
Morgenstern, J. Monkeypox, First10EM, May 19, 2022. Available at:
https://doi.org/10.51684/FIRS.128007
In the Rapid Review series, I briefly review the key points of a clinical review paper (or two). With reports of monkeypox cases arising around the world (Canada, United Kingdom, Europe, and United States), I figured we had better do a quick review of the disease, because it was either never taught in my medical school curriculum, or I missed that day.
The papers:
Di Giulio DB, Eckburg PB. Human monkeypox: an emerging zoonosis. Lancet Infect Dis. 2004 Jan;4(1):15-25. doi: 10.1016/s1473-3099(03)00856-9. Erratum in: Lancet Infect Dis. 2004 Apr;4(4):251. PMID: 14720564
McCollum AM, Damon IK. Human monkeypox. Clin Infect Dis. 2014 Jan;58(2):260-7. doi: 10.1093/cid/cit703. Epub 2013 Oct 24. Erratum in: Clin Infect Dis. 2014 Jun;58(12):1792. PMID: 24158414
What is it?
Human monkeypox is a viral zoonosis endemic to central and western Africa. It is in the same family of viruses as smallpox and chickenpox, and is generally considered the most important orthopoxvirus since the eradication of smallpox.
How does it present?
Monkeypox presents very similarly to smallpox (although that is not going to help any modern doctor make the diagnosis) or chickenpox. There is a characteristic 2 day prodrome of fever, malaise, myalgias, and/or headaches. 90% of patients develop lymphadenopathy.
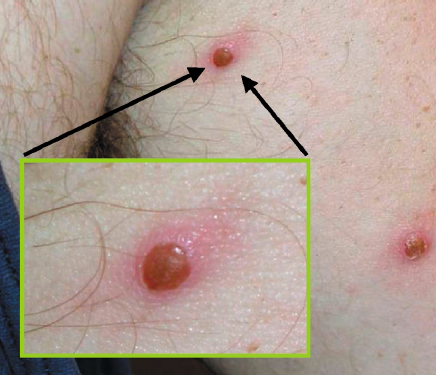
The typical rash starts as maculopapular lesions 2-5 mm in diameter, and tends to spread in a centrifugal pattern (from core out). These lesion then progress through papular, vesicular, and pustular phases, before crusting over and leaving dyspigmented scars. The evolution of the lesions is variable, with some patients having all lesions evolve at the same time (monomorphic, like smallpox), while other patients have the more classic chickenpox pattern (pleiomorphic).
When originally described, it was thought to look mostly like smallpox, but over time more cases have been identified that mimic chickenpox. In fact, in one study out of Africa, 3% of patients diagnosed with chickenpox actually had monkeypox on serologic testing, as well as 7% of patients with ‘atypical chickenpox’, and 6% of patients with rash of unknown cause. (Jezek 1988) This particularly bothers me, as I have seen a lot of chickenpox in my career, often in travelers, and have never once considered testing for monkeypox. Multiply that experience thousands of times over, and you can bet this disease has been missed many times.
What does this rash look like?
Yeah, I know my description may not have been that helpful. Here are some images from the papers:






How is it spread?
Thankfully, when compared to smallpox, monkeypox has a much lower rate of transmission from human to human, with a secondary attack rate of approximately 5-10%. There have been numerous outbreaks in the past, and all have been self-limited with just basic infection control measures. The exact mechanism of spread is unknown, and many resources list droplet/contact as the primary mechanism of spread, but most also acknowledge the possibility of airborne spread. The CDC says that patients should be placed in a negative pressure room, and airborne precautions should be used.
How is it diagnosed?
Laboratory diagnosis is important, as the clinical features can overlap significantly with chickenpox (and smallpox, but that would be a very bad day). Some of these articles contain some specific information about deroofing and transporting scabs for testing. Personally, I would talk to someone in the infectious disease realm, and allow them to guide the appropriate testing.
Is there a vaccine?
Smallpox vaccination appears to provide reasonable (approximately 85%) protection against monkeypox, and the CDC recomends pre-exposure vaccination for health-care workers who are investigating or caring for patients with suspected monkeypox and who have no contraindications to vaccination.
How is it treated?
There are no proven treatments, and like most viral illnesses, the management is primarily supportive.
Post-exposure vaccination was effective against smallpox, and so the CDC extrapolates to recommend giving the smallpox vaccine within 4 days from the date of exposure in order to prevent monkeypox. Giving the smallpox vaccine between 4 and 14 days post-exposure may not prevent the disease, but may reduce symptoms.
Cidofovir is a broad-spectrum antiviral with in vitro activity against smallpox, but there is absolutely no clinical data to support its use, and it has substantial toxicity.
Perhaps the most important management step in the emergency department is reporting the case to public health and getting guidance from them.
What are the complications?
About 20% of patients will develop secondary skin infections, and 10% of patients will develop pneumonitis. Ocular complications and encephalitis are also possible.
What is the prognosis?
The disease is probably significantly under-reported, and so mortality may be overestimated, but during the most intensive investigations in Africa, the mortality rate was 10-20%. However, there was an outbreak in 2003 in the United States in which 81 patients were reported, and there were no deaths.
Some history
Unlike our long history with smallpox, the first case of human monkeypox was only described in 1970, in the Democratic Republic of the Congo. (It was only recognized after the eradication of smallpox. Prior to that, it was probably just confused with smallpox).
Some trivia
Despite the name, the largest zoonotic reservoir of disease is probably in rodents.
Other FOAMed
Monkeypox info from the UK Health Security Agency
References
Di Giulio DB, Eckburg PB. Human monkeypox: an emerging zoonosis. Lancet Infect Dis. 2004 Jan;4(1):15-25. doi: 10.1016/s1473-3099(03)00856-9. Erratum in: Lancet Infect Dis. 2004 Apr;4(4):251. PMID: 14720564
Jezek Z, Szczeniowski M, Paluku KM, Mutombo M, Grab B. Human monkeypox: confusion with chickenpox. Acta Trop. 1988 Dec;45(4):297-307. PMID: 2907258
McCollum AM, Damon IK. Human monkeypox. Clin Infect Dis. 2014 Jan;58(2):260-7. doi: 10.1093/cid/cit703. Epub 2013 Oct 24. Erratum in: Clin Infect Dis. 2014 Jun;58(12):1792. PMID: 24158414




5 thoughts on “Monkeypox”
Thanks, very informative. I am at a refugee camp on the Ukranian boarder. We have a large outbreak of chicken pox. This makes me wonder.