
December 1,2020: This post was based on the best available evidence at the beginning of the pandemic (March-April 2020). The information contained is still very relevant, but there is also now an updated/companion review specifically looking at the transmission of COVID-19 (and concluding aerosols play a very important role in it’s transmission), that can be found here.
The rapid emergence of COVID-19 has created tremendous uncertainty in medicine. We don’t know where this pandemic is headed. We don’t know the ideal management strategy. Every day brings conflicting information. Emergency medicine is a field that embraces (or at least tolerates) uncertainty, but knowledge is an important pillar of our sense of control in medicine, and COVID-19 is doing a good job highlighting massive gaps in our knowledge. One of those gaps is the precise mechanisms through which infectious diseases spread and how best to protect ourselves. We hear terms like “aerosol generating” and “droplets”, but their precise meaning can be unclear, and so it is hard to know how to adjust our practice. In this post, I will review everything I have been able to learn about aerosols and droplets, how they spread, and how they should impact our practice.
I will start with a major caveat: despite reading hundreds of papers on this topic, I still have a lot of uncertainty. I think that uncertainty is born from uncertainty in the literature. There was debate and conflicting information with every new paper I found. However, it is also important to recognize that I am an emergency physician attempting to distill in a few weeks topics that people have dedicated entire careers to. If you think I missed something, or want to add to the discussion, please do so below.
I also want to acknowledge that these are incredibly trying times. We are all anxious, and that anxiety is made worse by the conflicting information that we are receiving. There is a risk that by adding even more potentially conflicting information I might add to that anxiety. I think science is fundamentally important. I think this information is important. How we act on this information is equally important. Remember that nothing here is definitive. In already trying times, we don’t want to create conflict with our colleagues. Try to use any information available to work collaboratively, focusing not on the negatives of uncertainty and disagreement, but on the positives of growth and a common goal of safety for all healthcare workers and our patients. For the most part, I am reassured by what I read, and will continue to work hard to use this information to keep my entire team safe.
What exactly is an aerosol?
I have to say, I didn’t expect this to be such a complicated question to answer. There is actually a pretty heated academic debate, centering around desiccation rates and the formulas for turbulent flow, such that it seems that no one really agrees on an exact definition. You will see some pretty definitive definitions in some sources, but that definition will invariably be refuted in the next paper you encounter. In general, aerosols are liquid or solid particles suspended in air. (Tellier 2009; Judson 2019) They can be visible, like fog, but are most often invisible, like dust or pollen.
They are often divided into small droplets (and many, but not all, people reserve the term “aerosol” to refer only to these small droplets) and large droplets. Large droplets drop to the ground before they evaporate, causing local contamination. Disease transmission through these large droplets is what we often refer to as “droplet/contact spread”, where disease transmission occurs because you touch a surface contaminated by these droplets, or get caught within the spray zone when the patient is coughing. Aerosols are so small that buoyant forces overcome gravity, allowing them to say suspended in the air for long periods, or they evaporate before they hit the floor, leaving the solid particulate (“droplet nuclei”) free to float very long distances, causing what we often refer to as “airborne” transmission. (Nicas 2005; Judson 2019)
Respiratory aerosols are created when air passes over a layer of fluid. (Fiegel 2006; Morawska 2006) There are a large number of factors that can alter this process. The viscosity of the fluid layer is an important determinant of aerosol generation, and could be a very important practical consideration in medicine. Increases in surfactant increase overall droplet formation, and produce smaller droplets (which will travel farther). (Fiegel 2006) This could be an important consideration, as some people are discussing the use of surfactant to manage COVID-19 lung disease. Conversely, nebulized saline has been shown to decrease the number of bio-aerosols produced, and has been suggested as a possible (but unproven) infection control strategy. (Fiegel 2006)
In the world of aerosols, there seems to be two main points of contention. The first is the size cutoff between large and small droplets. Various sources will put the cutoff at 2 µm, 5 µm, 10 µm, 20 µm, or even 100 µm. (Judson 2019; Morawska 2006; Fiegel 2006; Xie 2007; Chen 2010; Nicas 2005; Tellier 2009) This is a key distinction, because it is the difference between airborne and droplet precautions. Many papers make definitive statements based on one of the cutoffs that would be incorrect if a different cutoff was used. (For example, Morawska 2006 states that droplets smaller than 100 µm, which is almost all droplets, will evaporate before hitting the floor, meaning that they can transmit disease through the airborne route, while other documents will use 5 µm as the cutoff.) There is probably a grey area in which droplets can behave either way, depending on how quickly they evaporate compared to how quickly they fall to the ground based on the atmospheric conditions of the room.
The second main point of contention is exactly how clean the distinction between airborne and droplet transmission is. Some sources treat this as black and white, but others point out that large droplets evaporate and become smaller, and most activities create a very large variety of sizes, so it is more like a spectrum than a dichotomous distinction. A lot of epidemiologic studies will make strong claims that a disease is only spread by close contact, but we have to remember, those studies cannot possibly distinguish between short distance aerosol transmission (I caught it while breathing a few feet away from you) and contact transmission (I touched the door handle and then rubbed my eye.) Too often, if you were close together, studies will just assume it was contact instead of aerosol spread, biasing the literature in that direction.
What are aerosol generating procedures?
An aerosol generating procedure is a medical procedure that creates aerosols in addition to those that the patient creates regularly from breathing, coughing, sneezing, and talking. (Judson 2019) In other words, it is important to remember that patients will create their own aerosols even when we are not performing these procedures. Aerosol generating procedures can produce both large and small droplets. Each procedure will be unique, so they really need to be considered independently. (Judson 2019) Importantly, aerosol generating procedures can cause transmission through pathways that microbes don’t usually use (a virus normally spread through contact or droplets can become airborne). Procedures can either generate aerosols directly or by inducing the patient to cough or sneeze, a distinction that may be important when trying to mitigate risk. (Judson 2019)
Although respiratory infections are the primary source of aerosols, they are created in other ways as well. Surgery can aerosolize pathogens found in the blood or tissues. (For example, HIV was found in aerosols created by surgical power tools.) (Judson 2019) Aerosols can also be produced by seemingly mundane things, such as fast running tap water and flushing toilets. (Morawska 2006)
Because the individual risks (and benefits) of each procedure is likely unique, I will consider them each independently. For the sake of space, I have done so in a second post that accompanies this one.
Aerosols and normal activities
Throughout our preparations for COVID-19, we have all been incredibly focused on aerosol generating procedures, but it is important to understand that aerosols are also produced through normal human activities, including simply breathing. (Tellier 2009; Asadi 2019) Essentially any air passing through the respiratory tract will create droplets. The clinical significance will depend on the number of droplets produced, their size, the concentration of infectious agents, the frequency with which the activity is performed, and the PPE used by staff. (Morawska 2006) For example, although a single cough produces far more droplets (of all sizes) than a single breath, breathing occurs much more frequently, and so may be responsible for more droplet production overall. (Morawska 2006; Fiegel 2006) It is also important to understand that although the majority of the droplets produced by a cough may be small enough to stay airborne, their small size means that collectively they add up to only a tiny fraction of the volume produced (perhaps less than 0.1%), and therefore only a tiny fraction of the total virus spread. (Nicas 2005) However, despite carrying smaller numbers of microorganisms, there is evidence that smaller droplets don’t need to contain as many microorganisms as larger droplets to cause a clinical infection (by several orders of magnitude). (Nicas 2005; Tellier 2009) Furthermore, we must remember that not every droplet will contain virus, and even if it does, it may not be enough to effectively transmit disease.
Table adapted from Morawska 2006, with similar numbers reported in the Fiegel 2006 review:
| Activity | Number of droplets produced | Small (1-2 um) aerosols? |
|---|---|---|
| Normal breathing (5 min) | A few | Some |
| Single strong nasal exhalation | Few to a few hundred | Some |
| Counting out loud (talking) | Few dozen to few hundred. Some sources say a few thousand (Xie 2007) | Mostly |
| Cough | Few hundred to many thousand | Mostly |
| Sneeze | Few hundred thousand to a few million | Mostly |
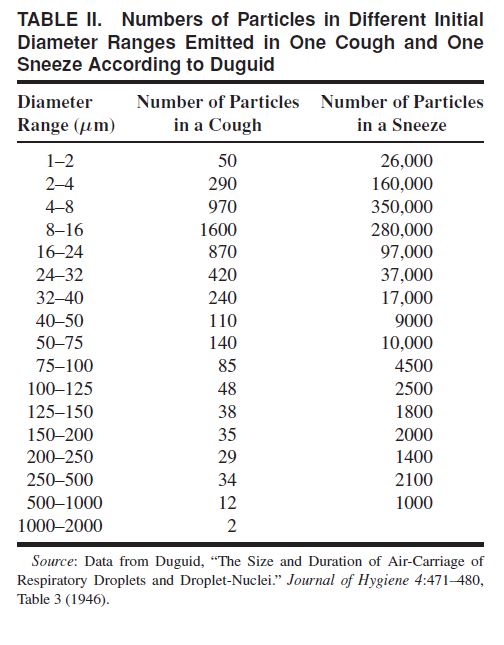
If you want a more specific breakdown, you can look at table 2 from Nicas 2005, but these numbers are estimates, and you will see different numbers even in this same paper:
Older studies concluded that humans primarily produce large droplets, but they were significantly limited because their instruments were insensitive to smaller sizes. (Morawska 2006) Recent research has indicated that as many as 80-90% of the particles generated by human exhalation are smaller than 1 µm in size. (Papineni 1997) Although the exact size of droplets produced is still debated, most sources agree that speaking, coughing, and sneezing produce droplets that are sufficiently small to remain airborne. (Fiegel 2006; Chen 2010)
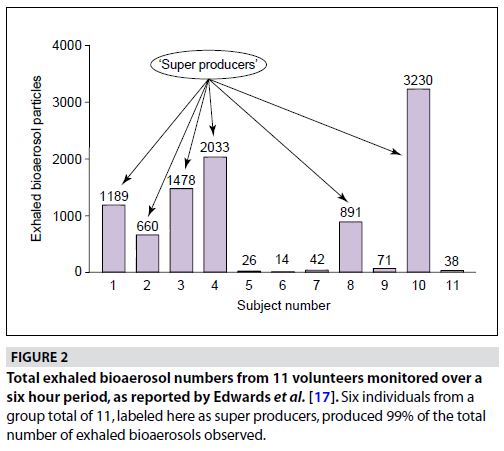
Interestingly, the total amount of bioaerosols produced varies tremendously among individuals, with some people creating very few, and others acting as “super producers”. (Fiegel 2006) I wonder whether this explains why we have observed super-spreaders of SARS and COVID-19, as “it appears that a minor percentage of the population will be responsible for disseminating the majority of exhaled bioaerosol”. (Fiegel 2006)
Vomiting, in which humans can shed up to a million virus particles per milliliter of vomit, can also produce aerosols. (Morawska 2006) A vomiting SARs patient was associated with nosocomial spread in a hospital in Hong Kong, although it isn’t clear by what route (contact, droplet, or airborne) the transmission occurred. (Morawska 2006) Similarly, there can be as many as a hundred million virus particles in every gram of feces, and flush toilets are known to result in aerosolization. As is discussed below, this form of aerosolization is thought to have spread SARS in the Amoy Garden apartment complex in Hong Kong. (Morawska 2006)
However, whether these aerosols are capable of transmitting disease still depends heavily on the number produced, the concentration of the infectious agent, the virulence of the microbe, environmental factors (the virus needs to be able to survive, whether in the air or on a surface, until it enters a host), and the health and immunity of the host. (Morawska 2006) Although it is clear that aerosols are commonly produced, it is also clear that the vast majority of disease transmission occurs among people who are in very close contact and therefore exposed to the largest of the droplets.
The fact that humans constantly produce aerosols is really important when assessing studies of aerosol generating procedures. The result sections of these papers will often only present a change in aerosols from baseline, and frequently our procedures won’t produce more droplets. However, if you look closely, we are already producing a ton of aerosols, and even if the procedures don’t produce more, their ability to spread those aerosols further is a big concern. (Simmonds 2010; Rule 2018)
Update: In one of the more entertaining and yet still scientific tweetorials of all time, Dr. Andy Tagg asks the question, “Is farting an aerosol-generating procedure?”:
What happens to the aerosol after it is expelled?
The only constant I could find in this data was a general lamentation of the lack of experimental data. (Nicas 2005; Xie 2007; Tellier 2009; Judson 2019) Most of the numbers we use clinically are based on mathematical models making large numbers of (potentially faulty) assumptions. Where droplets end up is regulated by a huge number of factors. The primary factor is probably the size of the droplet. A 1000 µm droplet will fall 1 meter in 0.3 seconds. A 100 µm droplet will take 3 second to fall 1 meter. A 10 µm droplet will take 300 seconds, and a 1 µm droplet will take 30,000 seconds. (Morawska 2006) How long a droplet remains in the air is clearly a huge factor in how far it is able to travel, and how likely healthcare workers are to be exposed.
As I said, exact size cutoffs are controversial, but Chen (2010) suggests that the distribution of all droplets between 0.1 and 200 µm will primarily be influenced by ventilation patterns and the initial velocity of the droplet, rather than gravity. In other words, these droplets do not just drop to the ground within 1-2 meters of the patient, as many infection control practices assume. However, the distribution of droplets is also influenced by a very large number of factors, including relative humidity, temperature, ventilation pattern and rate, initial velocity, shape of the human body, and droplet nuclei size and composition. (Xie 2007; Chen2010) Most of these factors are dynamic (droplet size changes as it evaporates and temperature changes as you move away from a febrile patient), making simplified calculations difficult. At smaller sizes, Brownian motion, electrical forces, thermal gradients, and turbulent diffusion have much bigger impacts. (Morawska 2006) Overall, it is complicated, there are lots of formulas, and reading these papers generally left me with a headache.
Many calculations regarding droplet distribution have significant assumptions embedded. For example, initial studies that estimated droplet dispersion made the assumption that the droplets were introduced into the air without any velocity, which is a bad assumption when coughing and sneezing can create tremendous initial particle velocities. (Morawska 2006) As general estimates, particles produced by normal breathing have a velocity of approximately 1 m/sec, talking 5m/sec, coughing 10 m/sec, and sneezing 20-50 m/sec. (Xie 2007) Thus, even though large particles are often assumed to land close to the patient, that assumption is frequently incorrect. (Bourouiba 2020) Think about walking by the sea on a windy day. Large droplets that usually only travel a very short distance can easily reach you a long way from the shore. (Judson 2019)
There are some mathematical models and experimental data that support the 2 meter rule for normal breathing and talking, but most suggest that coughing and sneezing spread droplets far further. (Xie 2007; Hui 2014; Bourouiba 2020) However, this rule only applies to large droplets. Smaller droplets remain trapped in the air and therefore can travel much greater distances. Unfortunately, most of these models ignore the impact of the patient covering their mouth and nose when they sneeze. Hopefully all of these patients are wearing masks while sneezing in the hospital, which will clearly change the distribution of droplets, and makes the 7-8 meter number less likely to be true. (Bourouiba 2020)
So how far do these droplets travel? I think this science makes it clear that there is no simple answer. Small droplets will remain in the air for very long periods of time (become airborne), but the exact cutoff is unknown, and can change significantly based on factors like temperature and humidity. With normal breathing, large droplets mostly fall to the ground within a 2 meter radius, but they can evaporate and become small droplets. (Nicas 2005) Coughing and sneezing can propel these large droplets much further – at least 6 meters or 18 feet. (Bourouiba 2020)
Perhaps the most important thing to remember is that this distribution is probabilistic. (Morawska 2006) There is nothing that guarantees a droplet will stop before a certain distance. When we make statements like, droplets over size X will fall to the floor within distance Y, what we really mean is that most droplets will. Luckily, for most diseases, knowing where most of the droplets end up is probably good enough.
As a quick aside, some sources will state that very small particles are not dangerous, because although you might breath them in, they remain in the air and are not retained in the alveoli. However, it appears this is not true, with 50% of particles smaller than 1 µm being retained in the respiratory tract. (Morawska 2006)
Influenza: droplet or airborne?
We need to think about the practical implications of all this basic science. Nobody is all that worried about influenza right now, but it is important to know a little bit about the transmission of influenza, because almost all of our PPE recommendations are based on extrapolations from this more common disease. Although the science is not definitive, it appears that influenza is transmitted by both large and small droplets (ie, transmission occurs through both droplet and airborne routes). (Judson 2019) However, although airborne transmission is possible, large droplet or contact transmission is probably responsible for the vast majority of disease transmission.
Although some experts seem to doubt that influenza can be spread through small droplets or airborne droplet nuclei, (Brankston 2007) there are multiple lines of evidence that support this hypothesis. Studies in ferrets showed that influenza spread even when the animals were separated by “S” and “U” shaped ducts that would not allow for the passage of larger droplets, indicating “that infection was conveyed either by droplet-nuclei or very fine dust particles.” (Andrewes 1941) Likewise, in studies of mice, lower ventilation rates led to higher transmission rates, leading the authors to conclude spread must be by airborne droplet nuclei. (Shulman 1962) There are numerous other animal studies demonstrating the spread of influenza uphill (against gravity) over distances longer than droplets are supposed to travel, strongly supporting the conclusion of airborne spread. (Tellier 2009)
Influenza RNA has been detected in aerosol particles from infected patients while just breathing comfortably. (Fabian 2008) Influenza has been found in aerosols in random samples of air around an emergency department during flu season. (Blachere 2009) In one study that tested the air in an emergency department during flu season, influenza was identified in 43% of the samples taken. The total amount of virus found on samplers worn by healthcare providers was about twice that in the air, suggesting that the risk is still highest from close contact with patients, but that airborne spread is clearly possible. (Rule 2018) In another study, total viral load in air samples was higher outside patients’ rooms than right next to the patients. (Cummings 2014) On the other hand, Bischoff (2013) did find higher viral loads closer to the patient, but virus was still detected 6 feet or 2 meters away. It has also been proven that humans can develop influenza after breathing air artificially contaminated by the virus. (Francis 1944) (And I just have to point out that Jonas Salk is one of the authors on this paper!) The question is how often this occurs in a real world setting.
The TCID50, or the concentration of virus particles at which 50% of cells become infected, has been estimated to be as low as 3 for some strains of influenza A. (Thompson 2013) Assuming a respiratory rate of 10 L/min, during a 10 minute visit to a patient room a healthcare worker will breath 100 L of air. At baseline, one study found 7,690 viral particles per L of air in an influenza patient’s room. Therefore, in a 10 minute visit, the health care provider would have inhaled 769,000 viral particles, which is clearly above the TCID50. (Thompson 2013) Even studies that find lower viral counts in the air (approx 300 in Rule 2018) will still be well above this threshold.
There is indirect evidence that airborne transmission occurs, as good ventilation and UV irradiation limits influenza transmission. (McLean 1961; Shulman 1962; Drink 1996; Fiegel 2006; Tellier 2009) There are also multiple influenza outbreaks where airborne spread is hypothesized as the best explanation, however it is impossible to know retrospectively. (Moser 1979; Klontz 1989; Davis 2009) There is the interesting case report of an outbreak on a plane in Alaska in 1977. Because of a mechanical failure, there was a 4.5 hour delay with the ventilation turned off. 1 person was sick at the time of the flight, but over the next 3 days 38 others (72% of the people on the plane) developed influenza A. The size of the plane seems to make airborne transmission much more likely than large droplets, which we are told should not spread beyond 1-2 meters. That being said, if the index patient was the first person to use the washroom, the outbreak could easily be explained by droplet spread. (Moser 1979)
I think the data is pretty clear that influenza can spread through airborne aerosols, and I find that fact reassuring in the era of COVID-19. We generally treat influenza in “droplet precautions”, and transmission to healthcare workers is generally low. (Although the analogy fails because vaccination and prior exposure to influenza provide a level of immunity that does not exist with COVID-19). Even when a virus can be spread through airborne transmission, you are still much more likely to become ill as the result of close contact. If COVID-19 is transmitted similarly to influenza, we can be somewhat reassured by our current practices.
Some faulty epidemiologic reasoning
Many people dismiss airborne spread for any disease that doesn’t behave like measles or tuberculosis. They suggest that airborne must equate to long distance transmission. They suggest that a low R0 and the lack of large scale outbreaks proves that airborne spread is impossible. I think that is a mistake.
I think the animal studies above make it pretty clear that influenza can spread by the airborne route. This would provide direct evidence against those epidemiologic arguments. Influenza has a low R0. It occasionally causes large scale outbreaks (some of which have been blamed on airborne transmission), but those outbreaks are rare. It is hard to know exactly how people get sick, but we don’t routinely see influenza spread of long distances. Thus, the epidemiologic argument that “the R0 of this disease is too low for it to be airborne” doesn’t hold water. Any infection that behaves like influenza could easily be spread through aerosols.
Aerosols are tiny and their concentration drops off exponentially as you get farther from the source (especially with good ventilation). Of course we don’t frequently see transmission over large distances or large scale outbreaks. The chances of encountering viable virus across the room are just too lw.
However, that line of reasoning completely discounts close range aerosol spread. Aerosols will be most concentrated within a few meters of the patient. At that distance, aerosol spread is almost indistinguishable from droplet spread. In fact, it is generally completely ignored, because many people just assume that short range spread is due to droplets. However, short range aerosol spread would have significant implications for our PPE choices.
This short range aerosol spread is exactly what we are talking about when we discuss aerosol generating procedures. It isn’t the nurse 3 rooms down that gets sick (usually). It is the people in the room that are exposed to aerosols. However, as we discussed above, normal human activities like talking and coughing produce just as many aerosols as most of our aerosol generating procedures. Therefore, it is important to consider short range aerosol spread in order to appropriate protect ourselves.
Coronaviruses: droplets or airborne?
I don’t think we can say definitively, but it is highly likely that COVID-19 can be spread through airborne aerosols. Both SARS and MERS were thought to spread primarily by large droplets, but there were also outbreaks that were best explained by airborne spread of the disease (and others in which aerosols were thought possible, even if they weren’t highly likely). (Wong 2004; Li 2004; Morawska 2006; Xie 2007; Judson 2019) SARS was contracted by a nurse that never entered a patient’s room, which could be explained by airborne transmission, but could also have been through fomites. (Scales 2003) In a retrospective analysis out of Singapore, insufficient ventilation on hospital wards was one of 5 major factors that increased the risk of transmission of SARS. (Chen 2009) Although the evidence isn’t definitive, the pattern of nosocomial spread followed hospital ventilation patterns, rather than the random distribution you would expect if the infection was spread via surfaces.
An outbreak of SARS that affected more than 300 people across 150 apartments in the Amoy Garden apartment complex in Hong Kong is thought to have resulted from airborne spread of aerosols through the sewer system. Rather than the random distribution that you might expect from contact or droplets spread through common areas, residents on higher floors were more likely to be infected, “consistent with a plume of contaminated warm air”. (Morawska 2006)
It is also pretty clear that these viruses have been spread as the result of aerosol generating procedures. There was a strong association between multiple aerosol generating procedures and transmission of SARS to healthcare workers. (Tran 2012)
For COVID-19, the virus has been found in the air more than 6 feet away from the patient, in ventilation systems, and even in the air in hallways outside patients’ rooms, indicating the potential for airborne spread. (Santarpia 2020 preprint data; Ong 2020, Liu 2020) Guo (2020) found virus RNA in the air up to 4 meters from the patient. However, the presence of RNA doesn’t mean that there is viable virus, nor that it was present in large enough numbers to cause clinical infection. That being said, if COVID is aerosolized in large volumes, it is likely that the virus remains viable for at least 3-5 hours, and maybe much longer. (Van Doremalen 2020; Fears 2020)
There is definitely debate on this point. Some organizations have stated very strongly that SARS-CoV-2 is not spread by the airborne route. However, others say the opposite. For example, the CDC guidance for coronaviruses has always been to treat them as airborne, although that is based more on the precautionary principle than hard science (see here and here). Furthermore, the National Academies of Sciences, Engineering, and Medicine states that “while the current SARS-CoV-2 specific research is limited, the results of available studies are consistent with aerosolization of virus from normal breathing.” (Fineberg 2020)
At this point, I think the only safe conclusion is that airborne transmission is possible. However, that doesn’t make it likely. Because of their larger size, large droplets contain as much as 99.9% of viral particles exhaled. Although aerosols may carry small amounts of virus, they become very diffuse the further you are from the patient and are effectively managed by modern ventilation systems. I don’t think we should be making black and white statements. We need to consider the potential for aerosol spread, and how that might impact our PPE practices, while simultaneously recognizing that droplets and close contact with patients represent a far greater risk.
Update: It is becoming increasingly clear that there is significant pre-symptomatic spread of COVID-19. When discussing this issue on the Saint Emlyn’s podcast, professor of medical virology Pam Vallely made the interesting point that presymptomatic spread is further evidence of aerosol spread, as large droplets aren’t formed in any volume until you are symptomatic.
A few infection control notes
Managing aerosols
One of the most important aspects of managing bioaerosols is good ventilation. (Fiegel 2006) In ideal circumstances, 65% of all airborne droplets can be removed with each air exchange, although because air doesn’t mix perfectly, the number is probably in the 20-60% range in real life. (Fiegel 2006) In medicine, we are used to thinking in half lives. Each air exchange might take away half of the aerosols in a room, and therefore, if you can determine the air exchange rate for your facility, you can estimate the half life of aerosols, and use that to make PPE and clinical decisions.
You can also disinfect air using a number of different systems, such as HEPA filters and UV light. (Fiegel 2006) I wonder if anyone is using portable HEPA air purifiers in hallways to limit airborne spread of COVID? And of course, the most important mechanism for managing aerosols is almost certainly PPE, with a properly fit N95 mask being the medical standard, which I will discuss further below. (Fiegel 2006)
Is there evidence for the “2 meter rule”?
There is a widely spread infection control concept that as long as you are 2 meters away from the patient, you are safe from droplets. This claim is usually made without citation, and there is plenty of data to say that it is wrong, at least as a definitive cut off. The idea that all large droplets will fall to the floor within 2 meters seems to have been initially proposed by Wells, based on a very simplistic calculation, with assumptions that have since been questioned, and limited empirical data. (Xie 2007) Unfortunately, as is reviewed above, most of the existing data seems to refute that hypothesis. For example, one recent study had 5 volunteers cough after gargling with food colouring, and there was visible macroscopic contamination beyond 2 meters with 4 of 5 participants. (Loh 2020) Simple pictures of sneezes show a droplet cloud out to 8 meters. (Bourouiba 2020) In another study, in the absence of any aerosol generating procedures, influenza viral loads were actually higher further away from the patient, and they were highest outside the patient’s room. (Cummings 2014)
We should not rely on the 2 meter rule to keep us perfectly safe. That being said, because droplets spread through 3 dimensional space, the concentration of droplets decreases exponentially as you get further from the patient, and there is data that the majority of droplets created from normal breathing fall within 1 meter, although coughing and sneezing increase that distribution significantly.
Overall, the further you are from the patient the safer you are. You are more likely to become contaminated at 50 cm than you are at 1 meter. Your risk is lower again at 2 meters, but it doesn’t drop to zero. You are even safer 4 or 8 meters away from the patient (or even better, behind a closed door).
Practically speaking, this means that you should take off your PPE as far from the patient as possible. In an ideal world, you would always take your PPE off behind a screen or door to completely limit droplet contamination. However, although increasing the distance will decrease your risk from droplets, it actually increases the risk of contact spread. Clearly, you don’t want to bring dirty PPE into clean hallways. The risk of spread through contact with fomites is almost certainly higher than the risk from droplets once you are further than 2 meters away from the patient, which is why the 2 meter rule often works practically, even though it is not scientifically accurate.
What this means clinically will depend a great deal on the layout of your own space. If there is an empty anteroom to doff in, that makes the most sense. If you can doff behind a curtain, that would be great. Otherwise, realize that your risk is very small beyond that 2 meter mark as long as the patient is wearing a mask, not actively coughing or sneezing, and there is not an ongoing aerosol generating procedure.
Update: A new systematic review examined this topic, and 8 of the 10 studies included demonstrated droplet spread beyond 2 meters. The authors state, “although the studies employed very different methodologies and should be interpreted cautiously, they still confirm that the spatial separation limit of 1 m (≈3 ft) prescribed for droplet precautions, and associated recommendations for staff at ports of entry [10], are not based on current scientific evidence.” (Bahl 2020)
Comparing N95 and surgical masks
We actually use masks for 2 different purposes and it results in a common misunderstanding among the lay public. We can use masks to keep droplets out of the respiratory tract (to keep ourselves safe), but we can also use masks to keep droplets in (to keep others safe). The surgical mask is significantly less effective than the N95 at keeping particles out, but it is very good at keeping particles in. (It’s primary purpose is to protect patients from the surgeon during surgery). With coughing and sneezing patients in the hospital, one of the most important infection control strategies is placing surgical masks on the patients to limit the number of droplets then make it to the environment. (This is also one of the reasons that “aerosol generating procedures” are higher risk – because we generally need to remove that primary layer of protection.) Similarly, when hospitals are asking employees to wear surgical masks at all times right now, it is not a strategy designed primarily to protect employees, but to limit unintentional spread from asymptomatic or minimally symptomatic individuals.
There are a few studies that compare N95 and surgical masks in healthcare workers. (Loeb 2009; MacIntyre 2013; Smith 2016; Radonovich 2019) All were looking at influenza, so will only extrapolate to COVID-19 if the mechanism of spread is the same, which might not be a good assumption. Similarly, all studies will be impacted by the rate of compliance with the mask (as well as things like hand hygiene). In general, compliance is lower with the less comfortable N95 masks, so the studies may be biased to show no difference, even if there is a difference with perfect mask use. Studies done in an outpatient setting may not extrapolate well to critical care. Finally, although the studies contain what look like large numbers of people, the power of the studies comes from the event rate (or the number of people who get sick despite wearing a mask), which is much lower, and so the confidence intervals are very large. A systematic review and meta-analysis on this topic found no statistical differences, but the point estimates are all on the side of N95s being better, and the confidence intervals are huge. (Long 2020) Therefore, I don’t think it is fair to conclude that the two masks are equivalent, but just that we don’t know. It is hard to know what to do with that information. In an ideal world, I think using N95s as the standard until surgical masks were proven to be non-inferior makes the most sense, but that only works if we have an adequate supply of N95s to use for all COVID-19 encounters.
Summary
This is a lot of information, and unfortunately it does not allow for any black and white conclusions. There is pretty wide consensus that the science surrounding aerosol transmission of disease is severely lacking. (Morawska 2006; Chen 2010; Judson 2019) There are more questions than there are answers. We should avoid making definitive statements, and instead discuss the uncertainties and the trade-offs between alternating risks. Overall, given the lack of solid evidence, it is generally recommended that we rely on the “precautionary principle”. (Judson 2019) In other words, we should not be looking for evidence that a practice is harmful before avoiding it, but should instead be looking for evidence that a practice is safe before adopting it.
Based on this data, it doesn’t make sense to dichotomize into just airborne aerosols and localized droplets. It is clearly far more complicated than that, with larger droplets becoming smaller as they evaporate, and plenty of evidence that virus can be found further from patients than our current models predict. This literature also makes it clear that almost every activity, including normal breathing, can create aerosols. However, the risk from those aerosols is far lower than the risk of droplets and close contact with the patient.
Perhaps most importantly, we need to move beyond black and white statements and think in terms of probabilities. This data disproves definitive rules, such as “you are perfectly safe when 2 meters away from the patient”. Instead, it tells us that the chance of infection is much higher when close to the patient and much lower as we get further away.
We need to distinguish between possible and likely. Airborne transmission of influenza and COVID-19 is clearly possible, and probably does occur occasionally, but we also have to acknowledge that it is very rare. How can we know that it is rare? If airborne transmission was highly likely, we would see much bigger outbreaks. There have been thousands of COVID patients managed in normal hospital rooms, or behind curtains, and not every person in that department gets sick. Similarly, there have been many sick COVID patients on planes, and although there is some transmission, most people are fine. I think that message is key. Airborne spread is possible, but if there was a COVID patient coughing without a mask on the other side of the department, it is still very unlikely you will actually catch the disease, even if you aren’t wearing PPE. You are much more likely to catch it from droplets or close contact, which is why infection control practices are so focused on those activities.
If you are a numbers person, people have done some calculations. There are a lot of assumptions, but the best estimates are that if you spend 15 minutes in a room with a coughing patient, your chance of catching influenza from large droplets and self inoculation (contact) is about the same (and not very high). Transmission through airborne aerosols is about 100 to 1000 times less likely than the other two routes (Telllier 2009)
That is reassuring. However, it is a mistake to take that line of reasoning too far. Just because droplet spread is more likely, doesn’t mean that airborne spread should be ignored. It is wrong to categorically say that COVID does not spread through an airborne route.
The focus should be on droplet and contact spread. At the same time, we should not ignore the airborne route. The above science review gives hints at activities that could increase airborne transmission: sicker patients with higher viral loads, more coughing and sneezing, higher respiratory rates, longer times spent with the patient, and of course aerosol generating procedures. In these cases, the risk of airborne transmission increases, and we should consider adding airborne precautions to our standard of contact and droplet PPE.
Unfortunately, at this point I am not sure we understand the concept of “super spreaders” well enough. It is clear they exist. I think the above review explains their existence: some people produce far more aerosols than others, and if those same patients have high viral loads, you have an infection control problem. The issue is we don’t know how to identify these patients, nor do we know how to appropriately account for them in our current infection control practices. In my mind, their existence is probably the best argument for universal mask use during an outbreak.
I have said many times that the goal of every hospital during COVID-19 should be to ensure that ZERO healthcare workers become infected in the course of their normal duties, while still providing exemplary care to all of our patients. However, that goal may not be perfectly attainable. There are always tradeoffs between risks. Removing your PPE further from the patient may limit your exposure to droplets, but increases potential exposure to fomites as we carry dirty PPE further from the source. The small risk of airborne transmission might suggest increased use of N95 masks, but if we use our equipment in low risk scenarios it might not be available for us in higher risk encounters. You might suggest wearing an N95 at all times, but we have already seen providers suffering from skin breakdown and other complications.
There are no easy answers. If N95s were plentiful, I think if you make sense to wear them for all encounters with suspected COVID patients. However, that is not the world we live in, and although airborne spread is technically possible, it is incredibly unlikely. I am happy to wear a surgical mask when assessing the average patient with respiratory complaints. I think that will keep me close to 100% protected. But as the patient gets sicker and the risk of aerosols increases (either through procedures or natural activities like coughing), I will switch to an N95.
Other FOAMed and Reporting
Don’t Forget the Bubbles: AEROSOL GENERATING PROCEDURES
Epidemic podcast: A False Dichotomy: Airborne versus Droplet
COVID-19: Why We Should All Wear Masks — There Is New Scientific Rationale
Is the coronavirus airborne? Experts can’t agree
Perspective: Universal Masking in Hospitals in the Covid-19 Era
You can watch aerosol being created by talking in this Japanese news program:
References
Andrewes CH and Glover RE. Spread of Infection from the Respiratory Tract of the Ferret. I. Transmission of Influenza A Virus. Br J Exp Pathol. 1941 Apr; 22(2): 91–97 PMC2065394
Asadi S, Wexler AS, Cappa CD, Barreda S, Bouvier NM, Ristenpart WD. Aerosol emission and superemission during human speech increase with voice loudness. Sci Rep. 2019;9(1):2348. Published 2019 Feb 20. doi:10.1038/s41598-019-38808-z PMID: 30787335
Bahl P, Doolan C, de Silva C, Chughtai AA, Bourouiba L, MacIntyre CR. Airborne or droplet precautions for health workers treating COVID-19? [published online ahead of print, 2020 Apr 16]. J Infect Dis. 2020;jiaa189. doi:10.1093/infdis/jiaa189 PMID: 32301491 [article]
Bischoff WE, Swett K, Leng I, Peters TR. Exposure to influenza virus aerosols during routine patient care. J Infect Dis. 2013;207(7):1037–1046. doi:10.1093/infdis/jis773 PMID: 23372182
Blachere FM, Lindsley WG, Pearce TA, et al. Measurement of airborne influenza virus in a hospital emergency department. Clin Infect Dis. 2009;48(4):438–440. doi:10.1086/596478 PMID: 19133798
Bourouiba L. Turbulent Gas Clouds and Respiratory Pathogen Emissions: Potential Implications for Reducing Transmission of COVID-19 [published online ahead of print, 2020 Mar 26]. JAMA. 2020;10.1001/jama.2020.4756. doi:10.1001/jama.2020.4756 PMID: 32215590
Brankston G, Gitterman L, Hirji Z, Lemieux C, Gardam M. Transmission of influenza A in human beings. Lancet Infect Dis. 2007;7(4):257–265. doi:10.1016/S1473-3099(07)70029-4 PMID: 17376383
Chen WQ, Ling WH, Lu CY, et al. Which preventive measures might protect health care workers from SARS?. BMC Public Health. 2009;9:81. Published 2009 Mar 13. doi:10.1186/1471-2458-9-81 PMID: 19284644
Chen C, Zhao B. Some questions on dispersion of human exhaled droplets in ventilation room: answers from numerical investigation. Indoor Air. 2010;20(2):95–111. doi:10.1111/j.1600-0668.2009.00626.x PMID: 20002792
Cummings KJ, Martin SB Jr, Lindsley WG, et al. Exposure to influenza virus aerosols in the hospital setting: is routine patient care an aerosol generating procedure?. J Infect Dis. 2014;210(3):504–505. doi:10.1093/infdis/jiu127 PMID: 24596280
Davis J, Garner MG, East IJ. Analysis of local spread of equine influenza in the Park Ridge region of Queensland. Transbound Emerg Dis. 2009;56(1-2):31–38. doi:10.1111/j.1865-1682.2008.01060.x PMID: 19200296
Drinka PJ, Krause P, Schilling M, Miller BA, Shult P, Gravenstein S. Report of an outbreak: nursing home architecture and influenza-A attack rates. J Am Geriatr Soc. 1996;44(8):910–913. doi:10.1111/j.1532-5415.1996.tb01859.x PMID: 8708299
Fabian P, McDevitt JJ, DeHaan WH, et al. Influenza virus in human exhaled breath: an observational study. PLoS One. 2008;3(7):e2691. Published 2008 Jul 16. doi:10.1371/journal.pone.0002691 PMID: 18628983
Fears SC, Klimstra WB, Duprex P, Hartman A, Weaver SC, Plante KS, et al. Persistence of severe acute respiratory syndrome coronavirus 2 in aerosol suspensions. Emerg Infect Dis. 2020 Sep. https://doi.org/10.3201/eid2609.201806
Fiegel J, Clarke R, Edwards DA. Airborne infectious disease and the suppression of pulmonary bioaerosols. Drug Discov Today. 2006;11(1-2):51–57. doi:10.1016/S1359-6446(05)03687-1 PMID: 16478691
Fineberg HV. Rapid Expert Consultation on the Possibility of Bioaerosol Spread of SARS-CoV-2 for the COVID-19 Pandemic (April 1, 2020) Washington, D.C.. National Academies Press; 2020. https://doi.org/10.17226/25769
Francis T, Pearson HE, Salk JE, Brown PN. Immunity in Human Subjects Artificially Infected with Influenza Virus, Type B. American journal of public health and the nation’s health. 1944; 34(4):317-34. [pubmed]
Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and Surface Distribution of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospital Wards, Wuhan, China, 2020 [published online ahead of print, 2020 Apr 10]. Emerg Infect Dis. 2020;26(7):10.3201/eid2607.200885. doi:10.3201/eid2607.200885 PMID: 32275497
Hui DS, Chan MT, Chow B. Aerosol dispersion during various respiratory therapies: a risk assessment model of nosocomial infection to health care workers. Hong Kong Med J. 2014;20 Suppl 4:9–13. PMID: 25224111
Judson SD, Munster VJ. Nosocomial Transmission of Emerging Viruses via Aerosol-Generating Medical Procedures. Viruses. 2019;11(10):940. Published 2019 Oct 12. doi:10.3390/v11100940 PMID: 31614743
Li Y, Huang X, Yu ITS, Wong TW, Qian H. Role of air distribution in SARS transmission during the largest nosocomial outbreak in Hong Kong Indoor Air. 2005; 15(2):83-95.
Liu Y, Yu ZN, et al. Aerodynamic Characteristics and RNA Concentration of SARS-CoV-2 Aerosol in Wuhan Hospitals during COVID-19 Outbreak. 2020. Preprint, not peer reviewed, here.
Loeb M, Dafoe N, Mahony J, et al. Surgical mask vs N95 respirator for preventing influenza among health care workers: a randomized trial. JAMA. 2009;302(17):1865–1871. doi:10.1001/jama.2009.1466 PMID: 19797474
Loh NW, Tan Y, Taculod J, et al. The impact of high-flow nasal cannula (HFNC) on coughing distance: implications on its use during the novel coronavirus disease outbreak [published online ahead of print, 2020 Mar 18]. Can J Anaesth. 2020;1–2. doi:10.1007/s12630-020-01634-3 PMID: 32189218
Long Y, Hu T, Liu L, et al. Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta‐analysis J Evid Based Med.. 2020
MacIntyre CR, Wang Q, Seale H, et al. A randomized clinical trial of three options for N95 respirators and medical masks in health workers. Am J Respir Crit CareMed. 2013;187(9):960-966.
McLean RL. The eff ect of ultraviolet radiation upon the transmission of epidemic infl uenza in long-term hospital patients. Am Rev Respir Dis 1961; 83: 36.
Morawska L. Droplet fate in indoor environments, or can we prevent the spread of infection?. Indoor Air. 2006;16(5):335–347. doi:10.1111/j.1600-0668.2006.00432.x PMID: 16948710
Moser MR, Bender TR, Margolis HS, Noble GR, Kendal AP, Ritter DG. An outbreak of influenza aboard a commercial airliner. Am J Epidemiol. 1979;110(1):1–6. doi:10.1093/oxfordjournals.aje.a112781 PMID: 463858
Nicas M, Nazaroff WW, Hubbard A. Toward understanding the risk of secondary airborne infection: emission of respirable pathogens. J Occup Environ Hyg. 2005;2(3):143–154. doi:10.1080/15459620590918466 PMID: 15764538
Ong SWX, Tan YK, Chia PY, et al. Air, Surface Environmental, and Personal Protective Equipment Contamination by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) From a Symptomatic Patient JAMA. 2020
Papineni RS, Rosenthal FS. The size distribution of droplets in the exhaled breath of healthy human subjects. J Aerosol Med. 1997;10(2):105–116. doi:10.1089/jam.1997.10.105 PMID: 10168531
Radonovich LJ Jr, Simberkoff MS, Bessesen MT, et al. N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial. JAMA. 2019;322(9):824–833. doi:10.1001/jama.2019.11645 PMID: 31479137
Rule AM, Apau O, Ahrenholz SH, et al. Healthcare personnel exposure in an emergency department during influenza season PLoS ONE. 2018; 13(8):e0203223-. [article]
Santarpia JL, Rivera DN, et al. Transmission Potential of SARS-CoV-2 in Viral Shedding Observed at the University of Nebraska Medical Center. 2020. Preprint here.
Scales DC, Green K, Chan AK, et al. Illness in intensive care staff after brief exposure to severe acute respiratory syndrome. Emerg Infect Dis. 2003;9(10):1205–1210. doi:10.3201/eid0910.030525 PMID: 14609453
SCHULMAN JL, KILBOURNE ED. Airborne transmission of influenza virus infection in mice. Nature. 1962;195:1129–1130. doi:10.1038/1951129a0 PMID: 13909471
Simonds AK, Hanak A, Chatwin M, et al. Evaluation of droplet dispersion during non-invasive ventilation, oxygen therapy, nebuliser treatment and chest physiotherapy in clinical practice: implications for management of pandemic influenza and other airborne infections. Health Technol Assess. 2010;14(46):131–172. doi:10.3310/hta14460-02 PMID: 20923611
Smith JD, MacDougall CC, Johnstone J, Copes RA, Schwartz B, Garber GE. Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis. CMAJ. 2016;188(8):567–574. doi:10.1503/cmaj.150835 PMID: 26952529
Tellier R. Aerosol transmission of influenza A virus: a review of new studies. J R Soc Interface. 2009;6 Suppl 6(Suppl 6):S783–S790. doi:10.1098/rsif.2009.0302.focus PMID: 19773292
Thompson KA, Pappachan JV, Bennett AM, et al. Influenza aerosols in UK hospitals during the H1N1 (2009) pandemic–the risk of aerosol generation during medical procedures. PLoS One. 2013;8(2):e56278. doi:10.1371/journal.pone.0056278 PMID: 23418548
Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. PMID: 22563403
Wong TW, Lee CK, Tam W, et al. Cluster of SARS among medical students exposed to single patient, Hong Kong. Emerg Infect Dis. 2004;10(2):269–276. doi:10.3201/eid1002.030452 PMID: 15030696
Xie X, Li Y, Chwang AT, Ho PL, Seto WH. How far droplets can move in indoor environments–revisiting the Wells evaporation-falling curve. Indoor Air. 2007;17(3):211–225. doi:10.1111/j.1600-0668.2007.00469.x PMID: 17542834
Morgenstern, J. Aerosols, Droplets, and Airborne Spread: Everything you could possibly want to know, First10EM, April 6, 2020. Available at:
https://doi.org/10.51684/FIRS.17317



78 thoughts on “Aerosols, Droplets, and Airborne Spread: Everything you could possibly want to know”
Hi
Thanks for your paper. what is the source of your statement: “Because of their larger size, large droplets contain as much as 99.9% of viral particles exhaled.” please? I note https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3591312/pdf/ppat.1003205.pdf which finds more influenza virus in exhaled fine droplets than large and this paper https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3331822/pdf/12890_2011_Article_304.pdf which in a cough finds very small droplets predominate. It is a baffling area for sure!
Thanks
John Ferguson
It is a is a simple volume issue. Definitely virus in the smaller particles, but the large ones are a much bigger total volume.
From the post: “It is also important to understand that although the majority of the droplets produced by a cough may be small enough to stay airborne, their small size means that collectively they add up to only a tiny fraction of the volume produced (perhaps less than 0.1%), and therefore only a tiny fraction of the total virus spread. (Nicas 2005)”
Very nice article, learned a lot. Only one point .. the quoted study as concentration of influenza virus was higher outside the room has an explanation in it. They say that some other source of the influenza virus couldn’t be excluded.
I am not sure that “couldn’t exclude” is that same has having an explanation. It certainly adds some uncertainty, but that is true of all science.
Whatever the source, it is clear that influenza can be found in airborne aerosols, and the animal studies make it clear that it can be transmitted through the airborne route as well. In my mind the question is not as much can this happen, but more how often does this happen, and it seems like droplet spread still outweighs airborne spread in most practical settings.
Thank you. A very clear unbiased opinion – based on the available literature, from someone in the trenches. I learned a lot.
I’m an orthodontist. The dental community is very concerned and confused about the various recommendations for protecting our patients, our staffs, and ourselves during this pandemic. We are concerned about asymptomatic transmission in aerosols produced during dental procedures. Many of our offices will have been closed for 2 months+ when we resume work and if we haven’t contracted COVID-19 yet and then do, we will have to shut down for another 2-3 weeks in the best case scenario of consequences. Based on your research would you have any specific insights or takeaways that apply to dental offices? How about large volume, open bay practices like orthodontic offices? Would medical grade HEPA filters make a significant difference in transmission? Any other best practices you’d recommend in this setting? Thanks so much for such an informative and unbiased article.
I wish I had specific answers to your questions. I have received many similar questions from dentists, and the most honest answer I can provide is I don’t know.
Unfortunately, working in the mouth is likely high risk for disease transmission, but it is also really important work. I tried to include everything I came across in this write up so hopefully people can apply the science to their own practices, but the science is far from perfect. The risk will probably depend a lot on the specifics of procedures being done (drilling, spraying water into the mouth, and suctioning all probably have a high risk of transmission). I honestly don’t know enough about oral surgery or dentistry to say specifically, but my guess is it probably requires full airborne type PPE for many/most procedures, and full cleaning procedures between patients.
Good luck and stay safe
The stand out best article I have read on this critical topic. Outstanding work
Hi Justin,
Thank you for the time you put into researching and assembling this.
Intuitively it doesn’t seem like normal breathing should produce much in the way of droplets since it involves a pretty low-velocity airflow through a fairly unrestricted passage. Since the air we exhale is warm and humid, I wonder if a lot of the very small droplets observed to result from breathing might actually be condensate that forms after the air leaves the body and cools. It seems like this difference would matter since if the water in the droplets was in gas phase until it left the body, the droplets could not contain any virus particles. Do you know if the research addressed this possibility?
Thanks again for the great article,
Paul
That is a fantastic question, and I didn’t see it addressed anywhere in the literature. Most of what I read said that a single normal breath makes very few aerosols (although the add up over time as we are always breathing), which might not fit well with your theory. Air flow is one component or aerosol generation, but surface tension is another. We specifically produce surfactant to lower surface tension, which will allow aerosols to form easier. even without significant air flows. But I honestly don’t know. (We can probably pretty definitively say that simple breathing is not making large quantities of infectious aerosols, because otherwise everyone would be sick by now – I have looked after many many COVID patients with just a surgical mask, and haven’t caught it yet, as far as I know.)
Thanks for a very useful article. It seems to explain easier transmission in winter as well: indoor relative humidity is much lower (big difference between outdoor and indoor temperature), so droplets of any size evaporate faster, so more droplets shrink to dry, light particles and survive in air.
Which doesn’t make me happy, because we’re reprising March at the moment in NJ. Below freezing where I am 2 nights ago.
Thank you for doing so much research and putting this information out to us laypeople in a way that is easier for us to understand than all the scientific papers out there. I have been trying to develop homemade masks that are both effective and comfortable to wear, and have been trying to figure out what size the droplets coming out of our mouths and noses might be. Some people suggest 2 layers of quilting cotton, but is that really enough to protect other people from the wearer? And what about protecting the wearer from someone who might not be wearing a mask, or is wearing a respirator with a valve in it, so their breath is coming out of that mask unfiltered? Am I correct in thinking that a mask that protects the wearer would need to be able to filter out smaller particles than a mask that protects everyone else from the wearer, because the droplets will evaporate through the air?
Also, what about Brownian motion and static electricity?
What are your thoughts on this study that was published on April 24? https://pubs.acs.org/doi/10.1021/acsnano.0c03252 News articles about it are saying that 1 layer of 600TPI cotton and 2 layers of the polyester/spandex chiffon they tested are almost as effective as an N95 mask if it fits well with no gaps, but trying to interpret the study myself is making me go cross-eyed. I think that’s what it actually says, but I know reporters often have a tendency to misunderstand scientific literature, and other reporters will just copy what the first reporters say. Also, if this is true, and if we were to put the sheer layers on the outside of the mask, would moisture build up in the cotton get the sheer fabric moist, eliminate the static, and render those sheer fabrics ineffective? And one last thing, since mixing negatively-charged materials with positively-charged materials is supposed to create static, wouldn’t it be more effective to use one layer of polyester/spandex chiffon with one layer of something like silk along with the layer of cotton, since they have opposite charges, instead of 2 layers of chiffon?
On a side note, the uppercase styling in a heading in one of your charts is making “Small (1-2 µm)” look like it says “SMALL (1-2 MM)”. If you have access to the HTML, you can add before the µm and after it.
Thanks again, for all you do! Be well, and stay safe!
The system ate my HTML tags. I was trying to say, the uppercase styling in a heading in one of your charts is making “Small (1-2 µm)” look like it says “SMALL (1-2 MM)”. If you have access to the HTML, you can add (span style=”text-transform:none;”) before the µm and (/span) after it, but change the parentheses to less-than and greater-than symbols.
Great summary.
How about https://www.pnas.org/content/early/2020/05/12/2006874117
The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission
Valentyn Stadnytskyi, Christina E. Bax, Adriaan Bax, and Philip Anfinrud
PNAS first published May 13, 2020 https://doi.org/10.1073/pnas.2006874117
Edited by Axel T. Brunger, Stanford University, Stanford, CA, and approved May 4, 2020 (received for review April 10, 2020)
Abstract
Speech droplets generated by asymptomatic carriers of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are increasingly considered to be a likely mode of disease transmission. Highly sensitive laser light scattering observations have revealed that loud speech can emit thousands of oral fluid droplets per second. In a closed, stagnant air environment, they disappear from the window of view with time constants in the range of 8 to 14 min, which corresponds to droplet nuclei of ca. 4 μm diameter, or 12- to 21-μm droplets prior to dehydration. These observations confirm that there is a substantial probability that normal speaking causes airborne virus transmission in confined environments.
Very good review. From an Aerosolphysicist and involveld in the field of Aerosolmedicine since 1980 just a few remarks:
1.) Pollen are not invisible and are as big as 20 – 200 µm.
2.) You are correct that there is no real cutoff particle size in the Aerosol Definition. Aerosol is a suspension of fine solid particles or liquid droplets in air or another gas. When Aerosol particles fall out of the gas in a few seconds, it is no longer an Aerosol particle. But not only the size, but also the shape, the densitiy and some other factors are responsible for beeing airborne.
3.) There is another important mechanism how aerosol particles are generated by breathing: They are produced in the deep lungs by reopening of collapsed small airways. This mechanism is described by several aerosolphysicists (Edwards, 2004; Gebhart, 1988; Bake, 2016 and 2019; Johnson, 2009; Schwarz, 2009 and 2013…..). Unfortunately, it is not very often mentioned. This mechanism produce ub to several hundred thousand particles per breath. And in that way is much more effcient than cough, sneeze, speaking….
4.) Taking all that into account it is very likely that the transmission via Aerosol is the major mechanism in the spread of COVID 19.
Thank you for you comment.
I agree, physically speaking, it would seem like aerosols play a huge role. However, based in the spread of disease, I would have a hard time labelling it “the major mechanism”. In hospitals, we don’t use protection against aerosols, even with patients with known COVID. We just use droplet/contact precautions. If aerosols were the major mechanism, I would think the Canadian health workforce would all have been sick by now. That being said, as we see more and more outbreaks among healthcare workers, we are going to have to strongly revaluate the role of aerosols and the PPE we use.
👍
Having an expertise in both dust & static electricity control & salon industry air quality, I find the suddenly ubiquitous implementation of plexiglass sneeze guards worrisome. These plexiglass shields are providing a false sense of security in preventing inhalation exposure to dust and microorganisms, including COVID19. And, their use may be unwittingly contributing to an unrecognized increased exposure source.
Plexiglass is an extremely non conductive material and has a high propensity to create and hold high static charges, especially after cleaning due to the friction created by simply wiping the surface during the cleaning process. The higher the static charge, the greater the likelihood of attracting airborne dust from greater distances. Airborne droplets are able to attach themselves to dust particles, which affect coronavirus by serving like vehicles to transport droplets further than they would be able to travel otherwise, and potentially entering the breathing zone of people in close proximity. If these plexiglass guards/shields are now here to stay and are going to be seen everywhere we go, it’s best to understand how to prevent static electricity build up on their surfaces. Feel free to contact me, should you have an interest in learning how to maintain dust & static free surfaces, helping to prevent airborne virus inhalation exposure.
I was just searching the internet, because I am supposing that a static charge imparted to plastic shields, would attract droplets, that being a good quality. Rather than floating around the shield and around the room, they would rest on the surface and begin to degrade.
Good Afternoon I am a Freshman on High School currently doing research on how far microbes travel in exhaled breath. My project is severely limited because I do not have access to a laboratory. I am positioning agar plates in front of me at distances of .3, .6 and .9 meters.and have CO2 sensors monitoring the CO2, HUMIDITY AND TEMP I will read from a book for a few minutes and then hopefully collect whatever microbes travel in my exhaled breath. I know there will be many flaws in my research, but I believe social distancing does not work. If there are any recommendations to help me on my research I would appreciate it. I truly enjoy reading all the research.
Thank you very much
Very Respectfully
Jonah
Hi Jonah
Sorry for the delay in responding.
First of all, I applaud you on your effort to study this question. I hope you learn a lot in the process.
I think you will run into some problems with this set up. The biggest is that almost all respiratory pathogens are viruses, whereas your agar plates will only demonstrate the presence of bacteria (and things like yeast). These microbes exist on completely different scales, and therefore travel different distances.
This is a very hard topic to study with basic equipment, but it is worth experimenting to learn about the process. One key thing to remember about the scientific process: we learn by trying to falsify. It is very easy to find evidence that seems to support our beliefs. (Look up confirmation bias.) The key when studying a topic is to ask yourself what you really believe, and then do everything in your power to try to prove yourself wrong. If you prove yourself wrong, you have learned something great. If you can’t prove yourself wrong, you can add a little more certainty to your prior belief.
Sorry I can’t be much help with the practical side, but I applaud your effort.
Best of luck,
Justin
Thanks for this amazing work!
Did you come across anything about exhaled cigarette smoke and whether it could be aerosolizing? I was trying to click around and found this article but had no idea how to interpret it in comparison to a normal exhalation https://aaqr.org/articles/aaqr-12-02-oa-0041.pdf
Hello!
I had to attend an interview today and did not have a face mask due to the nature of the interview. When I arrived at the building there were a couple of people but I was told the place had been very busy prior to my arrival. When I went to the interview room there was a plexiglass screen separating me from the two people interviewing me.
My main concern is weather i could be contaminated by a person who had been there before I arrived? I’m quite sure the interview room had been empty a minimum 30 minutes prior to my arrival, but I’m concerned that smaller aerosols could have remained in the rather stale air of such a small room. What is the likelihood of becoming sick from this?
I think if you read through the science above, you will find that although the risk is not zero, it is very very low and probably not worth worrying about, aside from the general precaution of not touching your face and being sure to wash your hands
Thank you for your fast reply!
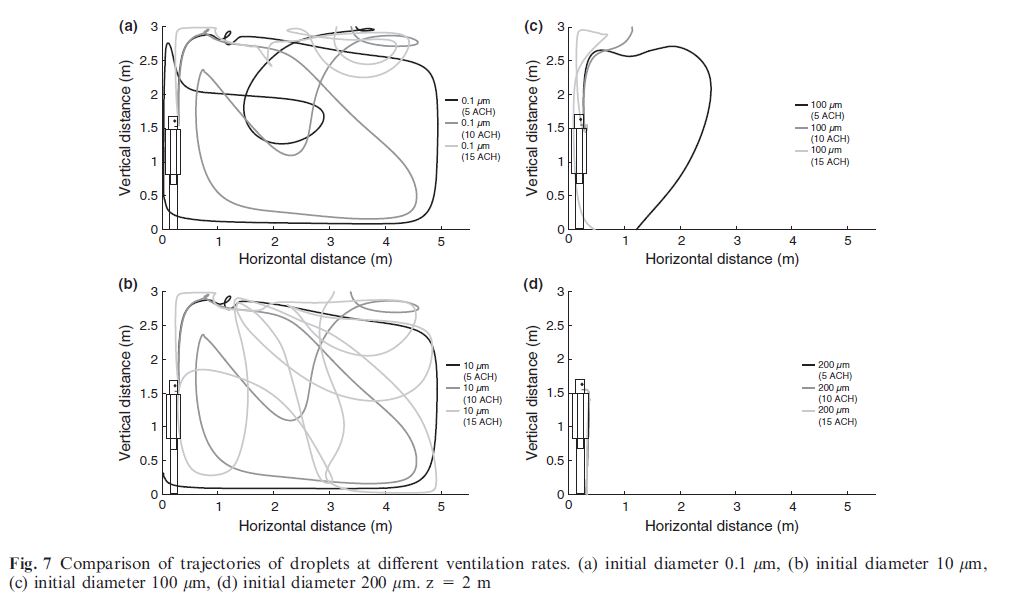
I read most of what you wrote, and found it especially interesting to see the paths of the smallest nuclei. But I think I was just seeking some reassurance.
Fantastic blog!
Absolutely – we are all feeling that way these days. I wish I could talk in absolutes, but everything we know is about grey areas. The more experience we get with COVID, though, the more it seems like the small droplet nuclei only have a small role in transmission. I would still be more concerned about the stuff everyone is talking about – masks, distancing, and hand washing.
Thanks for your article! One comment and one question.
Question: Do you think the seasonal nature of higher influenza (and maybe SAR-CoV-2 or other viruses/bacteria) levels in the winter might be related to the (typically) lower indoor relative humidity levels during that season? My thinking is that lower dewpoints/vapor pressures/relative humidity increases the evaporation rate on the surface of the airborne droplet. That in turn reduces the mean aerodynamic diameter of the droplets (evaporation occurs at a faster rate in the dry air than it would in more humid “summer” air). This global reduction in the droplet’s aerodynamic diameter creates a triple threat of: a. Deeper penetration into the lungs of each droplet. b. Longer suspension time in the air thereby increasing the probability the droplets become/stay airborne and c., (perhaps of less consequence), The concentration of virus has increased (the semi-spherical droplet has shrank but virus count stayed the same) thereby depositing more organisms per square micron at each landing site. Your comments/thoughts are appreciated!
Comment: HVAC design for critical spaces like O/R Theaters or Clean Room has general involved the near laminar flow of cooler/denser filtered air flowing vertically downward over the patient/occupants/hardware and then towards the floor where the “return” grilles are location and the air (and hopefully much of its contaminants) exits the room. It is typically then it is filtered, diluted with outside (“fresh”) air, sometimes treated with UVC or bipolar-ionization, heated/cooled/dehumidified and or humidified and returned to the space. Adopting this HVAC “architecture” to additional applications would be expensive but I suspect very helpful in mitigating airborne transmission.
My understanding is that the increased transmission in the winter is simply from prolonged time spent in contained spaces with sick people, but there may be a lot more to it than that. I haven’t seen anything directly written about humidity, but these other factors seem to make sense.
Thank you for your summaries and discussion.
I have added my comments already , however, don’t see it . Anyway. I have been preparing systematic review to find if covid-19 can transmit during oral and maxillofacial aerosols generating procedures.
So do you think dental generating procedures can spread the viruses in dental offices? And respirators are mandatory?
Sorry about that – I have been so busy, I fell way behind on the comments.
Honestly, I have not looked into dental procedures specifically. Drilling seems to produce aerosols, so I would assume these procedures would be very high risk, but I don’t have any data myself. Best of luck.
Thanks for such painstaking effort.
Thanks for all of this valuable information. I have a query. Is it plausible that cloth masks turn exhaled breath into finer clouds of aerosol? If the mask captures droplets but allows small particles to pass wouldn’t exhaling through a mask be a means of generating more aerosol from exhaled breath? Might it therefore do more harm than exhaling without wearing a mask?
Thanks for the question
1) I think this has been specifically looked at, and wearing a mask decreases the number of measurable aerosols.
2) Droplets are much much more important than aerosols in spreading most diseases, including COVID, so even if it was true, it would be irrelevant, and masks would still decrease overall transmission.
Thanks. The news has been full of headlines about aerosol transmission of Corona virus recently. I would love to see a study on the question of whether exhaling through a cloth mask creates more aerosol than exhaling without wearing a mask. Physical distancing alone could deal with droplet transmission.
I’ve been proved right about this for some types of face coverings. https://advances.sciencemag.org/content/early/2020/08/07/sciadv.abd3083.full
Ideas for experimentation– water molecules are slightly electrically polar. So maybe a mask with an electrostatic charge — a watch battery might be enough– would trap aerosols as well as droplets. Another idea– would a good sized dehumidifier in the vicinity of patients help– perhaps in conjunction with humidifiers strategically placed to maintain overall humidity balance.
“Perhaps most importantly, we need to move beyond black and white statements and think in terms of probabilities.” – LOL. The “quantum” approach.
Just wanted to say thanks for a great article. Very well written and easy to read but not at the expense of thoroughness!
As time pass by, the airborne route becomes more relevant than originally considered. The disproportionate amount of health workers with the disease – and deaths – means that even the best trained people wearing PPE are not safe in highly infected areas. We should focus on the airborne route even where everyone wears masks.
You mentioned UV light. We have a UV-C light that we can place in the room for added disinfection (not the far UV). Many staff members want the magic box put into the patient room after discharge to zap all the virus in the air. I don’t disagree but I don’t have any evidence and do not want to give a false sense of security. How much time or what dose of light, 5 minutes; 10 minutes?
At this point, I have not had the opportunity to look into the specifics of UV light. It is mentioned hear as a line of evidence of aerosol spread, and those specific are beyond the scope of this review. However, it is a topic that I think I will be writing about more in the near future.
Thank you for sharing this informative article on aerosols, droplets, and airborne spread. It’s clear that understanding these mechanisms is crucial, especially in the context of the COVID-19 pandemic. Your efforts to distill complex information into a comprehensible format are greatly appreciated, as they help healthcare workers and the public make informed decisions to ensure safety. Science and knowledge are indeed vital during these challenging times.
Thanks for sharing this insightful information.
Thank You