
There was a bit of a social media fracas a few weeks ago when the first ‘trial’ of remdesivir for COVID-19 was published in the New England Journal of Medicine. (The journal being a red flag that you might be seeing advertising rather than real science). It was an uncontrolled observational cohort from a highly select group of patients, with significant financial conflicts of interest, so I decided not to write anything about it. (I did add it to the main COVID antiviral page, and you can read all about this trial on blogs like PulmCrit.) However, remdesivir is back in the news – and not just because of leaked trial results and stock market manipulation – but because the first real trial has been published.
The paper
Wang Y, Zhang D, Du G, et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. The Lancet. 2020; [article] NCT04257656
The Methods
This is a double blind, placebo controlled trial from 10 hospitals in China.
Patients
Adult patients admitted to hospital with confirmed COVID-19 pneumonia based on PCR testing and radiologic findings, with symptoms less than or equal to 12 days, and an oxygen saturation less than 95% or a P/F ratio of <300.
Intervention
Remdesivir 200 mg IV on day one then 100 mg IV daily for 10 days total.
Comparison
Placebo.
Outcome
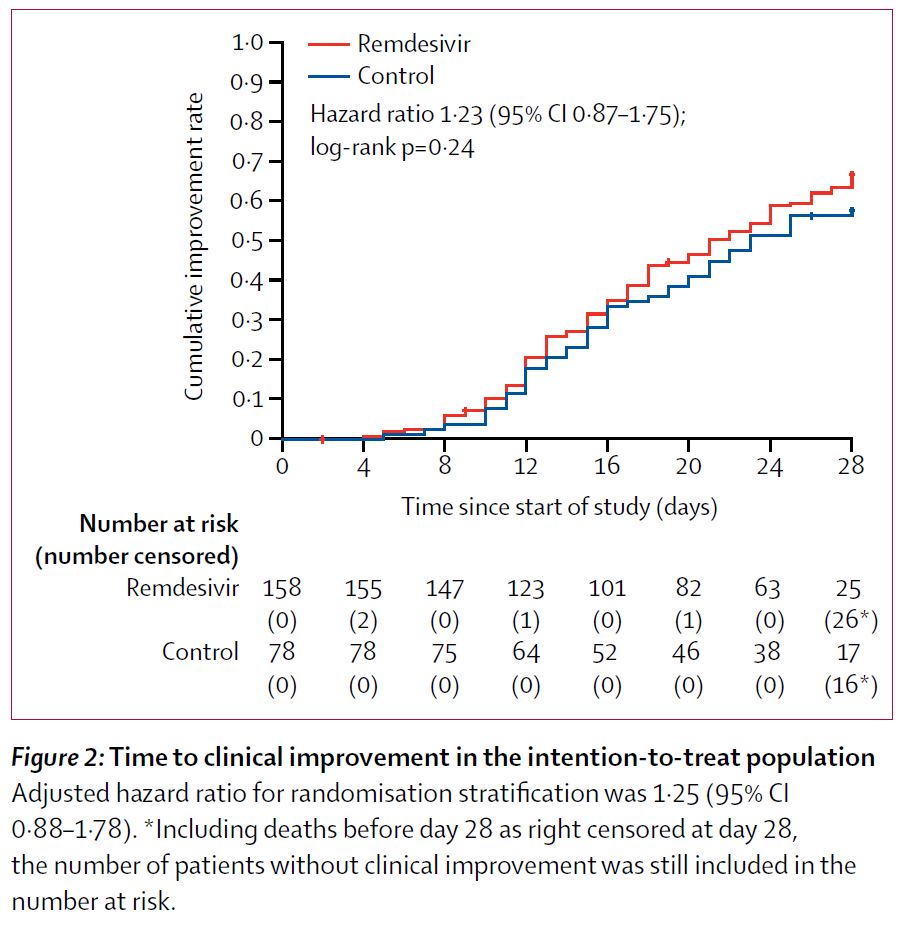
The primary outcome was time to clinical improvement, which was defined as discharge from hospital or a 2 point improvement on the following scale:
- 6 = death
- 5 = Hospital Admission for ECMO or Mechanical Ventilation
- 4 = Hospital admission for NIV or HFNC
- 3 = Hospital admission for O2 therapy (but not requiring HFNC or NIV)
- 2 = Hospital admission but not requiring O2 therapy
- 1 = Discharged or having reached discharge criteria
The Results
They enrolled 237 patients, 158 of whom received remdesivir. Most patients were moderately ill on admission (requiring some oxygen, or a level 3 on their scale). The median age was 65 and 70% of participants had at least one comorbidity, with hypertension being the most common. The median time from symptom onset to enrollment in the study was 10 days.
There was no difference in the primary outcome. Time to clinical improvement was 21 days with remdesivir and 23 days with placebo (HR 1.23; 95% CI 0.87 – 1.75).
There was also no difference in mortality (14% vs 13%; ARR -1.1% 95% CI -8.1 to 10.3%).
There was also no statistical difference in length of mechanical ventilation, although the numbers look better in the remdesivir group (7 days vs 15.5 days; ARR -4.0 95% CI -14 to 2%).
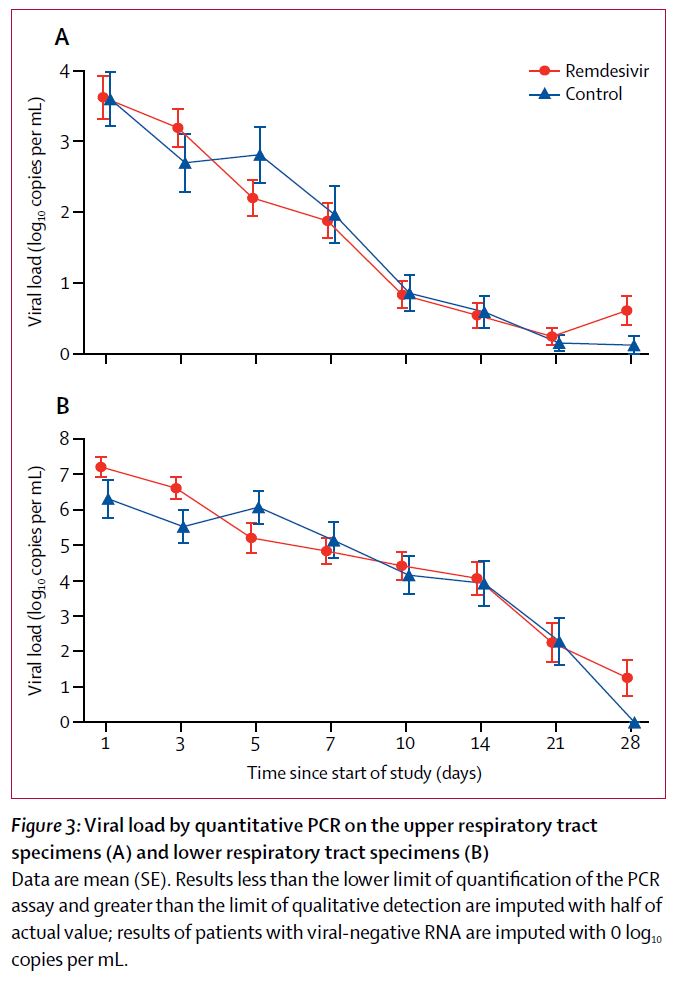
Perhaps most importantly, this antiviral had exactly 0 impact on viral clearance, so there is no biologic rationale to expect better clinical outcomes with remdesivir.
My thoughts
In the context of COVID, this is a fantastic study. It is the first double blind, placebo controlled trial that we have seen, and it gives us important information. People are always disappointed by “negative” results, but this study has the potential to save many lives by stopping physicians around the world from prescribing an ineffective and potentially harmful medication. That is an essential contribution to science.
People always quibble about how we phrase the outcomes of these studies. There was no statistical difference in the outcome here, but that doesn’t exclude any possible difference. A bigger trial might show a small difference between the groups. However, with 236 patients, it is clear that remdesivir is not a miracle cure.
That being said, the study was terminated early. They originally planned to enroll 325 patients. I have talked before about the danger of terminating trials early for benefit, and the potential of early termination to hide harms, but it is also important to remember that early termination can result in a type II error, in that the trial becomes under-powered, and no benefit is seen despite a benefit truly existing.
As was discussed in the initial antiviral post, the timing of antiviral therapy is interesting. Treating patients on the tenth day of symptoms might simply be too late, as the disease may have transitioned from a viral replication phase to a primarily inflammatory phase. However, trying to treat people early might also be a losing strategy, as most people won’t benefit from therapy, and you end exposing a lot more patients to the harms of therapy.
Speaking of which, the overall adverse events were equal between the two groups, but the remdesivir group did have more patients who had to stop their treatment early because of adverse events. Furthermore, this study is just too small to say anything conclusive about harms.
Overall, this is a negative trial and I believe the results. That being said, there are actually two remdesivir trials that people are talking about this week, and the other trial is apparently positive. I say apparently because the trial has not actually been published yet and so all we have is press releases and uncritical statements by politicians, which are very dangerous sources for medical and scientific knowledge.
It would probably be silly to say anything too negative about remdesevir when we know a “positive” trial will be published any day. All the same, we need to consider our pretest probability. Although COVID-19 is new, viral pneumonia is a yearly scourge, and no therapy has ever been shown to improve important outcomes in viral pneumonia. (No, tamiflu doesn’t work.) For that reason, our pretest probability should be very low. It should take a lot to convince us that an intervention works for COVID-19. A single trial, especially if flawed, may not be enough to overcome the mountain of evidence thus far that our drugs don’t help viral pneumonias. Unfortunately, given the sheer number of studies underway (often with imperfect methodology), we are bound to see a few that look positive by chance alone, despite there being no real benefit. Considering how the media (and even many doctors) have responded to crappy observational data, I anticipate that people will similarly over-react to the first “positive” RCT. It is our job as science based doctors to reign in that insanity, and help people interpret the data for what it actually shows.
Bottom line
This well done, placebo controlled, randomized trial demonstrates no benefit from intravenous remdesivir in moderately sick COVID-19 patients.
Other FOAMed
REBEL EM: Two More Trials Just Published on Remdesivir
PulmCrit: First placebo-controlled RCT on remdesivir for COVID-19
References
Grein J, Ohmagari N, Shin D, et al. Compassionate Use of Remdesivir for Patients with Severe Covid-19 [published online ahead of print, 2020 Apr 10]. N Engl J Med. 2020;NEJMoa2007016. doi:10.1056/NEJMoa2007016 PMID: 32275812
Wang Y, Zhang D, Du G, et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial The Lancet. 2020; [article]
Morgenstern, J. Remdesivir: The first real trial, First10EM, May 1, 2020. Available at:
https://doi.org/10.51684/FIRS.19756



One thought on “Remdesivir: The first real trial”