
I hope to get back to normal emergency medicine literature sometime soon, but for now there is enough new COVID-19 research that I think another COVID specific research roundup is worthwhile. In this edition, I will tackle some more evidence that COVID can be spread by the airborne route, some evidence of pre-symptomatic spread, evidence again the 2 meter rule, and a whole bunch more…
You can find the podcast version here, or just listen:
COVID is everywhere
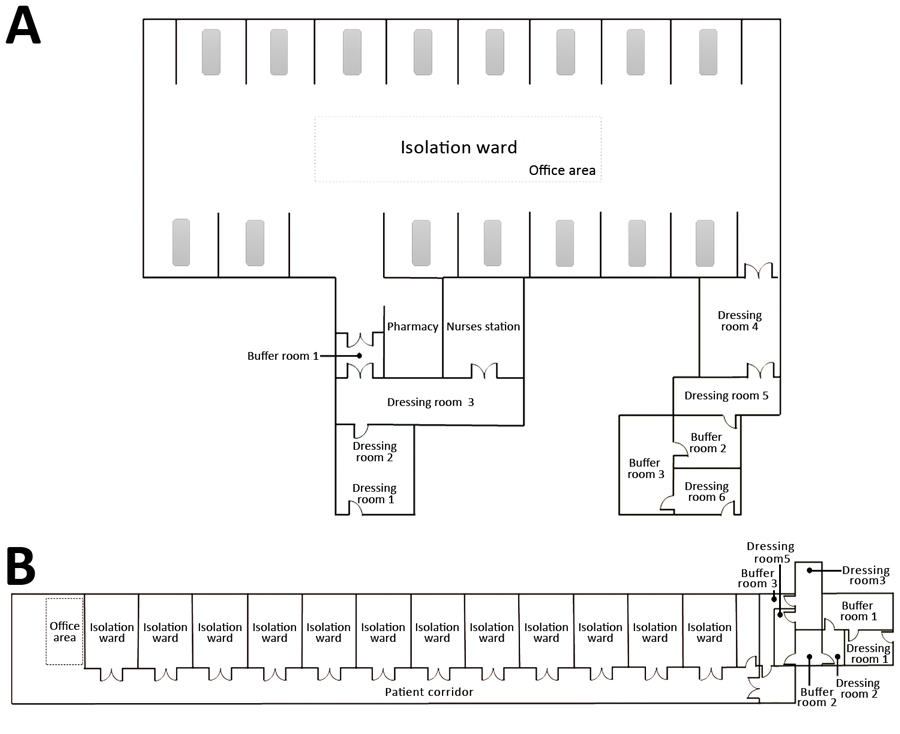
Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and Surface Distribution of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospital Wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26(7):10.3201/eid2607.200885. doi:10.3201/eid2607.200885 PMID: 32275497
This is an observational study from Wuhan that took swabs and air samples from 2 COVID units (one an ICU and 1 a general ward). You can read a more in depth summary here. In the general ward, only 1 swab outside of the patient area was positive – on a computer keyboard. For the most part, their clean areas remained clean, but they are much more strict about the division between clean and dirty areas than any emergency department I have ever seen (check the image). The exception was the floor of their dressing room. The floor and shoes are a general problem, including the floors in non-patient areas like the medication room in the ICU. Perhaps most importantly, this trial again suggests that COVID-19 could potentially be spread by airborne transmission, with most air outlet ducts testing positive, and COVID RNA being found in the air samples as much as 4 meters away from any patient room in the ICU. (We don’t know if this was viable virus, and we don’t have any details about what was happening with the patients at the time).
Bottom line: We need to be exceedingly careful about contact and droplet transmission. We probably need to be much more careful about our shoes and keeping our clean areas clean. Airborne transmission is still less likely, but I think the data continues to point to it being possible, so airborne precautions should be used with sicker patients (and probably all patients if we can ever get an adequate PPE supply.)
No symptoms, but still giving you COVID
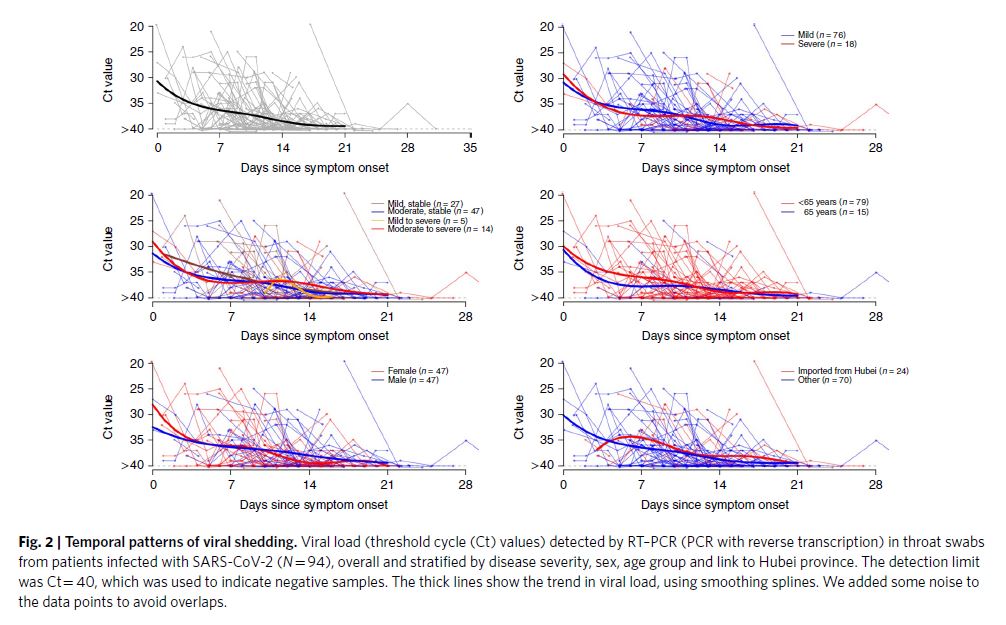
He X, Lau EHY, Wu P, et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med. 2020;10.1038/s41591-020-0869-5. doi:10.1038/s41591-020-0869-5 PMID: 32296168
This study looks at viral shedding and when patients might be most infectious. They took 414 swabs from 94 moderately ill admitted patients in China over about 1 month after symptom onset, and looked at the total amount of virus present. The amount of virus was highest on the first swab (soon after symptom onset), and slowly decreased over the next 3 weeks. I will say, however, that although they plot their data with a downward curve, the data points are really all over the place. It is not the cleanest data I have ever seen. Furthermore, they don’t seem to have a protocol that decided when patients were reswabbed, which could bias the results.
They also looked at a different data set of 77 pairs of patients, where one patient was thought to have given the disease to the other. Based on some modelling calculations, they say that infectiousness started 2.3 days before symptoms onset and peaked 0.7 days before symptoms onset. You can see from their figure that in many cases, the only time the patients spent together was before either displayed symptoms. One thing to keep in mind is that during an outbreak data will always be skewed towards showing presymptomatic spread, as symptomatic patients are aggressively isolated and so have much less opportunity to spread the disease.
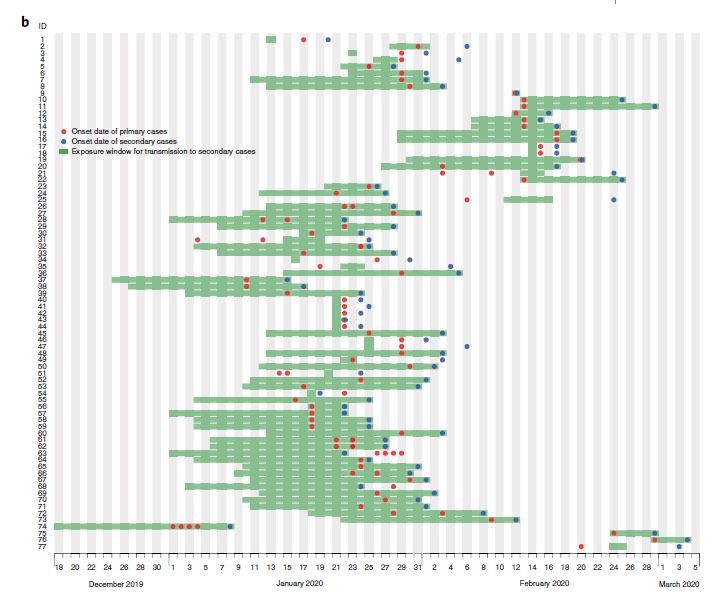
This has significant implications for our plans going forward. SARS-CoV-1 apparently didn’t peak in infectiousness until 7-10 days after symptoms onset, whereas SARS-CoV-2 seems to be acting more like influenza, with peak infectiousness just before symptom onset. A strategy of identifying patients through symptoms and isolating them at that point will be less effective if most infection is occurring before those symptoms develop. These authors state that a strategy of isolation and contact tracing will not be effective if more than 30% of transmission occurs before symptom onset unless more than 90% of contacts can be traced, which seems unrealistic with droplet spread while shopping at Costco. When presymptomatic spread is common, social distancing, universal masking, and hand hygiene become much more important infection control tools.
Bottom line: Patients seem to be infectious for a few days before symptoms develop. Universal precautions will be necessary, as we cannot effectively identify the patients that present the highest risk of transmission.
Droplets spread more than 2 meters
Bahl P, Doolan C, de Silva C, Chughtai AA, Bourouiba L, MacIntyre CR. Airborne or droplet precautions for health workers treating COVID-19? J Infect Dis. 2020;jiaa189. doi:10.1093/infdis/jiaa189 PMID: 32301491 [article]
All of a sudden, doctors around the world have become much more interested in seemingly childish questions, like how far does snot travel when you sneeze? This systematic review found 10 studies that looked at the distance that respiratory droplets travel. The quality of the data is pretty poor, and many of these studies are based on mathematical models rather than actual measurements. However, the results seem pretty consistent. 8 of the 10 studies showed droplet spread greater than 2 meters. 4 of the 5 papers actually measuring human droplets found spread more than 2 meters, and the only study that didn’t was from 1942 and didn’t describe how they reached their conclusion. However, it isn’t clear how high a risk these droplets represent at 2 meters, and how that risk compares to the risk of carrying contaminated PPE further into the department to get farther from the patient. Furthermore, the participants in these studies were not wearing masks, which should significantly decrease spread.
Bottom line: There is no “2 meter rule” when it comes to droplets, but there is still a lot that we don’t know about this topic.
Will patients be immune?
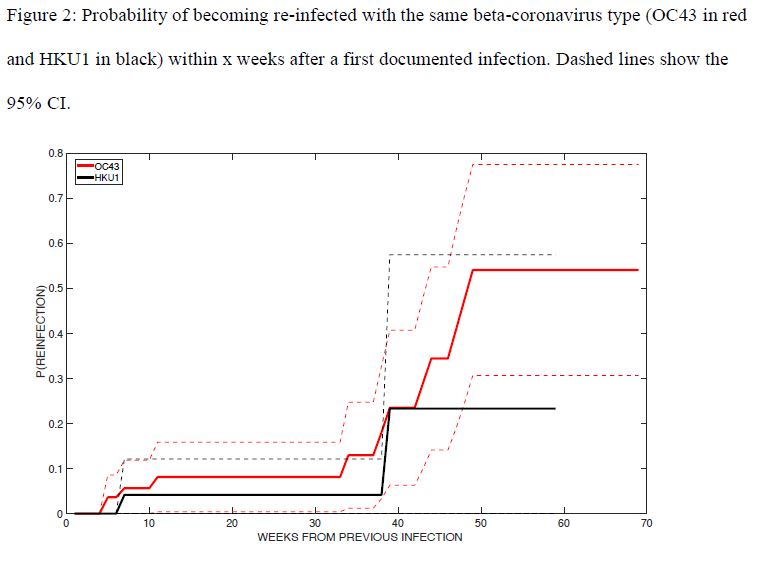
Galanati M and Shaman J. Direct observation of repeated infections with endemic coronaviruses. 2020. Preprint, not officially published, available here.
This study looks at the reinfection rate from endemic coronaviruses (the ones that cause mild colds every year). They have a convenience sample of 214 healthy volunteers from a number of high risk settings (children in daycares, teachers and students in highschool, and emergency department employees). They excluded anyone over the age of 65 (who I would expect to have higher re-infection rates because of immune deficiencies). These volunteers had nasopharyngeal swabs done every week and also recorded a daily symptom journal. This study looks at the subset of 191 that had at least 6 separate NP samples in the same season, looking for the recurrence rate of the same strain of virus. Their outcomes will likely be a conservative estimate, because they defined swabs that were positive 2 weeks in a row as the same infection, and if there was a negative swab between two positives, they assumed that was a false negative and it was all one continuous infection. Given how often infections seem to ping-pong back and forth in households, I would assume that some of these actually represent re-infection. 86 patients tested positive for 1 coronavirus during the year, and 12 (14%) had a subsequent positive with the exact same strain of virus. The median time to reinfection was 37 weeks. 9 of the reinfections were in children, and the remaining 3 occured in patients between 25 and 34 years of age. The real question is how close these endemic coronaviruses are to COVID-19. With SARS and MERS, it was thought that immunity would last longer, given the more extensive immune responses, and antibodies were detected up to 2 years later (but not 5). I would be hesitant to make any major decisions based on this data, but we probably shouldn’t assume that patients will be immune to a second infection after recovering from COVID-19, and we might want to be skeptical about using antibody testing as a tool for allowing people to relax social isolation.
Bottom line: We don’t have long term immunity to endemic seasonal coronaviruses. It isn’t clear how this will apply to COVID-19.
In hospital cardiac arrest in the COVID era
Shao F, Xu S, Ma X, et al. In-hospital cardiac arrest outcomes among patients with COVID-19 pneumonia in Wuhan, China [published online ahead of print, 2020 Apr 10]. Resuscitation. 2020;151:18–23. doi:10.1016/j.resuscitation.2020.04.005 PMID: 32283117
This is a single center chart review from Wuhan looking at inpatient cardiac arrest outcomes in adult patients (over 13 years of age) with known COVID. The results are not good. Of 761 patients admitted over a 1 month period, there were 151 inpatient cardiac arrests (20%). After a few exclusions, they include 136 patients, of whom 110 (81%) were over 60 years of age, but patients had relatively few comorbidities. 119 arrests (88%) were determined to be respiratory in origin. The initial rhythm was asystole in 90% of cases, and only shockable in 6%. Therefore, it is not surprising that ROSC was only achieved in 13%, with 4 patients (3%) alive at 30 days, and only 1 (<1%) alive with good neurologic function.
In this hospital, there was a 24/7 rapid response team ready to deal with cardiac arrest. All staff were wearing PPE, including an N95, for their entire shifts, so they were likely able to get to patients much faster than hospitals that require staff to don PPE after the code blue is called. (In other words, these outcomes probably represent a best case scenario.) On the other hand, they made some modifications to standard ACLS which could have affected outcomes, such as changing the person doing CPR every minute, because of the difficulties in doing CPR in full PPE. Furthermore, it isn’t clear exactly how bad this hospital was hit with COVID-19 at the time of the study, but you could imagine limited resources and over-extended staff could result in worse outcomes.
I almost hesitate to include this study with an audience primarily made up of emergency doctors, as these are not our patients. The results in inpatients with known COVID will not extrapolate well to out of hospital cardiac arrests where cardiac causes are still probably the leading etiology, unless you are in the middle of a really bad surge. Furthermore, this is a single center that was operating outside of its usual norms because of COVID, so we need to be careful about any extrapolations.
Bottom line: In this single center chart review, outcomes after in hospital cardiac arrest in patients with known COVID were dismal. This might guide our decisions on which patients to attempt resuscitation, but we should be aware of the limitations of this data.
As a note on out of hospital cardiac arrest, there is some data from Italy that the total number of arrests is up by 58% and death in the field is also up over the same period from last year. Comparing the same 40 day period, the number of arrests rose from 229 to 362, and the number of patients they transported with ROSC dropped from 31 to 18 (14% to 5%). The numbers don’t look that different between people with or without suspected COVID. (Baldi 2020)
Where did all the patients go?
Metzler B, Siostrzonek P, Binder RK, Bauer A, Reinstadler SJ. Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19: the pandemic response causes cardiac collateral damage. Eur Heart J. 2020;ehaa314. doi:10.1093/eurheartj/ehaa314 PMID: 32297932 [free full text]
This study doesn’t have the best methods, but it raises a very important point that many of us have been talking about: our normal emergency patients have disappeared. This is a retrospective survey, in which they polled the 19 public PCI capable hospitals in Austria about their admissions for acute coronary syndrome in the month of March. There was a 39% reduction in admissions from the first week to the last week of the month, as the COVID-19 pandemic escalated. The retrospective survey methodology is somewhat problematic (it is possible that everyone with ACS was admitted with the diagnosis of “rule out COVID” while swabs were pending, for example). This also could be a commentary on baseline unnecessary admissions for small rises in troponin. However, the rate of STEMI admissions also declined, which doesn’t really fit with either of those explanations. The most likely explanation is the simple one: people are scared to come to the hospital, and are putting their lives on the line by staying at home. (Which fits with the Italian study mentioned above that demonstrated a 58% increase in out of hospital cardiac arrests associated with COVID.) (Baldi 2020)
This is obviously a practical issue we need to rapidly address, but I think it also raises a broader lesson we need to learn in medicine: our actions almost always have unintended consequences. The initial messaging in COVID-19 was all very well intentioned. We needed to decrease unnecessary hospital presentations to preserve PPE. We needed to empty hospital beds to prepare for the potential surge. Unfortunately, these necessary messages created fear and resulted in patients avoiding necessary medical care. Unintended consequences are everywhere in medicine. We focus too much on a surrogate outcome, like lowering glucose, and forget about the consequences of our actions on the complex homeostasis that is human physiology. We craft decision rules with excellent sensitivities designed to decrease imaging, but they ultimately have the unintended consequence of increasing imaging as they are applied in broader populations. We institute screening programs with good intentions, but that have the unintended consequences of many false positives and incidental findings. Unintended consequences can be difficult, if not impossible, to anticipate, but they are a good reminder to engage in second order thinking (what are the likely consequences of the consequences of my actions) and to consider as many perspectives as possible when making decisions.
Bottom line: In Austria, admissions for ACS decreased as the COVID pandemic increased. This probably indicates that patients are scared to come into the emergency department and are missing out on important medical care.
Is COVID causing clots?
Klok FA, Kruip MJHA, van der Meer NJM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020;S0049-3848(20)30120-1. doi:10.1016/j.thromres.2020.04.013 PMID: 32291094 [article]
What is the relationship between COVID-19 and thrombosis? The conclusions of this paper are rather remarkable, and therefore worth knowing, but the quality of the data isn’t great. The authors present a chart review without methods of 184 ICU patients with confirmed COVID-19 pneumonia at 1 of 3 dutch hospitals. They were looking for thrombotic complications, including PE, DVT, ischemic stroke, MI, or systemic arterial emboli. All of these patients were on prophylactic anticoagulation. They report that 31% of these patients had thrombotic complications, the vast majority of which were PEs. Furthermore, they state that this is a conservative estimate, as at the time of writing 76% of these patients were still in the ICU, and therefore still at risk of complications. (It is a bizzare time we are living in, when an ICU cohort study can get published while the vast majority of the patients are still in the ICU.) However, I have some significant concerns about this paper. First of all, the numbers don’t add up. They report 25 PEs, 1 leg DVT, 2 central line related arm DVTs, and 3 ischemic strokes. That is 31 patients out of 184, or 17%, which is still high, but not the 31% they are claiming. That is a big red flag in my book. Furthermore, they tell us almost nothing about these patients, so it is impossible to tell whether the clots were clinically important or just incidental, or whether we can extrapolate these results to our own patients. They also don’t tell us how often or why they were scanning these patients. People are measuring DDimers routinely with COVID, something we don’t do for influenza. Are these thrombosis rates really different from other viral pneumonias? I don’t think we can change practice based on this study. The results don’t add up and the methods are prone to bias. However, I am sure we will hear more about PE and COVID as time goes on, so it is worth knowing about this paper.
Bottom line: This paper suggests an increased rate of thrombosis in COVID patients, but methodologic issues make the results less reliable, and it isn’t clear that the benefits of therapeutic anticoagulation will outweigh the risks.
Can we reuse N95s?
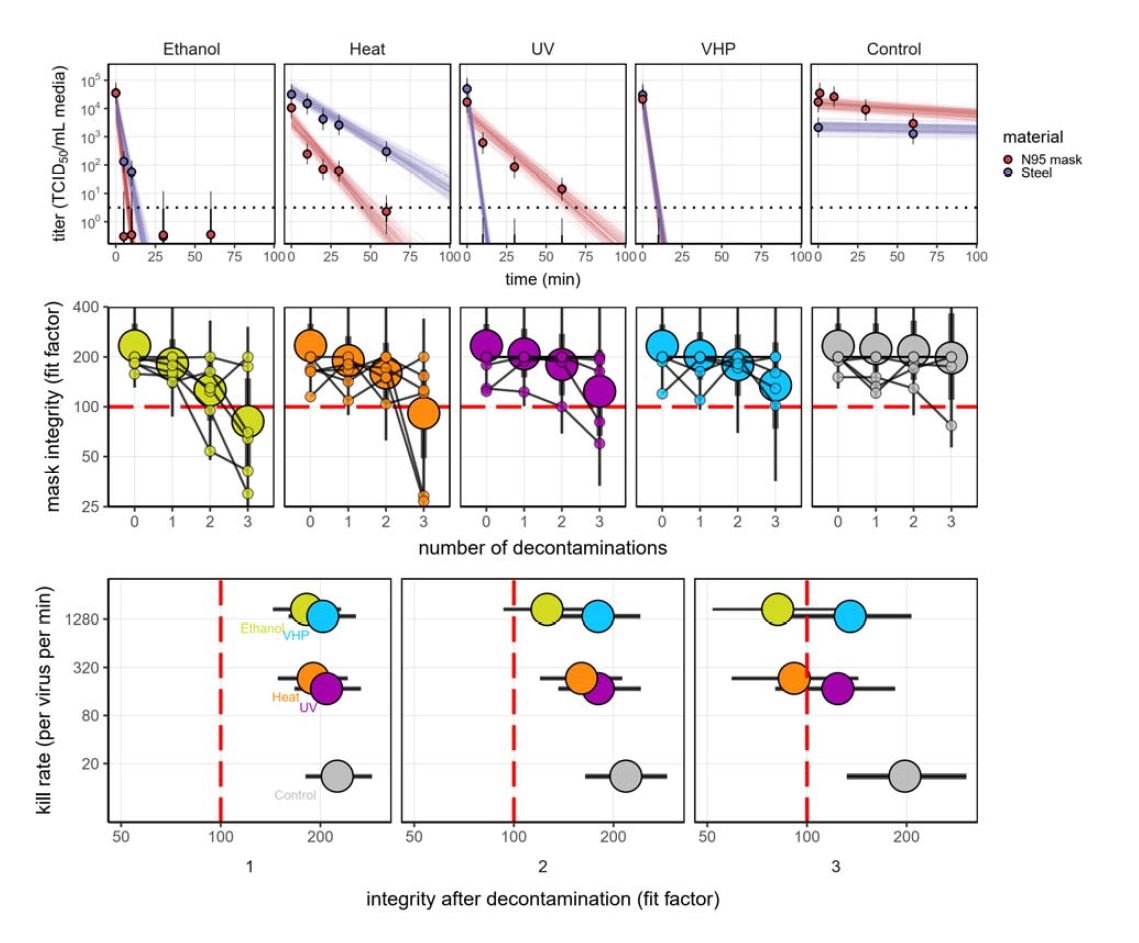
Fischer RJ, Morris DH, van Doremalen N, et al. Assessment of N95 respirator decontamination and re-use for SARS-CoV-2. 2020. Prepublished online.
This lab based study looked at 4 different techniques for decontaminating N95 masks (heat, UV light, 70% ethanol, and vaporized hydrogen peroxide). Vaporized hydrogen peroxide was the only technique to completely eliminate the virus in the relatively short time that they applied each of these techniques. The integrity of the masks held up to 1 decontamination, but the 95% confidence interval fell below the accepted safety standard after 2 decontaminations for all masks. This is probably partially because of the small sample size, but the numbers in this trial make it very clear that if decontamination is used, it should only be used a limited number of times. (The logistics of tracking the number of reuses seems like a bit of a nightmare to me.)
Bottom line: Very limited N95 reuse might be acceptable, but it is not panacea that will solve our PPE shortages.
Awake proning?
Caputo ND, Strayer RJ, Levitan R. Early Self-Proning in Awake, Non-intubated Patients in the Emergency Department: A Single ED’s Experience during the COVID-19 Pandemic. Acad Emerg Med. 2020;10.1111/acem.13994. doi:10.1111/acem.13994 PMID: 32320506 [free full text]
Awake proning has become quite the fad during COVID-19, with lots of anecdotes and social media praise, but this is the first real data on the practice. I could be biased into only saying nice things about this paper, as I know the authors and they are all brilliant, but I think everyone will admit the quality of the data is far from ideal. They look at 50 adult patients presenting to the ED with hypoxia that did not resolve with supplemental oxygen, and who were capable of self-proning. It isn’t clear exactly how these patients were recruited (they use both the terms consecutive and convenience), which could result in selection bias, and makes extrapolation difficult. They also say patients had documented COVID-19, but it isn’t clear to me how that is possible in the initial hours of patients presenting to the emergency department. The median oxygen saturation was 80% at triage, which improved to 84% with supplemental oxygen (mostly by nonrebreather), but then climbed to 94% after 5 minutes of proning. Those numbers look great, but of course they are just surrogate outcomes. An oxygen saturation that rises in the ED, but then crashes on the ward when the patient isn’t surrounded by critical care clinicians, could actually be harmful. Perhaps the most important number in this paper is that only 24% of the patients were intubated within 24 hours (and the median oxygen saturation was only 84% on supplemental oxygen). There are lots of details missing, but I think that in many hospitals 100% of these patients would have been intubated. I think that is a good hint that the surrogate outcome might translate into a patient important outcome. Of course, that is unproven in uncontrolled observational data. This is an important paper, and offers great food for thought, but I do worry about potential unintended consequences (more emergent intubations or unexpected deterioration). We need to be very careful interpreting observational data focused on surrogate outcomes.
Bottom line: A 10% increase in oxygen saturation by simply having a patient roll over is pretty impressive, and the harms of awake proning are probably pretty limited, but this trial cannot definitively tell us whether this translates into patient oriented benefit.
Pseudoscience and COVID-19 — we’ve had enough already
Caulfield T. Pseudoscience and COVID-19 — we’ve had enough already. Nature. 2020; [ARTICLE]
“Cow urine, bleach and cocaine have all been recommended as COVID-19 cures.” The utter disregard for science has been the most frustrating part of this pandemic thus far. We have seen it at all levels, from the tops of governments to local hospital responses. In this editorial, Tim Caulfield calls out hospitals and governments for their long standing practice of accepting and therefore legitimizing anti-science medical bullshit. When universities teach courses that lack any factual basis in reality, they lose credibility. When hospitals offer “alternative” treatments, they spread and reinforce healthcare illiteracy. When governments license quacks, patients are given quack advice. People will certainly die during COVID as a result of anti-scientific “alternative medical” advice. Although this has garnered attention recently, with the many ridiculous “cures” being offered for COVID-19, this is not a new problem. Our patients have long been harmed by this anti-science crap, and it is our fault (via our governments, universities, and healthcare systems) for tolerating it. Caulfield argues that this is our responsibility. Call out the bullshit. Speak up if your hospital or university promotes nonsense. In addition to calling out these major institutions, we also need to get reliable information to our communities. “The best way to fight misinformation is to swamp the landscape with accurate information that is easy to digest, engaging and easy to share on mobile devices.” Anti-scientific woo hurts our patients and damages our communities. We have ignored it too long. It has to go. “Let us hope that one of the legacies of this crisis will be the recognition that tolerating pseudoscience can cause real harm.”
Some hydroxychloroquine/chloroquine updates
Since the last edition, there have been a number of studies looking at hydroxychloroquine, but none are really worth going into in detail. The answer is the same: you shouldn’t be using this drug for COVID. All the studies were updated in the main post. As a quick review:
- Tang 2020 is a multi-center RCT of hydroxychloroquine in 150 patients that showed no difference in either viral cure or symptoms, but a significant increase in adverse events with hydroxychloroquine.
- Magagnoli 2020 is a retrospective look at 368 patients admitted to the Veterans Health Administration hospitals in the United States. The rate of death was higher in patients who were treated with hydroxychloroquine than in those who were not (28% vs 11%, p=0.03). Of course, this is not a randomized trial, and hydroxychloroquine might just have been given to sicker patients, but it is not promising data.
- Borba 2020 is a double blind RCT comparing two doses of chloroquine (600 mg BID for 10 days or 450 mg BID on day one then daily for 4 more days). They were supposed to enrol 440 patients, but the trial was stopped early after only 81 patients because mortality was significantly higher in the high dose chloroquine group.
Our first look at remdesivir (if you don’t count press conferences) is negative
This is the first double blind, placebo controlled RCT of remdesivir for COVID-19. It was negative. If you want more details than that, they included 236 adult patients admitted with confirmed COVID-19 pneumonia at 1 of 10 hospitals in Wuhan, and randomized them to remdesivir (200 mg on day one and then 100 mg for 9 days) or placebo. Their primary outcome was time to improvement by 2 points on a 6 point scale or discharge from hospital alive. There was no difference (21 vs 23 days; HR 1.23; 95% CI 0.87 – 1.75). There was also no difference in mortality, and there was no difference in viral clearance. The trial was stopped early, which may have resulted in it being under-powered, but it is clear that remdesivir is no wonder drug. (It is worth knowing that there is a second RCT – the ACTT trial – that has been completed and apparently shows a faster time to improvement. We know about it because of press releases, but the study has not actually been published yet, so it is hard to say anything about the results.)
Bottom line: There is still no reason to be prescribing antivirals for COVID-19. There have never been any successful therapies for viral pneumonia, so our pretest probability should remain very low that anything other than good supportive care will improve clinical outcomes in COVID-19.
A Reminder to Reason
Zagury-Orly I, Schwartzstein RM. Covid-19 – A Reminder to Reason. N Engl J Med. 2020;10.1056/NEJMp2009405. doi:10.1056/NEJMp2009405 PMID: 32343505 [free full text]
I don’t think anyone will be too surprised that I like this essay. The authors remind us of the potential harm of our actions. That often, the best course of action is: don’t just do something, stand there. They point out that there are exactly 0 interventions that have been proven to decrease mortality from COVID-19, and that treatment really needs to be focused on high quality supportive care. However, they describe the various biases and cognitive errors that can be accentuated in a crisis, and cause us to make poor decisions. Availability bias occurs when we inappropriately favour recently acquired information. (I heard that many of these patients have clots on a podcast last night. Maybe I should give this patient lytics.) Our anxiety may also increase our chance of anchoring. (I know this patient has had three negative COVID tests, but I don’t care – that is clearly the diagnosis.) Confirmation bias occurs when we only acknowledge the information that supports our beliefs. (Droplets only spread 2 meters, so that nurse couldn’t possibly have become sick at work, because they never came within 2 meters of the patient.) The authors argue that crisis makes anecdotes even more compelling, and that “the rational-emotional scale is tipping towards the emotional side.” They point to our historical mistakes. Of 29 studies looking at steroids during SARS, 25 were inconclusive (and 4 showed harm). In our rush to “do something”, we were left with flawed studies, no real answers, and potential “negative physical, social, and economic consequences.” Despite the sense of urgency that this crisis creates, science is fundamental for the good practice of medicine. Unfortunately, many seem to have forgotten that.
The first COVID research round up can be found here, if you missed it.
Cheesy Joke of the Month
Where do boats go when they are sick?
The dock
Cheesy Bonus Jokes
It was pointed out to me that I forgot to include a joke last time, so I had better include a couple bonus COVID related jokes, as I know that many people only read these updates for the bad jokes.
You know who buys up all the toilet paper? Assholes
What types of jokes are allowed during quarantine? Inside jokes
Did you hear the joke about the germ? Never mind, I don’t want to spread it around.
Why don’t chefs find coronavirus jokes funny? They’re in bad taste.
Other references
Baldi E, Sechi GM, Mare C, et al. Out-of-Hospital Cardiac Arrest during the Covid-19 Outbreak in Italy [published online ahead of print, 2020 Apr 29]. N Engl J Med. 2020;10.1056/NEJMc2010418. doi:10.1056/NEJMc2010418 PMID: 32348640
Borba MGS, Val FFA, Sampaio VS, et al. Chloroquine diphosphate in two different dosages as adjunctive therapy of hospitalized patients with severe respiratory syndrome in the context of coronavirus (SARS-CoV-2) infection: Preliminary safety results of a randomized, double-blinded, phase IIb clinical trial (CloroCovid-19 Study). 2020. Not published. Available preprint here.
Magagnoli J, Narendran S, Pereira F, et al. Outcomes of hydroxychloroquine usage in United States veterans hospitalized with Covid-19. 2020. Not published. Available preprint here.
Tang W, Cao Z, Han M, et al. Hydroxychloroquine in patients with COVID-19: an open-label, randomized, controlled trial. 2020. Not published. Available preprint here.
Morgenstern, J. COVID Research Roundup 2, First10EM, May 11, 2020. Available at:
https://doi.org/10.51684/FIRS.20945


One thought on “COVID Research Roundup 2”
Audio is out now at :
http://traffic.libsyn.com/broomedocs/May2020_Covid_First10EM.mp3