerosol spread than for any other mode of transmission.
For the bus – when they talk about it as a control, I believe they are referring to the fact that these individuals interreacted at the religious event, and so it suggests (weakly) that the transmission happened on the bus rather than at the event.
Read the bus article.
This was early days. China tested EVERYBODY who was at the event. There were very few cases at that time. There was only one index case, who rode the same bus, with the same co passengers, in the same seats to and from the lecture. The index case had no symptoms until later. No one wore masks.
ALL the people who got Covid at that event were on the same bus. They sat all over the auditorium, which was inside/outside with good ventilation. And the closer to the asymptomatic index patient, the higher the risk. The index case developed symptoms within a day, the others 5+ days later. There was no other time/place they were together, and there were no other infections in that district at the time. This was an excellent study.
Aerosol engineers and scientists don’t make a distinction between ‘droplets’ and ‘aerosols’. It’s not useful. But big particles fall to the ground within about a meter or so. People on the bus who were further away got Covid.
The point of this excellent review is that we have good evidence people got infected in many settings, further away than the medical superstition about “droplets” would account for. (PS, TB is ONLY aerosol, though close contact and lots of exposure is needed to be high risk.)
We have good evidence people can be infected through breathing the same air, especially in closed spaces.
That’s actionable information.
Posing contrapositives that contradict the data we have from peer-reviewed journal articles spreads confusion not light. You’re not raising reasonable doubts and you’re not following-or even examining- the evidence we have.
The claim that the index patient on the bus was asymptomatic is debatable. It’s based entirely on personal statements as to whether they had symptoms. In a follow-up investigation the index patient admitted to having “mild” symptoms prior to the bus ride, and experienced myalgia the night of the event. It’s not an entirely un-human thing to lie to absolve themselves of feelings of guilt.
“According to the field investigation report, the index patient reported being asymptomatic during the bus trip and to have started to experience cough, chills, and myalgias on the evening after returning from the temple. However, during follow-up investigations conducted by field investigators in February 2020, the index patient reported that she had had a mild cough the night before the trip”
Thanks for the comment
Agree that details in all these reports are somewhat circumspect.. don’t think symptoms change anything about it being aerosol though.
Completely agree that aerosol emission is the primary mode of transmission for COVID-19. I really like that you are presenting a less restrictive approach to mask use and acknowledging the limitations of most masks. I question the direction of forcing the general population of health and non-symptomatic people while outside of the house and in general public, casual settings like at outside, at a store or in a mall where there people mix in passing. People need to see people, need to be people and need to breathe freely to maintain balanced physical and mental health and immune systems.
Yes, we need to take precautions, but the way in which masks and social distancing are being promoted is also creating toxic mental and physiological environments that viruses and diseases thrive on. We need to take out the fear of breathing and COVID and make it educational and in line with the way physicians and psychologists previously encouraged people to do to improve their health and immune system.
I know this is a bit off topic, but another aspect to consider about the spread of disease and asymptomatic or limited symptomatic people are due to being exposed to a little amount of virus at a time. This initiates a body’s immune response, so the next time the body is exposed it is better prepared to respond. This is natures way of developing immunity without being severely affected by disease. This stated, completely eliminating natural exposure will limit our natural way of building immunity.
The way the world is responding to the virus is weakening our immune system and limiting our natural immune response. Locking down people, taking people away from their support communities and people, restricting breathing, scaring people by focusing on those that died vs those that survive and thrive, and making people feel afraid cough and breathe deeply which is our body’s way of about 70% of our toxins.
Making people believe we need a vaccine to survive this virus is unsubstantiated. Natural exposure to any disease a little at a time, exposes our bodies to a variety of viral strains. Viruses mutate all the time, the key is trying to not to stop exposure, but to limit or allow a gradual exposure to enable our bodies to naturally build our immune response and defenses.
Again, I commend you for taking a more logical and moderate approach to addressing the aerosolized spread of the virus and use of masks.
“They are spread out through 3 dimensional space, and therefore decrease exponentially with distance. ” Why exponentially? Simply spreading out through space would give an inverse square relationship. There will be loss of aerosol (it falls to the ground, evaporates), which would be exponential in the simplest case, but that would be multiplied by 1/x2, and might be insignificant at distances of interest.
From: Prof. Dr Dusan Keber, MD, Ljubljana, Slovenia
Dear DrJustin Morgenstern,
I have only recently come across yor excellent post which I fully agree with. I hereby add some additional epidemiological evidence in favor of aerosol transmission. I would very much appreciate you comment.
Epidemiological evidence
The vast majority of infections, more than 90%, occur indoors. This can be explained by both droplet and aerosol transmission, but mass infections with a single infected person in the room suggest a greater role for aerogenic transmission.
Seasonal fluctuations speak in favour of aerosol transmission. If we ignore the onset of the epidemic, which began in the northern and southern hemispheres at different times of the year, there has been a significant decrease of disease in summer and an increase in winter in both Europe and South America. The prevailing opinion is that higher summer temperatures and more intense UV radiation destroy the virus. This explanation is not necessarily correct. Regardless of the time of year, people spend 80 % or more of their time indoors.It is very likely that due to winter energy savings and poorer ventilation through windows, indoor spaces are more polluted with exhaled air. In the U.S., seasonal fluctuations are less pronounced, perhaps because air conditioning (AC), which covers more than 90% of U.S. homes, people keep windows closed all year round. Because AC only cools or heats the air, but not filters it, Americans are exposed to inhaling an expired aerosol evenly throughout the year. In Saudi Arabia, paradoxically, there was the largest outbreak of infections between July and September: perhaps because the windows are kept closed even more in summer because of the infernal heat than in winter. These observations are therefore consistent with aerogenic transmission but relatively »thin« and need further exploration.
The epidemiological differences between developing and rich countries are more convincing. Experts expected to find higher Covid-19 morbidity and mortality in people living in poor social and economic conditions: overcrowded housing, close contacts, inaccessibility of masks, poor hygienic conditions in which people have neither toilets nor running water – circumstances that should, according to droplet transmission, lead to a massacre. Looking at the world map, however, there is a a surprise: India and all of Africa (except the most developed South Africa) have comparatively very low incidence of infections and deaths. A similar picture has been revealed in refugee camps in which more than twenty million people have been condensed during Covid-19: despite the inhumane conditions, coronavirus infection and mortality are ten times lower among them than in EU countries. This cannot be explained by the fact that refugees are, on average, much younger than the population of developed countries. Experts are inventing hypotheses about the genetic differences and natural selection of the world’s poor, which are highly unlikely: HIV/AIDS and Ebola have been very unforgiving to Africans. I was interested to learn in what was going on in the Brazilian favelas, which are not much better than refugee camps. I found some field studies started on the assumption that a catastrophe would be disclosed, and then were surprised to find that coronavirus morbidity and mortality in the favelas were two to four times lower than in the richer areas of the same cities. They, too, have unconvincing explanations: it is said to be about the good self-organization of the poor and the sacrificial work of humanitarian organizations. Should an advise be given to wealthier Brazilians to take refuge in favelas? I myself have a different explanation: the observations are consistent with airborne transmission and almost completely deny the importance of droplet transmission. It seems that the world’s poor, at least in the case of the coronavirus, have the privilege in the form of the ever-present naturural vcentilation: the roof of their dwellings is the blue sky or non air-tight emergency dwellings blown by the wind.
Dr Dušan Keber
You did not mention the possibility of SARS CoV2 infection transmission from a positive smoker exhaling smoke with infectious droplets into the air indoors and out. Is this studied?
This is the most comprehensive article I’ve found on the subject of virus spreading through aerosols. Is it feasible to add AIR FOGGING (particularly non-toxic HYPOCHLOROUS ACID FOGGING) to the list of research evidence to mitigate virus aerosols…alongside UV Light?
Thanks for the comment. I haven’t come across air fogging in my reading. Do you have any references to science that suggests it could be helpful? All the best – Justin
Back in the early days of antisepsis, 1867, Lister proposed spraying carbolic acid (phenol) in the operating room air to reduce airborne infection. He used it for 15 years until his research showed airborne bacteria were rarely a problem, and thus the (toxic) spray had no benefit.
http://www.museumofhealthcare.ca/explore/exhibitions/listerism.html#:~:text=In%201871%20Lister%20recommended%20that,nor%20removed%20by%20the%20spray.
The problem with spraying bleach in the air is, it’s toxic to people. So,
Yes, you could, but no, the harm is greater than the benefit and there’s safer, cheaper ways to achieve the same end.
There’s some evidence that higher temperature and humidity also reduce Covid counts, but not as much as ventilation/filtration. Thus a humidifier as well as the fan/MPV1550 filter could reduce risk a bit.
The problem we have now is, public health advice is NOT WORKING. California, following CDC, has a higher new case rate than Florida, which never closed restaurants and bars. WHATEVER THE REASON, (I suspect the mechanism is 30% of people, including the 10% who cause 80% of new infections ignoring the advice, but this is IRRELEVANT) the current plan is NOT working, and vaccine immunity will take 6-12 months and 600k more deaths to stop the pandemic.
When what we’re doing is not working, that suggests we should examine the plan and see what might be modified for greater effect. One modification would be to allow people to gather, but require increased ventilation/filtration in all those venues, and making cheap fan/filter rigs available at cost or free. A 20″ box fan runs about $20, and a MERV13 2″ filter runs under $15 in bulk.
If we put these in every slaughterhouse, prison, bar, restaurant, church, or dorm, and gave them away to people living 15 in a 3 BR apartment, we could dramatically reduce the risk in those locations, which is where Covid is being transmitted today.
When what we’re doing isn’t working, we need to consider whether something else might.
Dr. Morgenstern,
Thanks for posting this! I am a bit late to the game here, but perhaps my response will be worthwhile if you post a one-year anniversary update next month.
The evidence continues to mount that COVID-19 is primarily spread by infectious aerosols. The Korean restaurant case where two people were infected by dining 6 m or so downwind of the index patient, one for only five minutes, is quite instructive. I am an HVAC engineer, so perhaps I can comment on the what can and cannot be done by an air conditioning system. First, however, I think we need to distinguish between the small particles emitted by people with the disease and gas molecules. A gas molecule like ethane or oxygen is about 7 orders of magnitude smaller by mass than a virion with no fluid coating from the host. Most likely, the ~125 nm virion is at least 1,000 nm by the time it gets out of the throat and after evaporation remains 300 nm or more.
If the particles were much smaller, say 50 nm or smaller, then just diluting the contaminated air would be adequate because the virions would diffuse into adjacent air packets. However, evidence like the Guangzhou restaurant study shows the virions staying confined to airstreams.
This tells us that we don’t necessarily need the best filters available. MERV 13 filters take out at 75% of the 300 nm particles that flow through them. And, as you note, infection is a numbers game. My guess is that it takes at least 1,000 active virions to infect a person. However, there are many confounding factors that prohibit a clean measurement of the minimum infectious dose or the rate of virion particle production.
Second, as Travis English, a leading Engineer at Kaiser Permanente, published at the most recent ASHRAE (American Society of Heating, Refrigeration and Air Conditioning Engineers) conference, we need to take into account the dilution factors. A person typically breathes out about 6 L/min of air. If the building has reasonably large air handlers of 10,000 cubic feet per minute (300,000 L/min) then the infected person’s breath that gets back to the air handler is diluted by 50 000. At that point, the filtration rate and the outside air dilution rates don’t matter. Filtration is important for smaller systems, however.
Given the speed that infection can occur, the main thing to worry about in a building (and to a lesser extent outdoors) is the speed and direction of slow breezes or drafts. The draft in the Korean restaurant was about 1 m/s or 2 miles per hour. You can feel that airflow, but only if you stop to notice.
For me, I don’t want to be downwind from unmasked people unless the breeze in at least 5 mph. That brings turbulence and significant dilution.
The new vaccines, which I consider essentially miraculous in their ability to virtually eliminate cases serious enough to need a hospital stay, change the risk levels immensely. However, this is not the last airborne pathogen we will face. We need more tools to fight them at the point of infection. 222 nm UV, which people tolerate far better than 254 nm traditional UV light has a great deal of promise. Some ionization technologies also show promise and we would do well as a society to study these to a degree that we have good engineering data available for deploying them safely and effectively.
How long does aerosolized SARS-nCov2 remain active in the air? I have read some studies that say 3 hours is the upper limit and others that say the aerosols remain indefinitely suspended in poor ventilation conditions?
No simple answer. Depends on a very high number of variables like humidity, airflow, and even people moving in the space causing particles that had previously settled to redistribute in the air. There is definitely no upper limit in poorly ventilated spaces. (Picture all the dust in the air in an abandoned building). However, the concentration of virus is likely to fall rapidly if the is any ventilation / volume for distribution. Discussed a little more in the original basic science post: https://first10em.com/aerosols-droplets-and-airborne-spread/
A simple flashlight illuminates pine pollen in the air on a still night in Charlotte, NC. These are 50+ micron particles. Do they look like they want to settle quickly under gravity? Imagine what COVID aerosol can do indoors. 6’?Meh. #COVIDisAirborne
https://twitter.com/Smogdr/status/1380193605176815616
Today, CDC FINALLY admitted surfaces are not a big problem, and we should spend less energy on reducing surface-hand-face transmission. THey’re STILL saying this: “COVID-19 most commonly spreads during close contact and can also be spread by airborne transmission” but should just say, “Covid is PRIMARILY spread by airborne aerosols, most concentrated near an infected person, but which can spread to fill poorly ventilated spaces, and linger like smoke.”
When what we’re doing is not working, that suggests we should examine the plan and see what might be modified for greater effect. One modification would be to allow people to gather, but require increased ventilation/filtration in all those venues, and making cheap fan/filter rigs available at cost or free. A 20″ box fan runs about $20, and a MERV13 2″ filter runs under $15 in bulk.
If we put these in every slaughterhouse, prison, bar, restaurant, church, or dorm, and gave them away to people living 15 in a 3 BR apartment, we could dramatically reduce the risk in those locations, which is where Covid is being transmitted today.
When what we’re doing isn’t working, we need to consider whether something else might.
An excellent well researched paper.I do not know how many
Of politicians and our babudom can understand this
WITH CORRUPT
W H O HOW THIS
WILL REACH DOWN
Excellent review!!!
A nice enough rundown on aerosol biohazards that I’ve only a couple things to add. Resistance by experts to acknowledging this mode of spread probably stemmed from economic considerations and a desire to avoid inculcating panic as countermeasures, the high-tech HVAC systems and mass use of respirators suggested here, are simply too expensive to implement everywhere, and most people don’t have the option of spending a year at home to cut their exposure risks. Mortality with Covid never justified a total curfew, and even had it, the world could never have interrupted production that long. We recall how the peasants continued working in the fields amidst the Black Death while colleagues dropped beside them.
The lesson for public health authorities is clear: You either stop the disease at the very beginning, when the first cases are detected in your country, or not at all. The USA sealed its fate by dithering for two months after January 21, 2020. It may be that delegating the bulk of responsibility for public health to state and local government, as we do, is adequate for control of foodborne illnesses, but not for a global airway pathogen.
Not one of those reasons is a valid reason though. We can’t all stay at home but some of us can and should. Indoor dining should never have reopened with massive ventilation changes and if that wasn’t economic, you don’t get to just kill people anyway. There are so many cheap and easy things you can do once you understand the threat and there so many risks you can avoid when you understand that 6ft outdoors might be safe but indoors it’s not.. The outcome is never going to be better by giving people bad information.
When I am outside running/walking I can smell people who wear axe or similar body spray at more than 20 yards. If I can smell the body spray, does that mean the molecules are getting into my nose, and therfore are these molecules similar in size to covid-19 and am I a risk of infection? Thanks
Thanks for the question. Smell is a good marker of how aerosols spread. (I have been using smoke, but body spray would also work). Of course, just being briefly exposed won’t put you at high risk, but the stronger the smell and the longer the exposure, the higher your risk will be.
I also can small bodys sprays/deodorants etc. through my mask when outside up to about 20 meters. If a smell is getting through my mask, can covid-19 virus also? Is an odor molecule smaller or larger than a covid-19 virus?
Smell molecules are much smaller than virions, at least 1,000 x.
AXE and similar perfumes can be smelled at huge dilution, but aren’t a good analogue for aerosol dispersion, since as John Weems points out, the odor molecules are much smaller than relevant infectious aerosols.
Cigarette smoke is a much better analogue because it IS an aerosol, although it also contains small smelly molecules.
Distribution of aerosol sizes in exhaled breath at Dr. Marr’s Google doc– https://tinyurl.com/FAQ-aerosols
It also turns out that MERV 10 filters with UVGI effectively remove Covid particles, as evidenced by lack of transmission at a gym that used them. https://aaqr.org/articles/aaqr-21-05-oa-0106.pdf
To answer the question above, being around other people’s exhalations, even outside, puts you at SOME risk, but that’s much reduced (1000 or 1,000,000 fold) by dilution and limited time exposure.
To repeat the main point, poorly ventilated enclosed spaces with many people talking loud or singing, for long periods of time, (Dance clubs, churches, etc.) are high risk.
Anything that reduces your exposure, like masks or ventilation, reduces risk of infection.