
Morgenstern, J. The evidence suggests N95s are better than surgical masks, First10EM, November 1, 2021. Available at:
https://doi.org/10.51684/FIRS.118213
For some reason, masks seem to provoke very strong opinions in medicine. Despite being one of the closest things we have to parachutes – devices so simple and obvious that RCT evidence may not even be needed – people lament the lack of evidence, and mistakenly translate the paucity of evidence into paucity of effect. When covering this topic in the past (here or here), I noted that although the evidence is far from conclusive, it suggested a possible benefit from N95s in imperfect and under-powered studies. There is a new study making headlines that suggests a 100% decrease in hospital acquired COVID infections with routine use of N99 (or FFP3) masks, so I thought it would be a good time for a deep dive review of this literature. Interestingly, despite being told repeatedly throughout this pandemic that there is no evidence for N95s, there is 1 RCT that shows that routine use of an N95 decreases respiratory illnesses in healthcare workers, and the bulk of the evidence fits with that hypothesis. More importantly, as N95s have always been considered the standard, there is no convincing evidence that surgical masks are an equivalent or safe alternative.
Basic Physiology
We need to be cautious of physiologic reasoning in medicine, as it has led us astray many times in the past. However, it is a reasonable starting point for evidence based medicine discussions, and may be our only option when science is limited.
When it comes to personal protective equipment against respiratory viruses, the choice has always been based on whether the virus is spread in droplets or aerosols. (Although this distinction is almost certainly overly simplistic.) We use N95s (or better) when airborne or aerosol transmission is suspected.
At this point, we definitely know that COVID-19 is at least occasionally transmitted through aerosols or the airborne route. Everyone agrees on that fact. There are some in the medical community who continue to argue that despite some airborne spread, the bulk of spread is through droplets. However, I have never seen this argument backed up with any science, and I think the science very clearly demonstrates that COVID-19 is predominantly spread by the airborne route. My main post on this science is here. (There is also good evidence that other respiratory viruses we encounter, such as influenza, are also airborne.) However, even the most intractable stance acknowledges that COVID is spread through aerosols at least some of the time, and therefore the baseline position would be that N95s are the appropriate PPE unless there is strong evidence that an alternative is equally safe.
Some Systematic Reviews
Anyone who follows this blog, or our Journal Jam podcasts, knows that systematic reviews can easily lead us astray. They tend to glaze over biases in individual trials, and simply piling more bad data together doesn’t make the data any better; it just makes a bigger pile. However, systematic reviews are a great place to start if you want an overview of a topic (and want to let other people do some of the hard work of sifting the PubMed). Let’s start with a few of the systematic reviews on the topic.
Smith JD, MacDougall CC, Johnstone J, Copes RA, Schwartz B, Garber GE. Effectiveness of N95 respirators versus surgical masks in protecting healthcare workers from acute respiratory infection: a systematic review and meta-analysis. CMAJ : Canadian Medical Association journal. 188(8):567-74. 2016. PMID: 26952529 [free full text]
This was the first publication I ever covered on N95s, and back in 2016 I didn’t seem very excited about the topic. It is a meta-analysis of 6 studies (3 RCTs, 1 cohort study, and 2 case-control studies) comparing respirators to surgical masks in the prevention of influenza-like illnesses. None of the results were statistically significant. There was no change in laboratory confirmed infection (OR 0.89 95% CI 0.64-1.24). There was no change in influenza-like illness (OR 0.51 95% CI 019-1.41). And there was no change in workplace absenteeism (OR 0.92 95% CI 0.57-1.50).
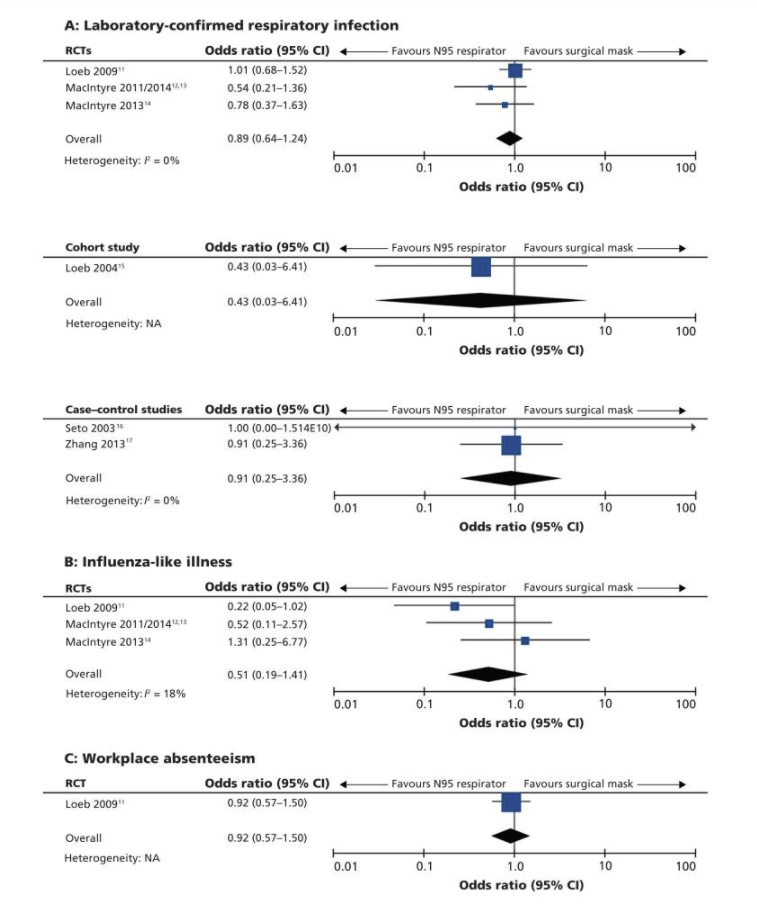
As I said at the outset, just looking at the meta-analysis hides many of the important details in these trials. How good was compliance with masks? Was the other PPE controlled? How prevalent were respiratory infections? (You can’t possibly show a difference between groups if there are too few infections overall.) How were infections defined? What were the vaccination rates among staff? What wards were involved, and what high risk activities might have taken place? (Although I firmly believe that “aerosol generating procedure” is a scientifically inaccurate and overall harmful concept.)
In addition to these details, we have to consider the statistical accuracy of the numbers presented. The 95% confidence intervals in this meta-analysis are huge, but the point estimates all favour the use of N95s. The magnitude of benefit is potentially huge, with N95s decreasing the overall rate of influenza-like illness by almost half. That would clearly be clinically significant, if the results are true. Thus, these trials are simply too under-powered to allow us to form clear conclusions, but they support a clear hypothesis that N95s provide better protection than surgical masks. (Or, framed another way, if N95s are considered the current standard, this data could certainly not be used to demonstrate the equivalence or non-inferiority of surgical masks.)
Long Y, Hu T, Liu L, Chen R, Guo Q, Yang L, Cheng Y, Huang J, Du L. Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta-analysis. J Evid Based Med. 2020 May;13(2):93-101. doi: 10.1111/jebm.12381. Epub 2020 Mar 13. PMID: 32167245
This is another systematic review and meta-analysis comparing N95 respirators to surgical masks against influenza. This review found a total of six RCTs involving 9,171 participants, and the results are very similar to the last one. There were no statistically significant differences in preventing laboratory-confirmed influenza (RR = 1.09, 95% CI 0.92-1.28, P > .05), laboratory-confirmed respiratory viral infections (RR = 0.89, 95% CI 0.70-1.11), laboratory-confirmed respiratory infection (RR = 0.74, 95% CI 0.42-1.29), or influenza like illness (RR = 0.61, 95% CI 0.33-1.14) using N95 respirators compared to surgical masks. There was a decrease in laboratory-confirmed bacterial colonization with N95 use (RR = 0.58, 95% CI 0.43-0.78), but the importance of that finding is unclear to me.
Once again, the confidence intervals are huge, and the point estimates are generally on the side of N95s being better. 9,000 people in a meta-analysis sounds like a lot, but you have to remember that a trial’s power comes from the number of events, not the number of people. Most healthcare workers don’t get sick in the average flu season, so you will need a large number of participants in order to show a benefit. (This also tells us that the magnitude of benefit will be small, which should be obvious, as most of us haven’t been sick throughout the COVID pandemic. However, even a small magnitude benefit could be tremendously important when facing a deadly pandemic.)
Jefferson T, Del Mar C, Dooley L, Ferroni E, Al-Ansary LA, Bawazeer GA, van Driel ML, Foxlee R, Rivetti A. Physical interventions to interrupt or reduce the spread of respiratory viruses: systematic review. BMJ. 2009 Sep 21;339:b3675. doi: 10.1136/bmj.b3675. PMID: 19773323
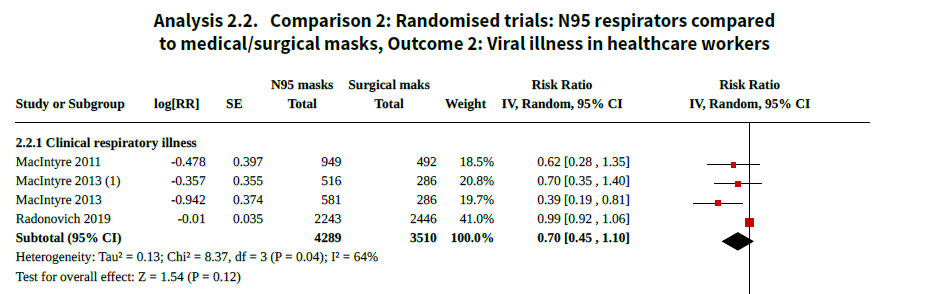
This is the Cochrane review, so it gets cited a lot, but it really doesn’t add anything to the two systematic reviews we have already looked at. They conclude that “there is uncertainty over the effect of N95/P2 respirators when compared with medical/surgical masks on the outcomes of clinical respiratory illness (RR 0.70, 95% CI 0.45 to 1.10; very low-certainty evidence; 3 trials; 7779 participants) and ILI (RR 0.82, 95% CI 0.66 to 1.03; low-certainty evidence; 5 trials; 8407 participants). The evidence is limited by imprecision and heterogeneity for these subjective outcomes.” I agree. There is definitely uncertainty, with wide confidence intervals, but the widest parts of those confidence intervals fall on the side of benefit from N95s.
They add “the use of a N95/P2 respirator compared to a medical/surgical mask probably makes little or no difference for the objective and more precise outcome of laboratory-confirmed influenza infection (RR 1.10, 95% CI 0.90 to 1.34; moderate-certainty evidence; 5 trials; 8407 participants).” I will go through all the trials below, but I think the contention that laboratory confirmed influenza is a better outcome is entirely wrong. When you read these studies, it turns out that the vast majority of “lab confirmed influenza” was a change in serology in people who were entirely asymptomatic. That is not a meaningful or objective outcome. I have no idea what that even means. The people never got sick. There was just a change in their blood work. None of us are getting this blood work routinely, and it is certainly not the reason that we are wearing masks.
It is also worth noting that these authors make a fairly fundamental mistake. As we will discuss below, MacIntrye 2013 has 2 different groups that wore N95s. One group wore N95s routinely. The other group wore surgical masks routinely, and only added N95s for high risk procedures. When comparing N95s to surgical masks, this latter group should clearly be considered in the surgical mask group, because they were in surgical masks the vast majority of the time, but these authors include it as an N95 group. This is particularly interesting, but this was a positive study, in that the group that wore N95s routinely had significantly fewer infections than the surgical mask group. Adding a group that wore surgical masks almost all the time and claiming that that is evidence against N95s is ridiculous, and clearly biases the results against N95s. (It probably wouldn’t ultimately affect their math, because Radonovich 2019 gets weighted as 41% of the meta-analysis. However, that also introduces bias, as Radvonovich only required masks to be worn within 6 feet of patients, which is clearly ridiculous if these diseases are airborne, and negates the purpose of the N95.)
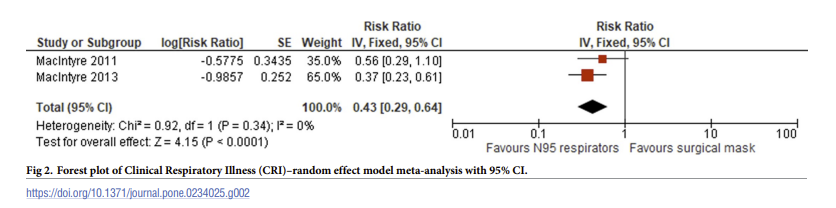
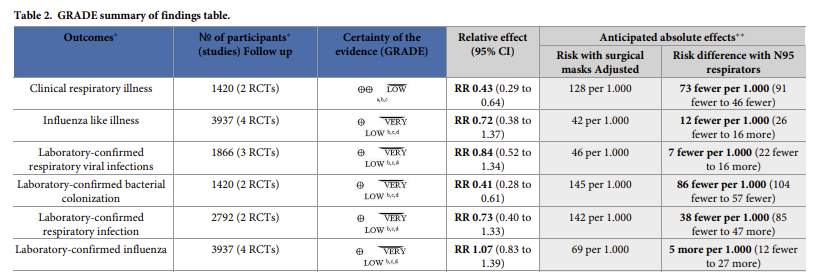
Iannone P, Castellini G, Coclite D, Napoletano A, Fauci AJ, Iacorossi L, D’Angelo D, Renzi C, La Torre G, Mastroianni CM, Gianola S. The need of health policy perspective to protect Healthcare Workers during COVID-19 pandemic. A GRADE rapid review on the N95 respirators effectiveness. PLoS One. 2020 Jun 3;15(6):e0234025. doi: 10.1371/journal.pone.0234025. PMID: 3249204
I am including 1 more meta-analysis, not because it adds any more data, but because I think it is important to know that there is at least 1 published meta-analysis that concludes that there is a statistically significant benefit of wearing N95 respirators over surgical masks
There are many more systematic reviews we could cover. There are more systematic reviews than there are studies. However, there is nothing to be gained by looking at more summaries of this data. Let’s just go directly to the source and look at the RCTs.
The RCTs
Loeb M, Dafoe N, Mahony J, John M, Sarabia A, Glavin V, Webby R, Smieja M, Earn DJ, Chong S, Webb A, Walter SD. Surgical mask vs N95 respirator for preventing influenza among health care workers: a randomized trial. JAMA. 2009 Nov 4;302(17):1865-71. doi: 10.1001/jama.2009.1466. Epub 2009 Oct 1. PMID: 19797474
This is a non-inferiority RCT, in which 446 nurses in emergency departments, medical units, and pediatric units from 8 hospitals were randomized to either wear an N95 respirator or a surgical mask when caring for patients with febrile respiratory illnesses. Nurses wore their assigned masks during ‘aerosol generating procedures’. They did not wear masks if they were not directly caring for the patient, or more than 1 meter from the patient.
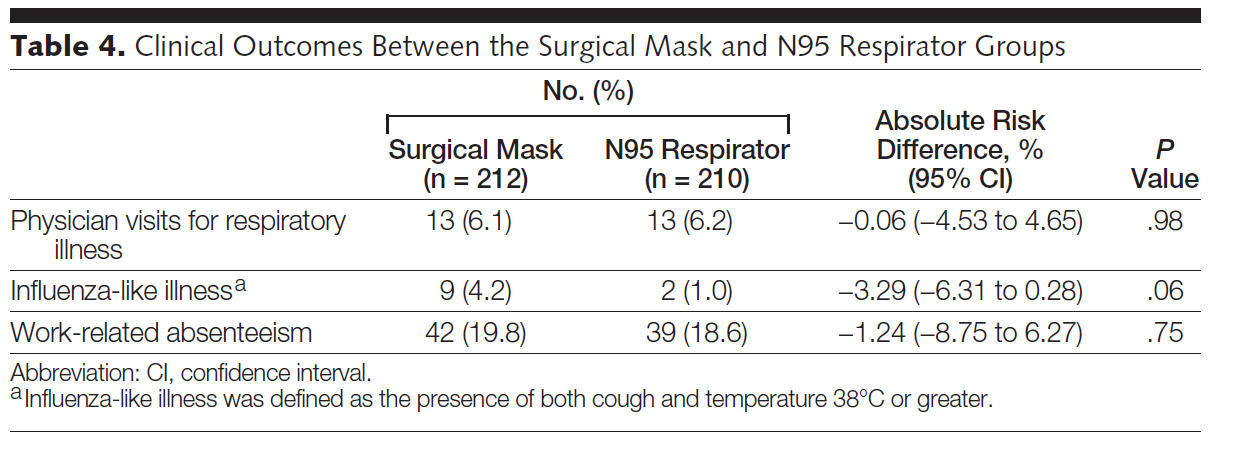
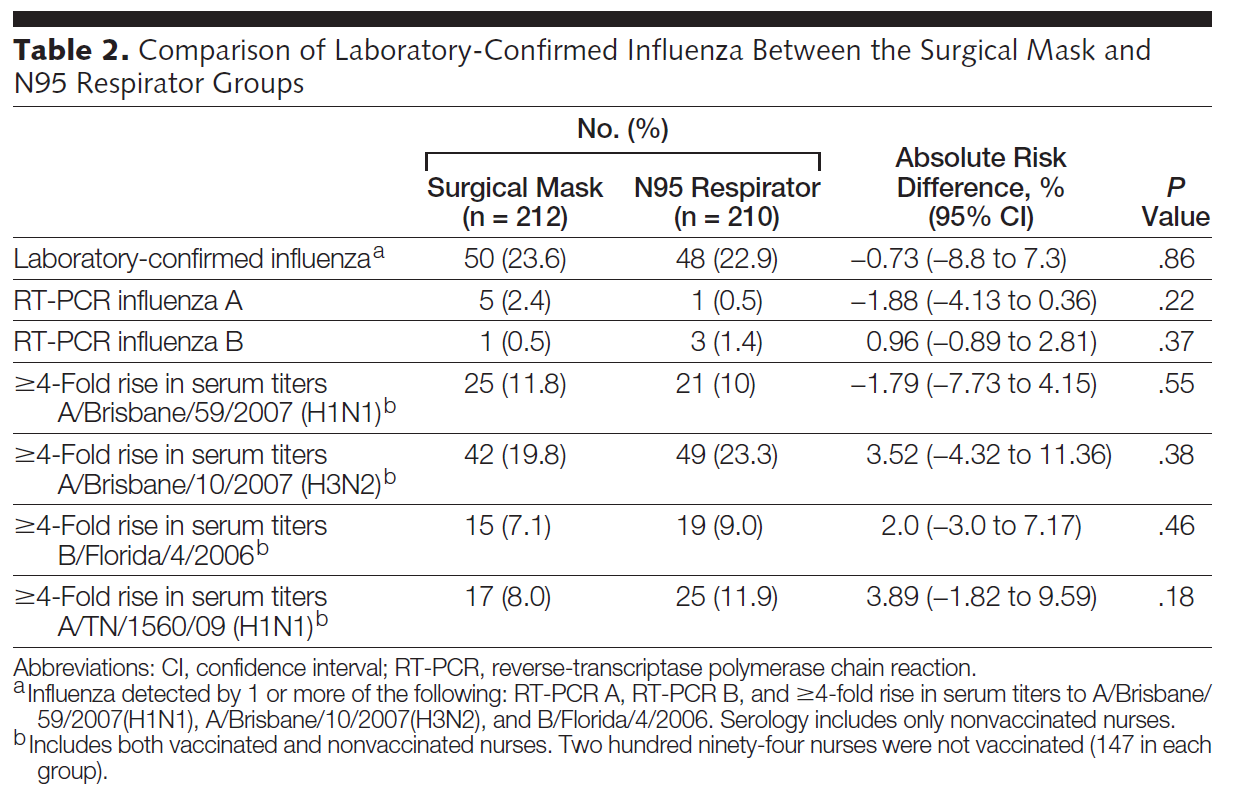
The primary outcome was unchanged, and met with their definition of non-inferiority (discussed more below). 23.6% of the surgical mask group and 22.9% of the N95 group had ‘lab confirmed influenza’ (ARR -0.7%, 95% CI -8.8% to 7.3%). However, almost none of these individuals were actually sick. Influenza-like illness occurred in 4.2% of the surgical mask group and 1% of the N95 group (ARR -3.2%, 95% CI -6.3% to 0.28%, p=0.06), which makes it look a lot like N95s could actually be better and this study was just underpowered to show the difference.
This is a well done study with proper randomization, a clearly defined primary outcome, and registration of clinicaltrials.gov. However, the one piece of information I really want to see in the trial registration – the non-inferiority margin – seems to be absent. A non-inferiority trial really hinges on this preset margin, and it would be good to know that the 9% margin was prespecified. (It would also be good to know why a 9% absolute increase in influenza infections was considered acceptable.)
The rates of influenza in this study were very high when compared to other studies, and may represent a flaw in the way that they defined laboratory confirmed influenza. They included both PCR confirmed cases and serological changes. PCR testing was only done with symptoms, but serology was done on everyone. The vast majority of ‘confirmed influenza’ in this trial was actually asymptomatic changes in serology numbers. Only 2.9% of the surgical mask group and 1.9% of the N95 group had symptoms plus a positive PCR test, which probably represents the true influenza rate. Similarly, influenza-like illness occurred in 4.2% of the surgical mask group and 1% of the N95 group. If non-inferiority had been calculated based on these small numbers, it seems very unlikely that you could demonstrate statistical non-inferiority of surgical masks. (There are many ways to undermine non-inferiority trials, but inflating the numbers in both groups is one way to do it.)
There is a bit of a mathematical red flag with this study as well. They say that they only included the serologic results from unvaccinated participants (because vaccination would confound the serology). If that is true, based on my calculations, the rate of lab confirmed influenza is actually 70% (of eligible participants) in the surgical mask group and 80% in the N95 group, which is just unbelievable, especially when only 2-3% were positive by PCR.
However, the biggest flaw with this study is that masks were only worn when nurses were in direct contact with patients. First, it does not extrapolate well to current practice. Second, it ignores the role of airborne spread, and therefore biases in favour of surgical masks. Surgical masks are reasonable if microbes are only spread through droplets. However, if there is an airborne component, the N95 would be favoured. However, the advantage of the N95 against airborne spread is negated, or at least greatly reduced, if the mask is removed as soon as one steps away from the patient. Medical wards and emergency departments are cramped environments, with nursing stations often found in close proximity to and surrounded by patient rooms. If influenza is airborne (which it almost certainly is) transmission will occur even when nurses aren’t providing direct care to patients, thus undermining the potential value of the N95. In this study, they specifically say that masks were only required if within 1 meter of a patient.
Bottom line: This trial concludes that surgical masks are non-inferior to N95s against influenza. However, their outcome of choice is very questionable, and masks were only worn within 1 meter of patients, biasing the results against the airborne protection provided by N95s.
MacIntyre CR, Cauchemez S, Dwyer DE, Seale H, Cheung P, Browne G, Fasher M, Wood J, Gao Z, Booy R, Ferguson N. Face mask use and control of respiratory virus transmission in households. Emerg Infect Dis. 2009 Feb;15(2):233-41. doi: 10.3201/eid1502.081167. PMID: 19193267
This study isn’t really applicable, as it looks at the use of masks worn at home by parents of sick children. However, it is included in some meta-analyses as a negative trial, so I will mention it. They randomized families to either use a surgical mask, a P2 mask (sort of like an unfitted N95), or no mask. Masks were supposed to be worn at all times when in the same room as the sick child, but the downfall of this study is that compliance was about 40% on day 1 of the study, and fell to about 25% by day 5. In other words, this study really just compared 3 groups of households who didn’t wear masks the vast majority of the time. Thus, it is not surprising that the rates of influenza-like illness were identical in the three groups. (To me, this study highlights the potential problems with simply combining data in meta-analyses. This study was included in the Long 2020 meta-analyses, but given its short-comings, that seems ridiculous.)
Bottom line: When masks are not worn the majority of the time, there is no difference between surgical masks, respirators, and no masks at all.
MacIntyre CR, Wang Q, Cauchemez S, Seale H, Dwyer DE, Yang P, Shi W, Gao Z, Pang X, Zhang Y, Wang X, Duan W, Rahman B, Ferguson N. A cluster randomized clinical trial comparing fit-tested and non-fit-tested N95 respirators to medical masks to prevent respiratory virus infection in health care workers. Influenza Other Respir Viruses. 2011 May;5(3):170-9. doi: 10.1111/j.1750-2659.2011.00198.x. Epub 2011 Jan 27. PMID: 21477136
This is a cluster randomized trial, in which all staff on a ward were randomized to either wearing N95 respirators or surgical masks for the course of a single influenza season. There were 2 N95 groups: fit-tested and non-fit-tested.
Interestingly, they wanted to include a proper no-mask control group, but this was considered unethical in China (but would have been standard operating procedure everywhere in Canada at the time.) Instead of randomizing patients to no-mask, they used a convenience sample control group of 9 hospitals in the same city where masks weren’t being worn. (The fact that masks weren’t being worn routinely sort of suggests the ‘unethical’ argument was incorrect, and randomization to no masks should have been allowed.)
They randomized 1441 nurses and doctors from emergency departments and respiratory wards in 15 hospitals in Beijing, and included another 481 nurses and doctors in the no mask control arm. The outcomes are somewhat difficult to summarize, because they looked at multiple different outcomes, making multiple different comparisons. The numbers were pretty small, and many of the comparisons were not statistically significant. However, figure 2 demonstrates a pretty clear hierarchy: N95 was better than surgical mask, which was better than no mask at all. (Some, but not all, of these comparisons were statistically significant.)
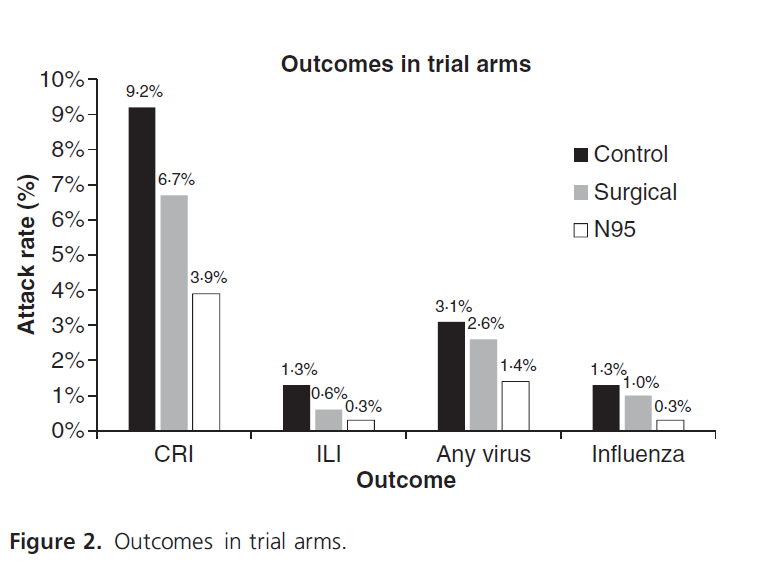
Compared directly with surgical masks, the N95 was not statistically superior in any comparison, but it had consistently lower rates of infection. They powered the study assuming a 12% attack rate in the medical mask arm and a 5% attack rate in the N95 arm. They only saw 7% and 4% respectively, so the trial was underpowered. When comparing N95s to no mask, 2 of the 4 outcomes in the trial were statistically significant. Comparing surgical masks to no masks, there were no statistically significant outcomes. Strangely, non-fit-tested N95s performed better than fit-tested.
This is clearly not a perfect trial. They had to include a convenience sample as their control group, and they ended up under-powered based on their power calculation. Adherence was reasonable, but not perfect (around 75%), and the masks were only worn for a total of about 5 hours per shift.
Although there were some statistically significant outcomes, I would not count this as a ‘positive’ trial, because there were so many comparisons being made without adequate adjustment. However, there is a very clear trend that suggests N95s could be superior to surgical masks which could be superior to nothing at all. Considering that this is exactly what we would expect based on basic physiology, the hypothesis is believable. How one approaches this clinically while waiting for follow-up research depends on a number of baseline assumptions. If you start from the position of the precautionary principle, assuming N95s are superior and should be considered the standard, there is clearly nothing here to suggest that surgical masks are a safe alternative. If you consider surgical masks the standard, this data doesn’t prove N95s are better, but it is suggestive enough that it could be worth using them while awaiting more data. (It is certainly stronger evidence than we have for many current medical treatments.) I don’t think this would have been enough to convince me to wear an N95 routinely during flu season, had I been aware of this data, but I think it is enough to suggest routine use of N95s during COVID, as we wait for definitive trials.
Bottom line: This is an under-powered and imperfect cluster RCT that does not definitively demonstrate a difference between N95s, surgical masks, and no mask at all, but supports the hypothesis that masks are helpful and N95s could offer the best protection.
MacIntyre CR, Wang Q, Seale H, Yang P, Shi W, Gao Z, Rahman B, Zhang Y, Wang X, Newall AT, Heywood A, Dwyer DE. A randomized clinical trial of three options for N95 respirators and medical masks in health workers. Am J Respir Crit Care Med. 2013 May 1;187(9):960-6. doi: 10.1164/rccm.201207-1164OC. PMID: 23413265
This is a cluster randomized trial, in which wards were randomized to one of three policies for a single winter season: 1) surgical masks at all times on shift, 2) N95s at all times on shift, 3) surgical mask at all times, with an N95 used during high risk or ‘aerosol generating’ procedures. They included 1669 nurses from 68 emergency departments and respiratory wards in 19 hospitals in Beijing. Although they did fit test participants for N95s, it sounds like they only provided a single type of N95 (3M 1860) and subjects who failed the fit test were still included in the N95 arm as part of the intention to treat analysis. They don’t provide details on how many people failed the fit test, but with only a single option, this could be a big source of bias against the N95s, as a significant number of participants may have been using a respirator that was known not to fit. There were multiple ‘primary’ outcomes, which is a methodologic faux pas.
Clinical respiratory illnesses were highest in the medical mask arm (17%), intermediate in the targeted N95 group (12%), and lowest in the routine N95 group (7%), with a p value <0.05. Although laboratory confirmed influenza was one of their outcomes, there were only 6 cases in the entire trial, which is clearly not enough to draw any conclusions. There were also too few laboratory confirmed viral illnesses to make a valid comparison, although it follows a similar pattern, with the most occurring in the surgical mask group and the least occurring in the N95 group. N95s resulted in a decrease in the detection of bacterial pathogens (primarily S. pneumoniae) in patients with clinical respiratory illnesses (15% with surgical masks, 10% with targeted N95s, and 6% with routine N95s, p=0.02).

Compliance was lower with routine N95 use (57% versus 66% with surgical masks and 82% with targeted use). This is a topic that comes up all the time. People find N95s uncomfortable and don’t wear them consistently. This is one reason IPAC gives for suggesting against N95s. However, the fact that this trial was able to demonstrate a significant benefit from routine N95 use, despite the fact that staff was wearing them less than 60% of the time suggests that N95s are even more protective than these numbers suggest. I imagine that people would have been more compliant with N95s when facing a novel deadly respiratory virus, but because IPAC has consistently denied their value, we will never know.
In addition to the low compliance rate, this trial included participants who had failed the N95 fit test. They provided some people (we don’t know how many) with equipment they didn’t expect to work, and they were still able to show a benefit! This could mean that there is an even bigger benefit among those properly fit, but it was washed out by those with poor fits. Or it could mean that fit testing is less important than we currently believe. (If I showed up at the hospital and they didn’t have a mask I was fit tested to, I would definitely use another N95, rather than just using a surgical mask, which is what I have heard some IPAC people suggest.)
In my mind, the most important part of this trial is that they compared against the current standard. It wasn’t just N95 versus surgical masks. The group that used N95s only during high risk procedures clearly replicates the advice most of us are getting from IPAC, and the routine use of N95s was better than this selective use. (There was a significant reduction in clinical respiratory illness – HR 0.56, 95% CI 0.32-0.98). This suggests that the current IPAC advice in many institutions is wrong.
Bottom line: This trial, although imperfect, shows a statistically significant decrease in clinical respiratory illness with the routine use of N95 masks as compared to routine surgical use, or the current ‘standard’ of using N95s only during high risk procedures.
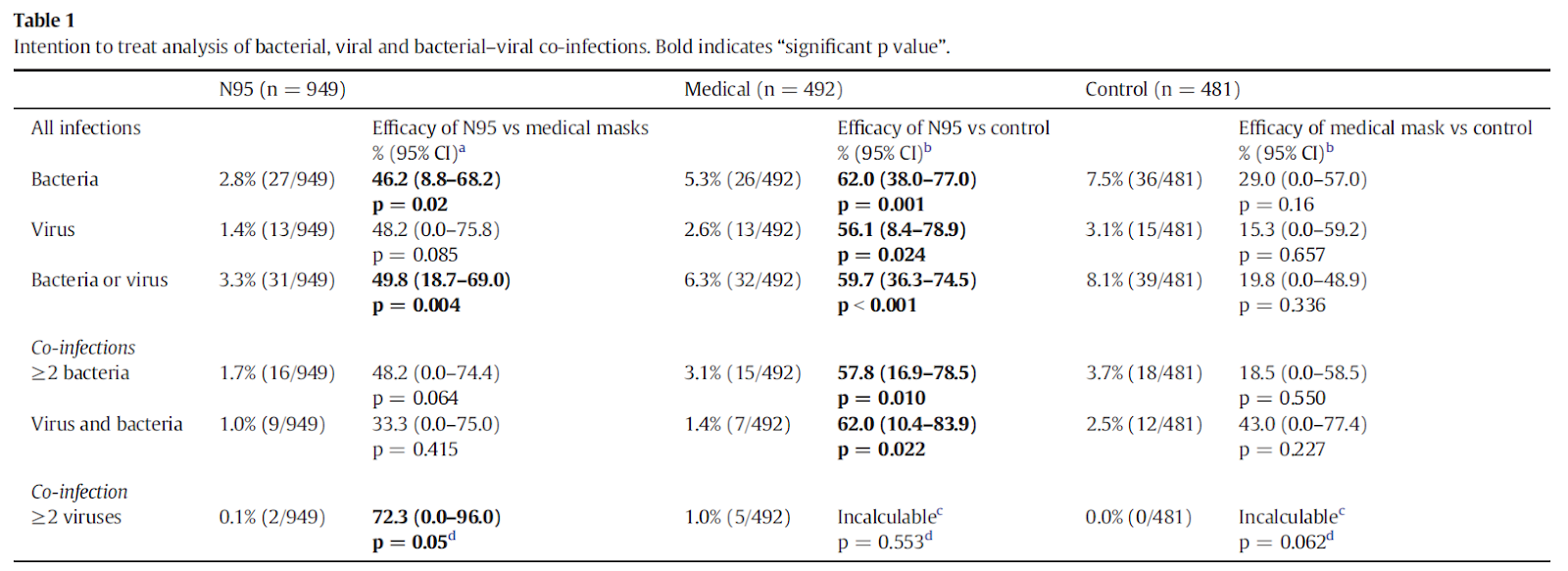
MacIntyre CR, Wang Q, Rahman B, Seale H, Ridda I, Gao Z, Yang P, Shi W, Pang X, Zhang Y, Moa A, Dwyer DE. Efficacy of face masks and respirators in preventing upper respiratory tract bacterial colonization and co-infection in hospital healthcare workers. Prev Med. 2014 May;62:1-7. doi: 10.1016/j.ypmed.2014.01.015. Epub 2014 Jan 25. PMID: 24472436
This is not an original publication. It is a second publication based on the same data set at the 2011 MacIntyre study. As such, it really should be treated as a secondary outcome, and shouldn’t be given its own entry into a meta-analysis. They wanted to emphasize that masks are not just protective against viruses, but also against bacteria. It is definitely interesting that N95s look better than surgical masks against bacteria, as it strongly suggests that we have historically really misunderstood microbial transmission. (Bacterial infections occurred in 2.8% of the N95 group, 5.3% of the surgical mask group, and 7.5% of the control group, with all comparisons being statistically significant. Keep in mind, however, that this is really the equivalent of a secondary outcome.)
Radonovich LJ Jr, Simberkoff MS, Bessesen MT, Brown AC, Cummings DAT, Gaydos CA, Los JG, Krosche AE, Gibert CL, Gorse GJ, Nyquist AC, Reich NG, Rodriguez-Barradas MC, Price CS, Perl TM; ResPECT investigators. N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial. JAMA. 2019 Sep 3;322(9):824-833. doi: 10.1001/jama.2019.11645. PMID: 31479137
This is the paper that has received the most attention throughout COVID, as it was published in JAMA just as the pandemic was getting underway. It is also the biggest overall study, so it certainly makes sense that it has received the most attention, but unfortunately there are some significant flaws.
It is a cluster randomized, multicenter, pragmatic trial that took place over the course of 4 consecutive flu seasons in 137 outpatient settings in 7 US hospitals. They randomized 1993 healthcare workers in 189 clusters to either wear an N95 or a medical mask when near patients with respiratory illnesses. One of the massive flaws of this study is that participants were only told to wear their masks when within 6 feet of the patient. Seeing as the 6 foot rule has no scientific basis, we might expect that a large number of staff infections occurred while they were not wearing masks, which negates the entire value of this study. The 6 foot rule also inherently biases against N95 masks, as the point of N95s is that respiratory viruses are spread through aerosols, which have always been assumed to travel further than 6 feet. So even if you believed in the 6 foot rule for droplets, the design of this study was inherently biased against N95s and their role in preventing airborne transmission.
The primary outcome of the study was laboratory confirmed influenza. Unfortunately, this included changes in serology in completely asymptomatic individuals, which in my mind is a very questionable endpoint (and clearly irrelevant to the participants).
Among the 1993 healthcare workers enrolled, there were a total of 5180 healthcare worker flu seasons covered, with only 4689 included in the per-protocol analysis. Unfortunately, based on their power calculation they needed 10,024 total healthcare worker flu seasons for their primary outcome, so the trial was drastically under-powered. I might be missing something, but I don’t see any explanation for why they stopped this trial so early in the manuscript.
There was no difference in the primary outcome, with laboratory confirmed influenza in 8.2% of the N95 group and 7.2% of the medical mask group (ARR 1.0%, 95% CI -0.5 to 2.5%, p=0.18). However, the majority of these cases were asymptomatic changes in serology. Actual influenza was quite rare, and the rate of influenza-like illness looks a touch lower in the N95 group.
Adherence wasn’t great, and was only measured by self-report, so is probably even worse than the numbers suggest. (There were occasional monitors, but seeing as they were not allowed to enter patient care rooms, and participants were only required to wear masks within 6 feet of patients, the monitoring was clearly ineffective.) Only 65% of both groups reported always wearing their masks when within 6 feet of patients with respiratory illnesses. (And this is 65% of people who responded to the question on their survey. 30% of participants didn’t even respond to the question, which suggests they weren’t wearing masks, which would bring overall compliance well under 50%.) Furthermore, participants were only asked to wear masks around patients with clear respiratory illnesses, which means they wouldn’t have been wearing masks around patients with minimal symptoms but who could still be infectious. If people aren’t wearing masks, you can’t test whether masks work.
This is ‘the trial’ that is constantly cited when people assert we don’t need to wear N95s during COVID. Unfortunately, the trial is a bit of a mess, so I don’t think that conclusion is valid. (And of course, this study was done prior to COVID, and doesn’t look at coronaviruses, so generalizability was always going to be an issue.) The entire theory behind this trial is that respiratory illnesses are droplet spread, which is probably wrong, and therefore undermines the entire study design. Only wearing masks within 6 feet of patients doesn’t make sense and is not based on any science. There is no explanation as to why the trial is less than half the size it is supposed to be. Masks were only worn approximately half the time. It was conducted in a number of outpatient clinics, where the risk of transmission is probably lower than in the emergency department. The majority of “confirmed influenza” cases were completely asymptomatic, and the rate of actual influenza-like illness looks lower in the N95 group. Overall, the weaknesses of this trial are so numerous it can’t be used to draw any solid conclusions about N95 use.
Bottom line: This trial showed no difference between N95s and surgical masks, but compliance was very low and masks were only worn within 6 feet of patients, which significantly biased the trial towards showing no difference. It cannot be used to demonstrate the equivalence of surgical masks, which is really what is required before we recommend potentially less safe PPE.
Summarizing this data
Is there definitive evidence that N95s are better than surgical masks? No. But despite the constant refrain of lack of evidence, there is actually at least 1 positive RCT, and the predominance of the evidence seems to align with basic physiology in suggesting that N95s will provide better protection than surgical masks.
Reading the RCTs is far more informative than reading the meta-analyses. It is very clear that simply combining these trials is inappropriate. In some trials, masks were worn 50% of the time or less. Some trials used unusual lab-oriented definitions of infection. Some trials were designed with the faulty assumption that airborne spread doesn’t occur. When these trials are grouped together into a meta-analysis, we are left with the impression that there is strong evidence against N95s, when in fact most of the trials offer reasonable evidence that N95s are beneficial.
We have always suggested N95s during respiratory pandemics. They were considered the standard of care during SARS, MERS, and H1N1. We have more evidence than ever that coronaviruses, and COVID-19 in particular, are spread through the airborne route. Considering N95s as the baseline standard of care, there is absolutely no way that one can look at this evidence and suggest abandoning them in favour of surgical masks. Even if you don’t consider N95s the standard of care, there is 1 positive RCT demonstrating lower infection rates with N95s, and none of the other studies are strong enough to over-rule those results. Therefore, until we see big equivalence studies, it is pretty clear that N95s are the standard of care, and I will continue wearing one whenever I see a patient with suspected COVID-19.
COVID specific data
There is one new study focused specifically on COVID-19, only available as a pre-print, that prompted me to finally write this review:
Ferris M,Ferris R, Workman C, et al. FFP3 respirators protect healthcare workers against infection with SARS-CoV-2. Authorea. June 30, 2021. DOI: 10.22541/au.162454911.17263721/v2
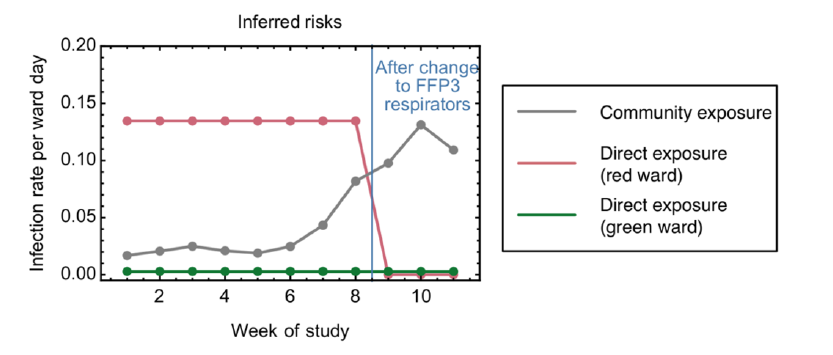
This is a pre-print study that has made headlines. It is an observational cohort looking at the rate of healthcare worker COVID infections before and after a change from standard droplet precautions with a surgical mask to routine use of an FFP3 respirator (N99 equivalent) on COVID wards.
Prior to the change, the rate of infection was higher for those working on COVID wards than non-COVID wards 7 out of 8 weeks analyzed. After the change to FFP3, the rate of healthcare worker infection was the same on COVID and non-COVID wards. There was a strong correlation between COVID rates in the community and healthcare worker infection rates on non-COVID wards, but not on COVID wards. This implies that the majority of COVID infections on COVID wards were caused by exposure at work. (The risk of exposure was 47-fold greater for those working on COVID wards as compared to those on non-COVID wards). Based on their mathematical modelling, the introduction of FFP3 respirators provided 100% protection against hospital acquired infection (95% CI 31-100%).
There are obviously many limitations to this observational data, but it seems to fit with all the available science. There is lots of data that suggests that healthcare workers are getting sick at work. The science is also pretty clear that COVID is transmitted through the airborne route. Combined, it just makes sense that the use of airborne precautions rather than droplet precautions would significantly decrease illness among healthcare workers. It is completely irresponsible that so many institutions continue to ignore the very clear evidence on this topic.
Other COVID stuff
Klompas M, Rhee C, Baker M. Universal Use of N95s in Healthcare Settings when Community Covid-19 Rates are High. Clin Infect Dis. 2021 https://doi.org/10.1093/cid/ciab539 PMID: 34113977
This editorial covers a number of important points about N95 use during the pandemic:
- Patients are generally most infectious just before and immediately following symptom onset. (This is a key point to understand about COVID transmission, and I think part of the reason we have been so lucky in hospitals, despite using inappropriate PPE. Patients generally don’t come see us until they have significant symptoms, which is past their highest point of transmissibility.)
- There are many reports of asymptomatic or pre-sympomatic patients infecting healthcare workers.
- Healthcare workers looking after undifferentiated patients are at higher risk of contracting COVID-19 than healthcare workers caring for patients with confirmed COVID-19.
- They use these points to argue that whenever community rates of COVID are high, all healthcare workers should be universally wearing N95s or an equivalent. At very least, it is clear at this point that we need to be using airborne precautions for known and suspected COVID patients.
Current Guidance
I have been consistently disappointed by the disconnect between guidelines, science, and common sense throughout this pandemic. (In fact, this is a constant ongoing issue with medical guidelines.) However, some guidelines are starting to slowly catch up to science. The American Centers for Disease Control and Prevention is now very clear that an N95 or equivalent should be used for protection against SARS-CoV-2:
- “HCP who enter the room of a patient with suspected or confirmed SARS-CoV-2 infection should adhere to Standard Precautions and use a NIOSH-approved N95 or equivalent or higher-level respirator, gown, gloves, and eye protection (i.e., goggles or a face shield that covers the front and sides of the face).” (From: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html)
Unfortunately, our public health agencies and hospitals are ridiculously behind on this issue.
Summary
Although the evidence is imperfect, there is a fairly clear signal of benefit from using N95s routinely. That certainly makes sense, as all the available science suggests that respiratory viruses like SARS-CoV-2 and influenza are spread through the airborne route, and therefore would require what we generally consider to be airborne precautions. Even if the evidence is imperfect, there is certainly no reason to overrule the precautionary principle that we have always used, in recommending N95s throughout SARS, MERS, and H1N1.
References
Ferris M,Ferris R, Workman C, et al. FFP3 respirators protect healthcare workers against infection with SARS-CoV-2. Authorea. June 30, 2021. DOI: 10.22541/au.162454911.17263721/v2
Jefferson T, Del Mar C, Dooley L, Ferroni E, Al-Ansary LA, Bawazeer GA, van Driel ML, Foxlee R, Rivetti A. Physical interventions to interrupt or reduce the spread of respiratory viruses: systematic review. BMJ. 2009 Sep 21;339:b3675. doi: 10.1136/bmj.b3675. PMID: 19773323
Klompas M, Rhee C, Baker M. Universal Use of N95s in Healthcare Settings when Community Covid-19 Rates are High. Clin Infect Dis. 2021 https://doi.org/10.1093/cid/ciab539 PMID: 34113977
Loeb M, Dafoe N, Mahony J, John M, Sarabia A, Glavin V, Webby R, Smieja M, Earn DJ, Chong S, Webb A, Walter SD. Surgical mask vs N95 respirator for preventing influenza among health care workers: a randomized trial. JAMA. 2009 Nov 4;302(17):1865-71. doi: 10.1001/jama.2009.1466. Epub 2009 Oct 1. PMID: 19797474
Long Y, Hu T, Liu L, Chen R, Guo Q, Yang L, Cheng Y, Huang J, Du L. Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta-analysis. J Evid Based Med. 2020 May;13(2):93-101. doi: 10.1111/jebm.12381. Epub 2020 Mar 13. PMID: 32167245
MacIntyre CR, Cauchemez S, Dwyer DE, Seale H, Cheung P, Browne G, Fasher M, Wood J, Gao Z, Booy R, Ferguson N. Face mask use and control of respiratory virus transmission in households. Emerg Infect Dis. 2009 Feb;15(2):233-41. doi: 10.3201/eid1502.081167. PMID: 19193267
MacIntyre CR, Wang Q, Cauchemez S, Seale H, Dwyer DE, Yang P, Shi W, Gao Z, Pang X, Zhang Y, Wang X, Duan W, Rahman B, Ferguson N. A cluster randomized clinical trial comparing fit-tested and non-fit-tested N95 respirators to medical masks to prevent respiratory virus infection in health care workers. Influenza Other Respir Viruses. 2011 May;5(3):170-9. doi: 10.1111/j.1750-2659.2011.00198.x. Epub 2011 Jan 27. PMID: 21477136
MacIntyre CR, Wang Q, Seale H, Yang P, Shi W, Gao Z, Rahman B, Zhang Y, Wang X, Newall AT, Heywood A, Dwyer DE. A randomized clinical trial of three options for N95 respirators and medical masks in health workers. Am J Respir Crit Care Med. 2013 May 1;187(9):960-6. doi: 10.1164/rccm.201207-1164OC. PMID: 23413265
MacIntyre CR, Wang Q, Rahman B, Seale H, Ridda I, Gao Z, Yang P, Shi W, Pang X, Zhang Y, Moa A, Dwyer DE. Efficacy of face masks and respirators in preventing upper respiratory tract bacterial colonization and co-infection in hospital healthcare workers. Prev Med. 2014 May;62:1-7. doi: 10.1016/j.ypmed.2014.01.015. Epub 2014 Jan 25. Erratum in: Prev Med. 2014 Dec;69:165. PMID: 24472436
Mark Ferris, Rebecca Ferris, Chris Workman, et al. FFP3 respirators protect healthcare workers against infection with SARS-CoV-2. Authorea. June 30, 2021. DOI: 10.22541/au.162454911.17263721/v2
Radonovich LJ Jr, Simberkoff MS, Bessesen MT, Brown AC, Cummings DAT, Gaydos CA, Los JG, Krosche AE, Gibert CL, Gorse GJ, Nyquist AC, Reich NG, Rodriguez-Barradas MC, Price CS, Perl TM; ResPECT investigators. N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial. JAMA. 2019 Sep 3;322(9):824-833. doi: 10.1001/jama.2019.11645. PMID: 31479137
Smith JD, MacDougall CC, Johnstone J, Copes RA, Schwartz B, Garber GE. Effectiveness of N95 respirators versus surgical masks in protecting healthcare workers from acute respiratory infection: a systematic review and meta-analysis. CMAJ : Canadian Medical Association journal. 188(8):567-74. 2016. PMID: 26952529 [free full text]


17 thoughts on “The evidence suggests N95s are better than surgical masks”
Wow. This is super scary. I have worn a surgical mask for the entire pandemic, except for intubation and CPR (if I remembered to switch out).
I think the big barriers are small numbers of events – I feel like our entire department has had covid at some point or another, but because it staggered over months, we didn’t really feel the loss of the workforce.
I also feel like cost is a barrier – I don’t know exactly what is the price difference between a surgical mask and N95, but if it’s multiplied by 1 per staff member per shift, it could be the reason guidelines are staggering.
Surgical masks and N95 respirators are very different kinds of masks. But surgical masks have not met all the standards that a N95 or higher-level respirator has.