Morgenstern, J. Key Updates from the 2021 AHA Guideline for the Evaluation and Diagnosis of Chest Pain, First10EM, March 14, 2022. Available at:
https://doi.org/10.51684/FIRS.126082
I have a long history of complaining about guidelines and their seeming disregard for science and common sense. Therefore, when I sat down to read the most recent AHA guidelines on the evaluation and diagnosis of chest pain, I expected to be disappointed. Honestly, I was pleasantly surprised. It is still a very long way from perfect, but there is some reasonable new advice mixed in with all the nonsense.
The paper
Writing Committee Members, Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2021 Nov 30;78(22):e187-e285. doi: 10.1016/j.jacc.2021.07.053. Epub 2021 Oct 28. PMID: 34756653 [free full text]
Some of my key take-aways
This is a very long and dense publication. The majority of their recommendations are not practice changing (things like calling 911 if you have chest pain, or trying to get an ECG done within 10 minutes) and there is a lot that is irrelevant to emergency physicians. I am not going to attempt a comprehensive summary of the guidelines. Some people will want to read them all, and they are available for free online. I am just going to highlight a few points that I found interesting, potentially practice changing, or clearly wrong.
No stress tests in low risk patients
Testing Not Needed Routinely for Low-Risk Patients. For patients with acute or stable chest pain determined to be low risk, urgent diagnostic testing for suspected coronary artery disease is not needed.
Let me start with the big one: In low risk patients, testing for coronary artery disease is not needed. In other words, stop ordering so many damn stress tests. Specifically, they say that patients that are defined as low risk (either by a clinical decision pathway such as the HEART pathway or EDACS, or by negative high sensitivity troponins) do not need any further testing.
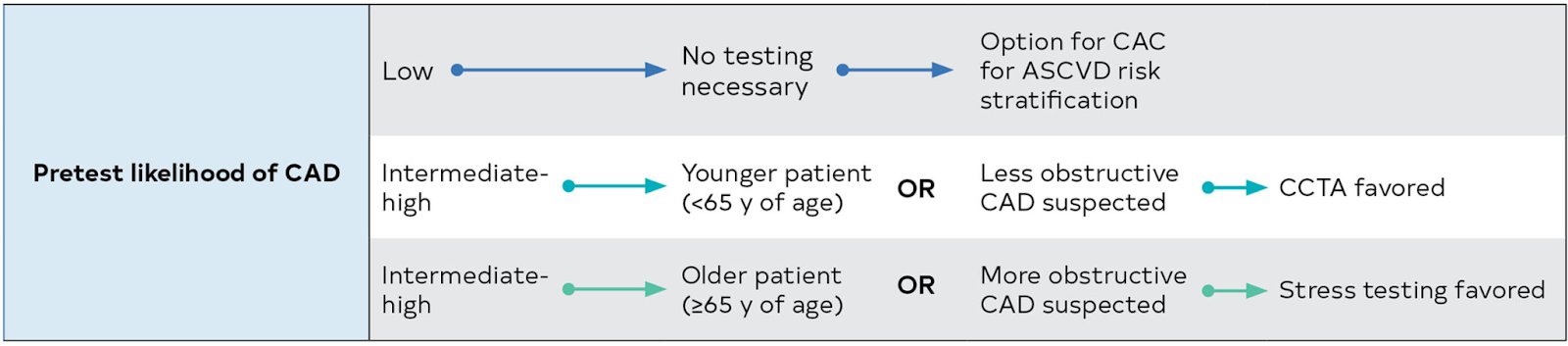
Of course, I don’t think they go far enough. They are still recommending CCTA in intermediate to high risk patients who are younger than 65 or less likely to have obstructive CAD, and stress testing in intermediate to high risk patients who are older than 65 or more likely to have obstructive CAD. Neither of these recommendations are supported by good evidence. Both cause net harm in patients. However, it is a big step forward for them to clearly state that the majority of chest pain patients should be discharged from the emergency department and do not need any further testing.
This is their definition of low-risk:
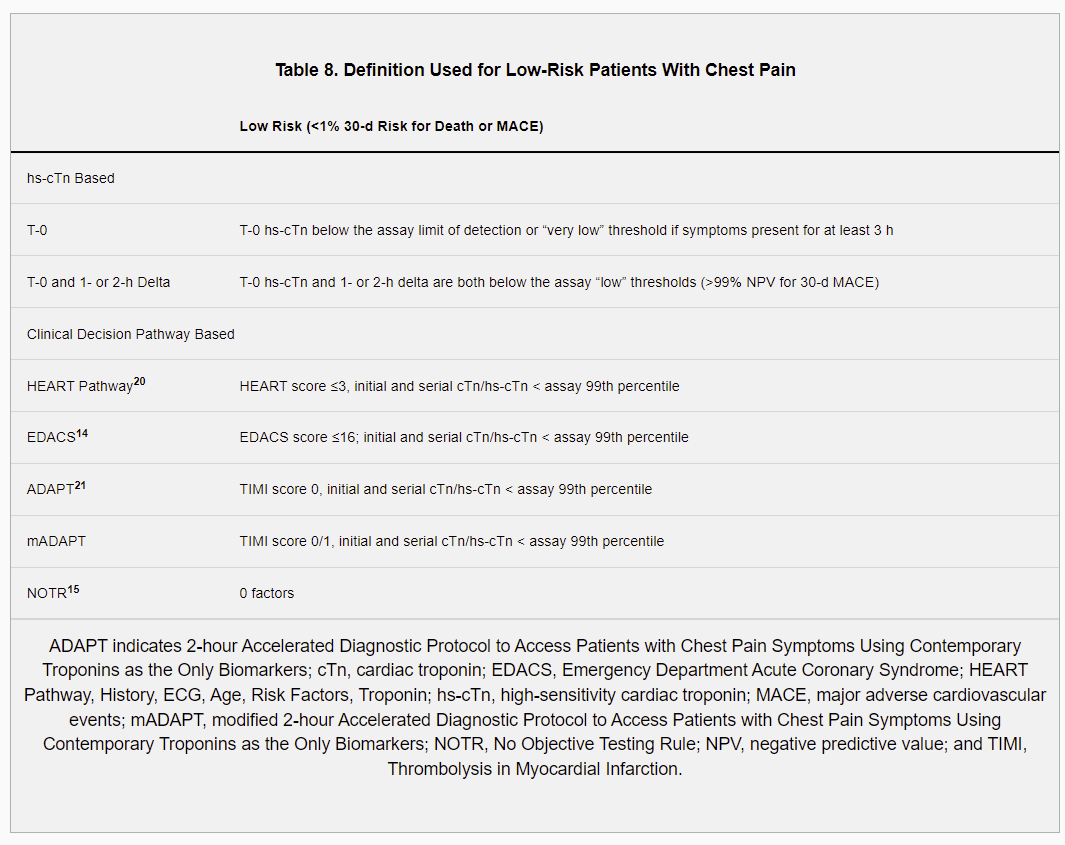
“Patients with acute chest pain and a 30-day risk of death or MACE <1% should be designated as low risk. … For this low-risk subset of ED patients who have chest pain, there is no evidence that stress testing or cardiac imaging within 30 days of the index ED visit improves their outcomes.” My only comment is that MACE is probably not clinically relevant, and the outcome we should be looking at is 30 day death and MI instead.
High sensitivity troponin is preferred
“In patients presenting with acute chest pain, high-sensitivity [troponin] is the preferred biomarker because it enables more accurate detection or exclusion of myocardial injury and increases diagnostic accuracy.”
This is one of those times where the guideline strays away from good science, but I don’t actually mind. (Even if I did, this ship has long sailed.) There is no evidence that HS-troponins improve patient outcomes. In fact, the two available RCTs comparing high sensitivity troponin to conventional troponin demonstrate no difference in clinical outcomes, such as incidence of missed MI or cardiovascular death in the year following presentation. (Shah 2018, Chew 2019) Additionally, high sensitivity troponins probably increase downstream invasive testing due to their lower specificity. In other words, they result in a net clinical harm to patients.
However, high sensitivity troponins allow for a much more rapid assessment of patients in the emergency department, which is a massive benefit for us and our patients alike. It is difficult to know how to balance the harm from increased testing with the benefit of improved efficiency. My bet is that, if we asked patients (and we should), the massive combined reduction in time spent in emergency departments would be an acceptable tradeoff for a slight increase in unnecessary invasive testing. EIther way, your hospital probably already decided what troponin to use, so this is basically a moot point.
Bottom line: Despite ignoring the available science, the guidance is probably still fine.
They like echo in intermediate risk patients
“For intermediate risk patients with acute chest pain, TTE is recommended as a rapid, bedside test to establish baseline ventricular and valvular function, evaluate for wall motion abnormalities, and to assess for pericardial effusion.”
“Point-of-care echocardiograms performed at the bedside by properly trained clinicians and technicians may be particularly useful.”
I don’t have a ton to say about this. In the right patient, I find echocardiography to be extremely valuable. I don’t think it should be used routinely, and honestly I have no idea why ‘intermediate risk for CAD’ would be the deciding factor in using ultrasound. However, ultrasound clearly has a role in the search for alternative pathologies (such as tamponade) or complications of AVS (such as valvular issues), as well as the evaluation of ACS (in looking for wall motion abnormalities). I just thought some people would be interested to know it is formally recommended.
They are stuck in the STEMI/NSTEMI world
Unless I missed something in these endless pages, they make absolutely no mention of the many ECG findings that we know to be STEMI equivalents. They just say, “patients with chest pain and new ST-elevation, ST depression, or new left bundle branch block on ECG should be treated according to STEMI and NSTE-ACS guidelines”, which is obviously wholly inadequate for a guideline describing the appropriate assessment of patients with chest pain.
For more on this, read the OMI manifesto.
Share the decision making
Share the Decision-Making. Clinically stable patients presenting with chest pain should be included in decision-making; information about risk of adverse events, radiation exposure, costs, and alternative options should be provided to facilitate the discussion.
“For patients with acute chest pain and suspected ACS who are deemed intermediate risk by a CDP [clinical decision pathway], shared decision-making between the physician and patient regarding the need for admission, for observation, discharge, or further evaluation in an outpatient setting is recommended for improving patient understanding and reducing low-value testing.”
I like that these guidelines emphasize shared decision making. They probably shouldn’t have to, as shared decision making is just good medicine, but sadly it is a part of good medicine where we frequently fail. There is mountains of evidence that patients are willing to take on more risk than we are. In other words, we often order tests to protect ourselves rather than to protect our patients. Shared decision making is an excellent way to protect ourselves while simultaneously providing care best aligned with the patient’s values. Shared decision making should really be part of every patient encounter, but it is still nice to see it referenced in these guidelines.
Forget “atypical”
First, they recognize that men and women with acute coronary syndrome are both equally likely to present with chest pain. The key difference is that women are more likely to present with accompanying symptoms, such as nausea and shortness of breath. I think there has been some confusion on this point, arising from the fact that we frequently say that women present ‘atypically’. However, it is still true that women are misdiagnosed more often than men, so they emphasize the need to ask about accompanying symptoms, and to recognize that those accompanying symptoms may point to ACS.
They also want us to stop using the word ‘atypical’ because it has two distinct and conflicting uses in the context of ACS. The way I use it is to describe on the chart that I think the patient’s pain is unlikely to be ACS (ie, it was brief, localized, and sharp). However, others use atypical to describe symptoms that rule in as angina, but aren’t crushing central exertional chest pressure.
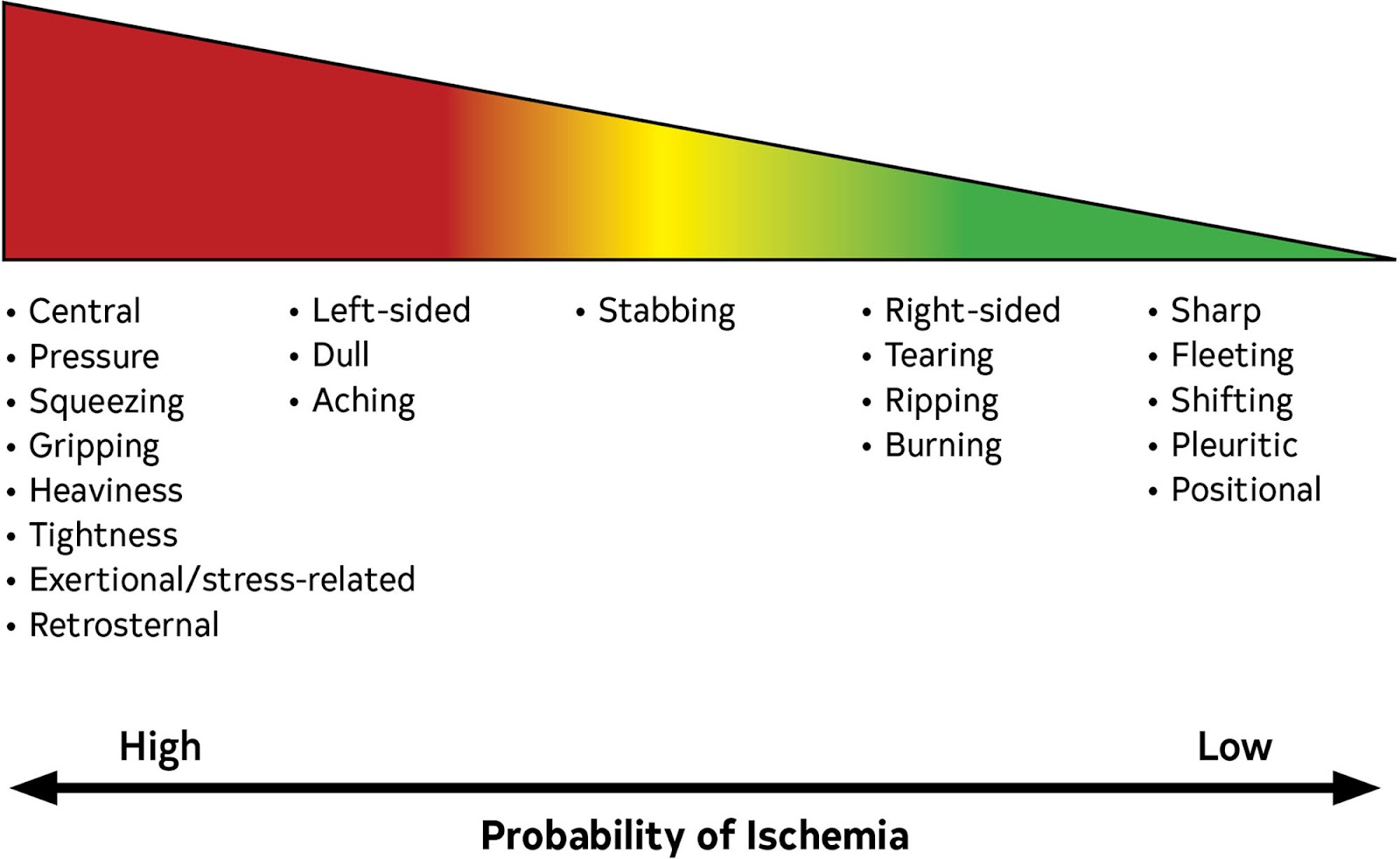
Instead, they prefer the terminology of “cardiac”, “possibly cardiac”, and “noncardiac”. I think this is probably a silly recommendation, and even contradicts some of the other statements that they make. Aside from trauma or shingles, where we wouldn’t even be referring to this guideline, when is chest pain definitively “noncardiac” by history alone? When is it definitely “cardiac”? And “possibly cardiac “ is so ridiculously vague that you are essentially saying nothing at all. There is a big difference between a patient with squeezing central chest pressure and a patient with a burning left sided chest pain. Both could end up being ACS, but the probability isn’t the same. I like the figure they provide that breaks down the probability of ischemia based on the description of the pain, but you will notice that they don’t even use their suggested terminology in their own image. For me, this suggested terminology will be a hard pass. (I might use the terminology from this image instead. Ie, this patient’s described pain is low probability for ischemia.)
Their text sometimes doesn’t match their recommendations: Should you get a chest x-ray?
Their official recommendation for chest x-rays is “in patients presenting with acute chest pain, a chest radiograph is useful to evaluate for other potential cardiac, pulmonary, and thoracic causes of symptoms.” To me (and I am sure lawyers), that sounds like a pretty strong recommendation for routine chest x-ray.
However, in the underlying text, they state, “chest radiographs often do not lead to a diagnosis that requires intervention, and their use should be guided by clinical suspicion.”
I honestly don’t have very strong opinions about chest x-ray for chest pain patients, but this second statement seems appropriate, and provides very important context for their main recommendation. Not everyone needs an x-ray.
They really like structured risk assessment and clinical decision pathways
They are strongly supportive of things like the HEART score and EDACs. That might sound relatively uncontroversial, but I think the evidence here is highly contextual and could potentially mislead.
I won’t get into the back and forth over whether the HEART score is accurate enough. What I really care about is whether these pathways actually improve clinical outcomes. I have not seen any evidence of improved outcomes in terms of mortality or missed MIs. There are a number of studies that demonstrate shorter ED stays and lower admission rates, but I think you need to be very cautious when interpreting those studies. Practice varies tremendously around the world, and so extrapolation may be inappropriate. These studies are often admitting patients that I wouldn’t have even referred to outpatient cardiology. In Canada, the vast majority of these patients are going home. When I consider the HEART pathway in my practice, it would result in a massive increase in admission to hospital, and I worry that is true of many environments outside of the United States. The vast majority of patients who have negative troponins and non-ischemic ECGs can be discharged home, no matter what their HEART score says.
Despite strongly recommending these tools, they do bury this comment deep in the “evidence gaps and future research” section: “Clinical risk stratification and decision tools will likely continue to grow in popularity because they are incorporated into electronic health records, but it would be useful to test them in large randomized trials to rigorously determine their benefit in terms of improved outcomes or lower costs before widespread implementation.” Sort of conflicts with their strong recommendation, but is actually the most important thing they say on the topic.
They give you a warranty period based on prior test results (which I don’t think is at all evidence based)
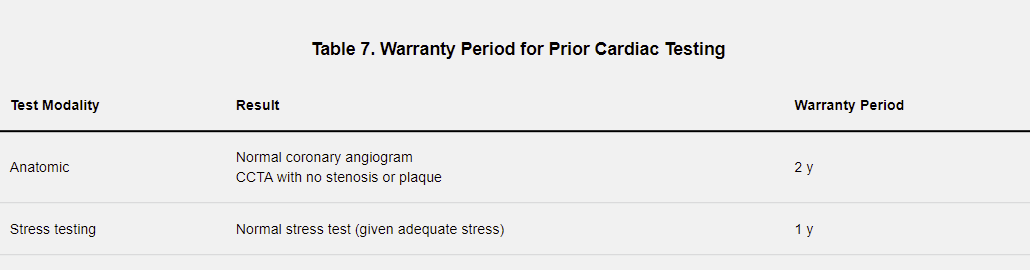
This goes counter to all teaching I have received in emergency medicine. I don’t really feel like doing a deep dive into this, but considering that the sensitivity of an exercise stress test is only 45%, and that many STEMIs develop from unstable plaques with less than 50% stenosis, there is just no way that these warranties can be correct.
Other FOAMed
CCTA doesn’t help: The evidence
The stress testing series:
- Introduction
- Part 1: How often to we miss MI?
- Part 2: Cardiovascular outcomes
- Part 3: The accuracy of stress tests
- Part 4: Revascularization and the value of stenting
- Conclusion: Putting it all together
References
Chew DP, Lambrakis K, Blyth A, Seshadri A, Edmonds MJR, Briffa T, Cullen LA, Quinn S, Karnon J, Chuang A, Nelson AJ, Wright D, Horsfall M, Morton E, French JK, Papendick C. A Randomized Trial of a 1-Hour Troponin T Protocol in Suspected Acute Coronary Syndromes: The Rapid Assessment of Possible Acute Coronary Syndrome in the Emergency Department With High-Sensitivity Troponin T Study (RAPID-TnT). Circulation. 2019 Nov 5;140(19):1543-1556. doi: 10.1161/CIRCULATIONAHA.119.042891. Epub 2019 Sep 3. Erratum in: Circulation. 2021 Jun 22;143(25):e1118. PMID: 31478763
Shah ASV, Anand A, Strachan FE, Ferry AV, Lee KK, Chapman AR, Sandeman D, Stables CL, Adamson PD, Andrews JPM, Anwar MS, Hung J, Moss AJ, O’Brien R, Berry C, Findlay I, Walker S, Cruickshank A, Reid A, Gray A, Collinson PO, Apple FS, McAllister DA, Maguire D, Fox KAA, Newby DE, Tuck C, Harkess R, Parker RA, Keerie C, Weir CJ, Mills NL; High-STEACS Investigators. High-sensitivity troponin in the evaluation of patients with suspected acute coronary syndrome: a stepped-wedge, cluster-randomised controlled trial. Lancet. 2018 Sep 15;392(10151):919-928. doi: 10.1016/S0140-6736(18)31923-8. Epub 2018 Aug 28. PMID: 30170853
Writing Committee Members, Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2021 Nov 30;78(22):e187-e285. doi: 10.1016/j.jacc.2021.07.053. Epub 2021 Oct 28. PMID: 34756653 [free full text]