
Although the paper is not even officially published yet, everyone has already heard the results. We have our first treatment that appears to reduce mortality in COVID. For a week, we were stuck with only a press release, which is a really bad way to practice medicine. Now, we have a pre-print manuscript, so without further ado, let’s discuss the RECOVERY trial and dexamethasone for COVID.
The paper
Horby PW et al. Effect of Dexamethasone in Hospitalized Patients With COVID-19 – Preliminary Report. medRxiv Preprint 2020. [Epub Ahead of Print] **Note – this is a preprint version of the paper. It has not been peer reviewed yet.** NCT04381936
The Methods
This is a pragmatic, open-label, multi-centre RCT from 176 hospitals in the United Kingdom. (This is part of a much larger trial, in which 11,320 patients have already been randomized. The trial also looks at other therapies for COVID.)
Patients
Hospitalized patients with clinically suspected or laboratory confirmed COVID who, in the opinion of the treating clinician, had no medical conditions that would have put them at risk from receiving dexamethasone. They started the trial by only including adult patients, but part way through opened it to all age groups (although in this draft they don’t tell us how much children were actually included).
Intervention
Usual care plus dexamethasone 6mg daily (either orally or intravenously) for up to 10 days, or until discharge.
Comparison
Usual care.
Outcome
The primary outcome was all cause mortality at 28 days.
The Results
They randomized 2104 patients to the dexamethasone group and 4321 to usual care. The mean age of this cohort was 66 years, with 36% of patients being female, and half having at least one comorbidity. At the time of randomization, 16% were on mechanical ventilation or ECMO, 60% were receiving oxygen (including noninvasive ventilation), and 24% were on no oxygen support.
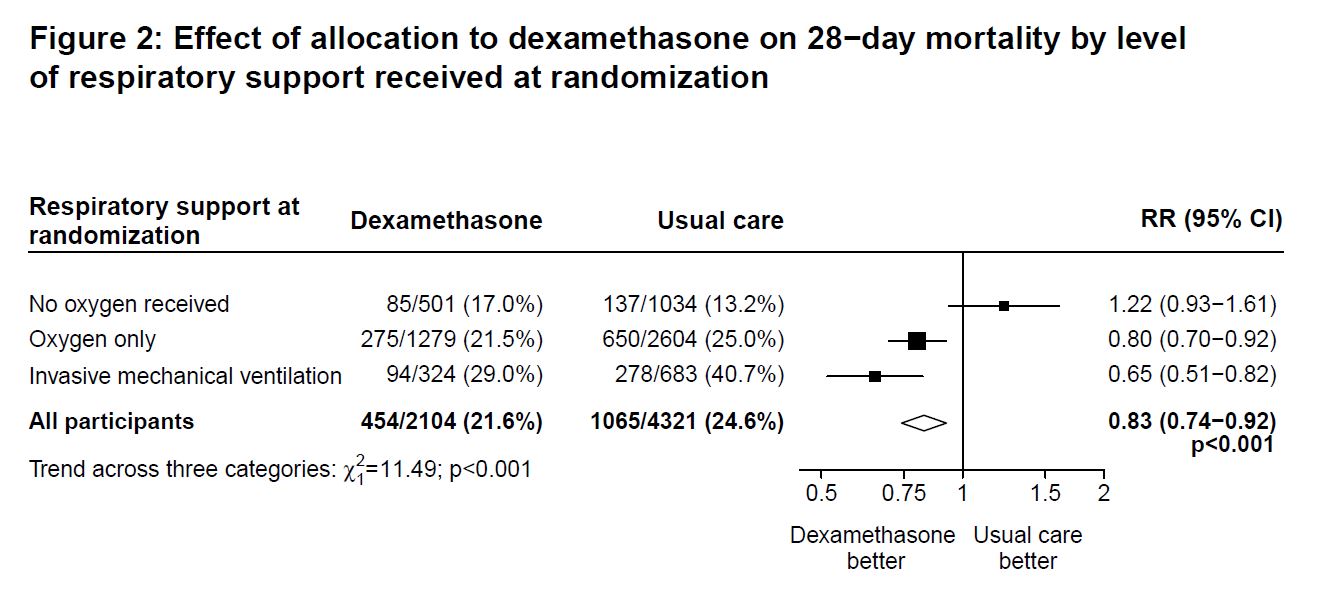
Mortality was lower in the dexamethasone group (21.6% vs 24.6%; OR 0.83; 95% CI 0.74-0.92, P<0.001).
Based on a pre-specified subgroup analysis, the biggest benefit was seen among the sickest patients (those on mechanical ventilation). There was a 11.7% absolute reduction in mortality among the patients on mechanical ventilation, a 3.5% reduction among patients on oxygen, and a 3.8% increase in mortality (not statistically significant) among those who weren’t on oxygen.
The benefit appeared to occur later in the disease course. Those who had more than 7 days of symptoms benefited from treatment, whereas those with less than 7 days of symptoms had no benefit.
Dexamethasone also results in a shorter duration of hospitalization (median 12 vs 13 days) and a greater probability of being discharged within 28 days (RR 1.11, 95% CI 1.04-1.19).

My thoughts
I am very glad to see this data published. This is still just a pre-publication version of the paper, but unlike a press release, this publication really gives us everything we need to analyze the study. (Honestly, I am not sure how much value traditional journals really offer us these days. The Surgisphere debacle is just another in a long line of reminders that peer review is imperfect, at best. We want to analyze these papers for ourselves, so does an anonymous and invisible peer review process really add anything of value?) Either way, I think we all agree that science by press release is incredibly harmful and should be avoided at all costs.
These results are incredibly promising. They can and should change practice immediately. I think the biggest risk, which almost always exists when we see promising results, is indication creep. That is, we might erroneously extrapolate the excellent results here to inappropriate patients. This is especially true for patients who would have been excluded from this trial, but the data suggests that there are even subgroups in whom we may wish to withhold treatment. (Of course, we should always be careful in interpreting subgroup analyses, but these results were predicted, and therefore relatively believable.)
As a general rule in medicine, harms tend to be relatively equal across subgroups, but higher risk patients will see larger absolute benefits from effective therapies. Unfortunately, we often try to extrapolate those bigger benefits back to the low risk patients, allowing the net harms to outpace the net benefits. Looking at the subgroups, there is clear benefit among the sickest patients (those on mechanical ventilation or requiring oxygen), but there is a hint of possible harm when dexamethasone was given to patients who didn’t require oxygen. This is supported by the theory that sicker patients are likely to be in the hyper-inflammatory or cytokine storm stage of their illnesses and therefore require immunosuppression. Conversely, less sick patients may actually be harmed by immunosuppression. We therefore need to be careful about who gets this medication.
Interestingly, the authors note that in the UK oxygen therapy is suggested for patients with room air saturations between 92 and 94%. That seems like a pretty high cut-off to me. I wouldn’t normally start oxygen until the room air saturation fell below 90%, and I go even lower in patients with chronic lung disease. However, a patient with a room air sat of 92% might have been included in the oxygen therapy subgroup of this trial, and therefore may benefit from treatment. I am not entirely sure how to apply this clinically.
The timing of therapy is also interesting. Unlike antivirals, that really need to be given early to have their maximal effect, dexamethasone only seemed to help patients who received it later in their disease course. That makes sense, as we believe that the early stages of COVID are predominated by viral replication, while the later stages represent the effects of systemic inflammation. Steroids could actually be harmful in the early stages (by reducing immune response and allowing increased viral replication), while they appear to be beneficial later in the disease course.
They use a pretty small dose of dexamethasone in this trial. Had the trial been negative, I might have wondered whether they had used too small a dose. It is possible that we could see even better results with a larger dose, but it is also possible that we would just see more harms without any increase in benefit. Assuming this trial is followed by further RCTs, I think there is probably room to test multiple doses. However, for now, I would just follow their protocol.
Being a pragmatic trial, we are missing a lot of the granular detail we would love to see. What effect did dexamethasone have on viral loads, vital signs, and SOFA scores, for example. That data would be helpful when trying to assess the biologic plausibility of the results we are seeing. However, it is not nearly important enough to outweigh the incredible benefit of getting 6,000 patients randomized in 3 months.
It is obviously incredibly difficult to design a trial when you know very little about the condition being studied. I think these researchers did an incredible job starting the trial without a sample size calculation, but then adjusting on the fly as new data became available, and using blinded statisticians to perform an appropriate power calculation after the trial was underway.
Unfortunately, the lack of blinding is an issue that introduces a significant risk of bias. All cause mortality is an objective outcome, which mitigates that bias to some extent, but cannot fully exclude the potential for biased outcomes. This is especially true in the context of modern critical care, where a large proportion of deaths are always due to withdrawal of care, and therefore mortality shifts towards a less objective outcome. They do not list causes of death in this manuscript, but I imagine that a reasonable number were due to withdrawal of care. Practically, I understand why this trial was open label, but we have to consider the additional risk of bias when interpreting these results. Thus, I think we have to downgrade our certainty about the results.
Selection bias probably also occurred in this trial, and is important to consider when applying these results. Patients were excluded if the treating physician thought that the patient shouldn’t receive dexamethasone, and therefore harms will probably be greater in the general population. (There were also patients that were missed simply because dexamethasone wasn’t available in the hospital.) We should attempt to apply the same exclusion criteria clinically, and withhold steroids from patients we believe to be at higher risk of adverse events.
Steroids have been widely studied in community acquired pneumonia, viral pneumonia, and ARDS. (Siemieniuk 2016; Villar 2020; Wu 2020; Ye 2020) I have been meaning to write a deep dive on the topic for a while, and will try to get one out soon as a follow up. As a quick summary, although I don’t think the results are definitive, there are lots of hints that steroids could be beneficial in lung infections and ARDS. I think it was more likely that dexamethasone was going to demonstrate a benefit in COVID than any of the suggested antivirals. In that context, the RECOVERY trial results are enough to convince me that all critically ill COVID patients (those requiring oxygen support) should be given dexamethasone for the time being, but that these results should still be followed with a properly blinded RCT.
Bottom line
This open label RCT demonstrates a mortality benefit from dexamethasone in COVID. There are significant potential sources of bias that should limit our certainty in the results. The benefit seems to be limited to patients requiring supplemental oxygen. Personally, I would prescribe dexamethasone to all admitted COVID patients requiring oxygen, but will not use it otherwise.
Other FOAMed
REBEL EM: The RECOVERY Trial: Dexamethasone for COVID-19?
FOAMCast: COVID-19: Dexamethasone [RECOVERY trial]
BroomeDocs: CoVid, Dex and Death… Recovery
PulmCrit: Dexamethasone & COVID – a study in immunopathology, evidence-based medicine, and ourselves
Other COVID EBM
Aerosols, Droplets, and Airborne Spread: Everything you could possibly want to know
Remdesivir: The first real trial
Can we safely reuse N95 masks?
Hydroxychloroquine for COVID: No good evidence
References
Horby PW et al. Effect of Dexamethasone in Hospitalized Patients With COVID-19 – Preliminary Report. medRxiv Preprint 2020.
Siemieniuk RA, Alonso-Coello P, Guyatt GH. Corticosteroid Therapy for Patients Hospitalized With Community-Acquired Pneumonia. Ann Intern Med. 2016;164(9):636-637. doi:10.7326/L15-0583 PMID: 27136220
Villar J, Ferrando C, Martínez D, et al. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respir Med. 2020;8(3):267-276. doi:10.1016/S2213-2600(19)30417-5 PMID: 32043986
Wu C, Chen X, Cai Y, et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China [published online ahead of print, 2020 Mar 13]. JAMA Intern Med. 2020;e200994. doi:10.1001/jamainternmed.2020.0994
Ye Z, Rochwerg B, Wang Y, et al. Treatment of patients with nonsevere and severe coronavirus disease 2019: an evidence-based guideline [published online ahead of print, 2020 Apr 29]. CMAJ. 2020;192(20):E536-E545. doi:10.1503/cmaj.200648
Morgenstern, J. Dexamethasone for COVID: The RECOVERY trial, First10EM, June 23, 2020. Available at:
https://doi.org/10.51684/FIRS.26745




8 thoughts on “Dexamethasone for COVID: The RECOVERY trial”
Hi Justin. Long time since UWO
Interesting if you look at Table 1… the hospitalized patients not on O2 were much older and somewhat more comorbid. Perhaps some of the tendency to harm is that you must think what sort of patient gets admitted for a condition with no proven treatment without hypoxia? These fragile elders are just the type to do poorly from delirium hyperglycemia
Etc
Absolutely – although the trial is randomized, the subgroups are really just observational data, and there are many confounders that could affect why patients were or were not on oxygen. There is a reasonable chance that I bought too much into the subgroups because they fit with my expectations of what this trial would show. I think it makes sense that steroids would work better with sicker patients in COVID, and pretest probability counts for something, but probably shouldn’t override the major limitations of subgroups.
Perhaps the best conclusion from this trial is that steroids given to all comers reduced mortality, and we should just ignore the subgroups. We won’t really know unless we see follow up trials.
Hello
” Interestingly, the authors note that in the UK oxygen therapy is suggested for patients with room air saturations between 92 and 94%. ”
Recently, there was a healthy discussion in my department about this topic, and then I remembered having read this in the blog a while ago, but then we searched for it in the RECOVERY paper and we couldn’t find the statement. Can you please tell me where you read it?
Bernardo Vidal Pimentel
Was in the last paragraph of the discussion
Doesn’t look like I can share a screen shot, but it says “Based on these results, 1 death would be prevented by treatment of around 8 patients requiring invasive mechanical ventilation or around 25 patients requiring oxygen (which, in the UK, is recommended when oxygen saturations on room air are 92-94%)”