
Morgenstern, J. Laceration evidence part 7: Aftercare instructions, First10EM, December 26, 2022. Available at:
https://doi.org/10.51684/FIRS.128678
We have finally reached the end of the laceration repair series. So far, it seems like nothing we do really matters. Eversion was a myth. Glue and steri-strips are as good as sutures. For that matter, for many lacerations we could probably just do nothing at all. The human body has a remarkable ability to repair itself, and our emergency department interventions seem to have a very small impact on that process. However, unlike our brief emergency encounters, patients will care for their wounds for many days, so maybe our aftercare instructions really matter? Maybe the things patients do after they leave the department will be the most important part of healing? Or maybe, like all the topics covered thus far, the evidence will just be too weak to say anything conclusive. Let’s find out.
Can wounds get wet?
The biggest question my patients have for me after laceration repair is: can I get this wet? Am I allowed to shower?
There is a multi-center study comparing early water exposure to dry dressings in family practice patients after simple excisions. (Heal 2006) Randomization was done by selecting a ball out of a hat, and there is no blinding, so methodology is imperfect, but it is a large trial (870 patients) with 98.5% follow-up. They “asked the dry group to leave the dressing on and keep it dry for the first 48 hours, then to bathe and undress as normal until the sutures were taken out.” They “asked the wet group to take the dressing off within the first 12 hours and then bathe as normal until the sutures were taken out.” The infection rate was identical in both groups (8.6% vs 8.9%), allowing for a statistical conclusion of non-interiority. The infection rate is higher than I would like to see, especially given that these were sterile excisions and not traumatic lacerations. Additionally, 48 hours may still be considered early by some practitioners, and with only a 36 hour gap between the two groups, the trial may be biased towards equivalence.
A Cochrane review of bathing or showering post-operatively from 2015 only found a single study, and it was the RCT by Heal discussed above. (Toon 2015)
There is an RCT from 1982 that I haven’t been able to get my hands on. (Voorhees 1982) The summary from a review paper is that 82 patients were randomized post-operatively to bathing on the second postoperative day or keeping the wounds dry until the sutures were removed. (Harrison 2016) There was no statistical difference between the groups, with 4 infections in the dry group and 2 in the bathing group. I can’t comment on methodology beyond the fact that this is a small unblinded trial, and therefore low quality.
There is another small RCT from 1981 in which I have a hard time deciphering the exact methodology, because different parts of the short methods sections seem to contradict themselves. (Goldberg 1981) They include 200 consecutive patients with head and neck wounds, but it is a mix of emergency department traumatic wounds and post-operative patients. Some patients were asked to keep their wounds dry until the sutures were removed. Other patients were told they were allowed to rinse the wounds with soap and water, and that bathing and showering was allowed. Every time the wound got wet, they had the patient apply topical antibiotics, but “the ointment was used only to lubricate the suture line and not for any antibiotic properties”. There were no infections at all. One patient in the water exposure group needed a scar revision after developing an inclusion cyst on the scar line.
There is a case series of 100 patients undergoing soft tissue excisions, and all were asked to wash the wound with soap and water twice a day starting the morning after the surgery (Noe 1988) They report no infections among these 100 patients, but this is obviously an extremely low level of evidence.
There is a letter to the editor from a plastic surgeon who was responsible for repairing lacerations for the Toronto Maple Leafs in the 1980s claiming that, contrary to the prevalent advice to keep wounds dry, cleaning wounds with soap and water makes the most sense. (Douglas 1988) He states that he has treated thousands of patients this way, and wound infections are “surprisingly rare”. I don’t think we can count this as evidence, but it felt like a fun publication to include anyway.
Unlike some of the other questions, I think this post-operative data is likely applicable to the traumatic lacerations that we see. If anything, you would think that there is a higher risk of exposing sterile surgical wounds to water and the outside world, so I expect a lack of difference in the surgical setting would translate well to traumatic lacerations.
I think some basic physiologic reasoning can be applied to this question. Personally, I wouldn’t expose a laceration to lake water, or a hot tub, or a public pool. However, basic hygiene with soap and water seems like it would go a long way to decreasing infection. Until new evidence comes alone, I encourage normal hygiene. (I imagine there are many partners and family members who appreciate the advice that their loved ones bathe.)
Bottom line: Very low level of evidence, but it is probably safe to get wounds wet early after repair, and keeping them clean with soap and water makes physiologic sense.
Do dressings help? If so, what kind and when should they be removed?
Physiologically, the primary role of a dressing is to keep dirt and pathogens from the outside world out of the wound, although there are other potential benefits, such as absorbing exudate, and preventing blood from getting all over one’s bedsheets. (This becomes complicated, as some dressings are medicated, and therefore might be better considered in the section on topical medications.) Traumatic lacerations are likely to already be contaminated, so it is unclear how important it is to avoid further contamination. On the other hand, surgical wounds are ideally sterile when the dressing is placed, and so represent the ideal scenario for dressing efficacy. In my mind, if dressings don’t help in post-operative patients, they are very unlikely to help in patients with traumatic lacerations.
The question of whether a dressing helps is deceptively complex. There are hundreds of types of dressings, which can be used for different lengths of times, and in combination with many other therapies, such as topical antibiotics. Considering the number of potential combinations, the quantity of available data is shockingly small. Definitive conclusions are impossible.
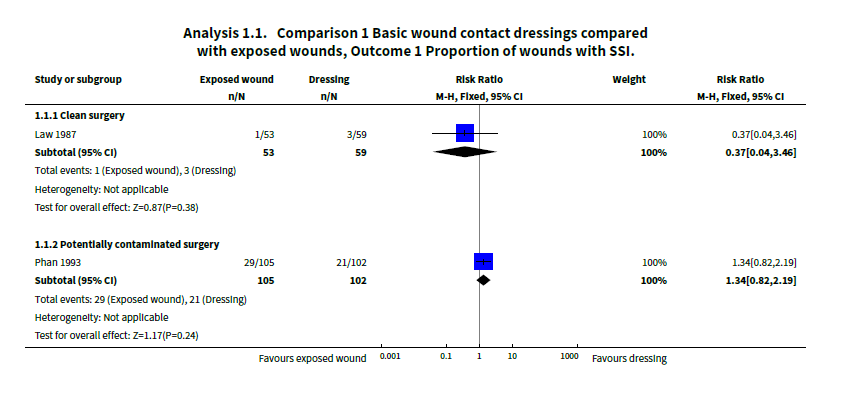
There is a Cochrane review looking at the use of dressings after surgery, including studies that compared dressings to no dressings, as well as studies comparing different types of dressings. (Dumville 2016) They conclude, “we found no clear evidence to suggest that one dressing type was better than any other at reducing the risk of surgical site infection, nor that covering wounds with any dressing at all reduced the risk of surgical site infection. Additionally, there was no clear evidence that any dressing type improves scarring, pain control, patient acceptability or ease of removal.” However, I think the most important takeaway from this review is that the trials were all small with a high risk of bias, and so we really have no idea if dressings help post-operatively. There are only 2 RCTs comparing dressings to no dressings, and even ignoring sources of bias, you can see that statistically, we have no idea if they help:
There is another Cochrane review from 2015 looking at surgical patients, and comparing early (less than 48 hours) and late (more than 48 hours) removal of dressings. (Toon 2015) There were only 3 studies, with a total of 280 patients. Also, I am not sure 48 hours is the time frame we care about. Although our conclusions from this paper should be very limited, they conclude “the early removal of dressings from clean or clean contaminated surgical wounds appears to have no detrimental effect on outcomes”.
Another Cochrane review looks at the use of silicone gel sheeting. (O’Brien 2013) I have never seen silicone gel sheeting used, which makes sense as it is not supposed to be applied to open wounds. It has been tested prophylactically, to prevent scarring, after initial post-operative wound healing in people prone to hyper-trophic scars. Although the numbers are impressive (risk ratio 0.46, 95% CI 0.21-0.98), the trials were highly susceptible to bias, with none of the trials being blinded for this mostly subjective outcome. It has also been tested as a treatment, after hypertrophic scars or keloid develop, and again there is a statistical benefit, but in trials of low methodological quality with high risk of bias. There isn’t really a good physiologic explanation as to how or why it would work, and it is quite expensive, so for now it shouldn’t be recommended routinely.
Almost every textbook and review article I found suggests that wounds heal best in a moist environment. (Korting 2011, Singer 1997, Singer 2008, Atiyeh 2002) There are many theoretical reasons this might be true, but the conjecture seems to be based entirely on laboratory and animal data. For acute wounds, I could not find any clinical trials of the fancy dressings, such as hydro-colloids, that are supposed to promote healing by creating a moist environment. I think it is reasonable to apply a small amount of petroleum jelly or antibiotic ointment to a wound based on the laboratory data, but would want to see clinic data before suggesting the much more expensive dressings that are available.
Researching this topic was incredibly frustrating. The citations in review papers just lead to other review papers, and it becomes almost impossible to separate clinical conjecture, from animal data, from clinical data in humans. I spent many days chasing my tail trying to determine why papers make the claims they do, but it mostly proved to be a futile exercise. It is possible that I have missed important trials, and if so, please send them my way. However, as far as I can tell, there is currently no strong clinical data to suggest the use of any specific type of dressing after the treatment of lacerations in the emergency department.
Although there are theoretical reasons that a dressing might help (reducing subsequent contamination), there are also theoretical reasons they could harm (they are usually dry dressings, and a moist environment might improve healing.) Dressings definitely add cost and hassle to patients, so there should probably be evidence of benefit if we are going to routinely suggest them.
Bottom line: The current evidence is very weak. There does not seem to be any evidence that dressings improve healing after acute lacerations. It makes sense to use a dressing for comfort, and to absorb blood and exudate in the first 12-24 hours after repair. Obviously, patients can continue to use dressings for aesthetic or comfort reasons if they prefer.
Should we use antibiotic ointments?
The debate about antibiotics ointments might provoke the strongest opinions of any topic in laceration aftercare. As if often the case in medicine, scientific support for those opinions seems to be mostly lacking.
In an early study from 1967, 432 patients either had a triple antibiotic preparation (neomycin, bacitracin, polymyxin B) sprayed into and around their wounds or no treatment. (Caro 1967) The study was not randomized, but rather just alternated back and forth between treatment groups. All of the wounds were cleaned with “Hibitane”, which I think is chlorhexidine? There was no difference in infection rate (10% in both groups). (This actually isn’t aftercare, but closer to irrigation type treatment in the ED, but the results may be somewhat applicable to decisions about topical antibiotics.)
In another trial that should technically be included under the “irrigation” discussion, but is so unlike any irrigation that we do today that I think it is more relevant to the antibiotics discussion, lacerations were randomized to ‘be flooded” with 10 mL of either normal saline or penicillin (in a double-blind fashion). (Lindsey 1982) Infections were decreased with antibiotics in both the early (< 48 hours) and late time frames, but the manuscript contains very little information and the infection rate with placebo seems very high at 31%. Although double blind, there are many problems with this trial and/or manuscript. We have no information about how many patients were lost to follow-up. Randomization was done by coin flip. Sample size wasn’t pre-determined. Perhaps most importantly, this practice of irrigation with antibiotics is simply not used, and so the results may not be that relevant.
There is a double-blind, placebo controlled trial that looked at the role of three different antibiotics ointments – bacitracin, triple antibiotic ointment (neomycin, bacitracin, and polymyxin B), and silver sulfadiazine – in 465 patients with minor wounds requiring suturing in a single emergency department. (Dire 1995) They excluded patients with immunocompromise and wounds older than 12 hours. All wounds were irrigated and scrubbed of visual particulate matter. Patients were discharged with instructions to clean the wounds with soap and water 3 times a day, and then apply the study ointment. (You can see the complexity and overlap between our various aftercare questions.) Otherwise, the wounds were kept covered, clean, and dry. Wound infections occurred in 6% of the bacitracin group, 5% of the triple antibiotic group, 12% of the silver sulfadiazine group, and 18% of the placebo group. The decrease of infections with antibiotic ointments was statistically significant, but there was no statistical difference between the groups. Although that difference sounds important, I think the results are more complex than that simple summary. Almost all of the infections were simple stitch abscesses, treated with local wound care only and not antibiotics. There were very few higher grade (cellulitis or systemic) infections, and there was no statistical difference in those infections. One patient in the triple antibiotic group had an allergic reaction and had to stop treatment. The study isn’t perfect. It is a single center study at a military hospital, and I wonder if military patients might be different. They may be more compliant with recommended therapy, but they also may be more likely to have duties that expose wounds to dirt or contamination. There is a clear difference in this study, but not in the kind of infections that we really care about.
There is a triple blind, single-centre pilot RCT that enrolled 120 patients with complicated soft tissue wounds presenting within 24 hours (and without exclusions based on health conditions), and randomized them to either triple antibiotic ointment (neomycin sulfate, bacitracin zinc, and polymixin B sulfate) or mupirocin. (Hood 2004) This is a well done study, although requiring in-person reassessment at 7 days did lead to an expected loss of 21 patients. Perhaps the biggest problem with the study is the definition of infection. The study nurses thought 9 patients had ‘signs of infection’, whereas only 2 were diagnosed with an infection by the physicians, but neither of these infections were thought to need any treatment, so were they really important infections? There were no statistical differences between the groups, but the rate does look clinically higher in the mupirocin group as compared to the triple antibiotic group. This is only a pilot study, and as far as I can tell, it never led to a full-sized follow-up RCT.
There is a Canadian Agency for Drugs and Technologies in Health (CADTH) review of topical antibiotics for wounds that are already infected. (Cowling 2017) Although that is not the question I am considering today, it is interesting to note that there is basically no quality data supporting the use of topical antibiotics in the treatment of infected wounds. That is because there is basically no data.
There is a 1995 systematic review that looks at the use of systemic prophylactic antibiotics for simple non-bite wounds. (Cummings 1995) They identified 7 RCTs, encompassing 1701 patients. Five used oral antibiotics and 2 gave intramuscular doses. None of the studies had statistically significant results, but point estimates of infection rates were higher in the antibiotic group in 6 of the 7 studies. The meta-analysis shows no statistical difference, with an odds ratio of 1.16 favoring no antibiotics (95% CI 0.77 to 1.78). Many people would consider systemic antibiotics to be a ‘stronger’ therapy than topical (I am not sure I agree), so it is possible that the lack of utility of systemic antibiotics indicates that topical antibiotics are unlikely to help.
The evidence from the surgical literature is mixed, and complicated by the fact that most surgeries involved prophylactic systemic antibiotics, so topical antibiotics may have less of a role. (McHugh 2011)
Bottom line: There is very little evidence either for or against this practice. The one proper RCT we have shows a decrease in infections, but the infections being prevented did not require antibiotics, and so were very minor. There are added costs with topical antibiotics, as well as side effects like allergic reactions, but both are minor. It probably doesn’t matter much one way or another, and I just let my patients decide.
Are there other medications that will reduce scarring or improve healing?
There is a Cochrane review looking at aloe vera for acute and chronic wounds, including lacerations. (Dat 2012) They found no trials looking at lacerations, but there were 2 RCTs in post-operative patients. The most applicable would probably be the trial of aloe vera after skin biopsy, in which there was no benefit, because 100% of patients in both groups had completely healed wounds at follow-up. (Phillips 1995) The RCT of aloe-vera after hemorrhoidectomy is a high quality design, with double blinding, but the results seem rather unbelievable to me. (Eshghi 2010) They don’t define a primary outcome, but they emphasize at 2 weeks 100% of the aloe group was fully healed as compared to 4% of the placebo group! That is an unheard of difference in medicine, making aloe vera the most miraculous cure of all time. All other outcomes, such as pain, also favoured aloe in the first few weeks, but by the end of the trial everyone had healed well without complications whatever group they were in. This is unlikely to apply to our laceration patients, and certainly needs to be replicated to be believed, but it would clearly be a worthwhile practice if true.
It is possible that honey should have been included in the dressing section, as the purported function is more as a bacteriostatic barrier cream, but it doesn’t look much like a dressing, so I include it here. There is a Cochrane review of honey in wounds that includes 26 trials and 3011 patients, but almost all of these trials are in chronic wounds or burns. (Jull 2015) Their overall conclusion is that, although there are positive studies, it is difficult to draw firm conclusions because of clinical heterogeneity and the low quality of the evidence, which is not surprising at all. In the 3 trials that looked at acute wounds, there was no difference in time to healing, infection, or adverse events when honey was compared to conventional dressings, but the confidence intervals are too large to provide any certainty. Only one of these three studies looked at traumatic wounds, which were only superficial abrasions, so the evidence is not really all that applicable.
Vitamin E is one of the more commonly recommended agents for the reduction of scars. I could not find any studies looking at vitamin E in traumatic lacerations. A systematic review identified 6 trials that assessed the effect of vitamin E on scar formation after surgery. (Tanaydin 2016) The results are mixed and hard to interpret, especially considering that many of the trials mixed vitamin E with other therapies such as hydrocortisone or silicon sheets. Three of the trials reported improved subjective outcomes, while 3 were negative. All 3 double blind trials were negative, which suggests to me bias in the subjective outcome in the imperfectly blinded trials. One trial reported contact dermatitis in 33% of patients treated with vitamin E, and another reported an increase in itch and rash.
I can return to the topic of vitamin E and go into the individual studies in detail if people are interested, but I don’t think it is going to give you an answer. The positive studies are somewhat dramatically positive (eg, 0% vs 7% keloids, or 97% vs 75% very good outcomes), but methodologic issues abound. The highest quality methodologic studies are negative, and there is a clear sign of harm in increased dermatitis. It is possible that vitamin E helps. The science is just not good enough to be sure. However, if we consider the added cost and increase in reported adverse events, I think we should probably wait for better studies before routinely recommending vitamin E. (Like many topics in emergency medicine, this should be a very easy RCT to perform, so if anyone is a big vitamin E proponent out there, this is a great opportunity to perform and publish some high quality research.)
Sun exposure
Healing wounds lack pigment, and with rapidly dividing cells, are likely more prone to injury from carcinogens like UV light. Lack of pigment in wounds increases risk of sunburn, and damage from ultraviolet radiation can lead to hyperpigmentation and increased scar size. At least, that is the claim made in almost every review article, textbook, and website. However, whether any of this is true (or, more specifically, whether the biological changes are clinically relevant) seems to be unknowable, as these claims are made universally without citation, reference, or discussion of clinical evidence.
I don’t know if I am using the wrong search terms, but hours on PubMed, the Trip Database, Google Scholar, and just plain google have led me nowhere. I don’t think we know whether sun protection after traumatic lacerations improves any clinical outcomes.
A reasonable physiologic argument can be made for protecting wounds from the sun. Conversely, ultraviolet light is known to be anti-microbial, and so some have suggested that purposeful exposure to UV light may be beneficial for some types of wounds. (Gupta 2013) Furthermore, lacerations are extremely common, and my guess is that the vast majority of our patients are not following advice about sun avoidance for the 6 months to 2 years that is often recommended, and almost all patients have favorable outcomes. Therefore, if sun avoidance is beneficial, the benefit must be relatively small.
If you know of evidence that sun avoidance helps, please share it below. Otherwise, I would generally tell my patients that sun burns are bad, but they can probably just maintain their normal skin protection regimen after a laceration.
Discussion
For such a common problem in emergency medicine, there is a striking paucity of evidence to guide our care of lacerations. Nothing I found allowed for definitive conclusions, so clinical judgment and shared decision making are, like always, necessary.
Personally, I tell patients:
- A dressing isn’t required, but you probably want one for the first 24 hours, as some bleeding may still occur. After that point, I would suggest applying a dressing if you are in an environment where the wound might become contaminated, or if you prefer one for cosmetic sake, but I want you to remove the dressing every day to check for signs of infection.
- It is fine to get the wound wet, and in fact I like the idea of keeping the area clean with soap and water. However, I would avoid obviously contaminated water sources, like lakes and public pools until the wound is completely healed.
- Topical antibiotics probably aren’t necessary. They might prevent small pimple-like infections, but there is a risk of an allergic reaction. You can use an over-the-counter preparation if you like.
- I don’t think there is any evidence that vitamin E or expensive scar creams help. Applying a very light layer of vaseline during the first week, to keep the wound moist as it heals, might make sense.
Obviously, all of these recommendations can be adjusted based on clinical judgment, such as if the patient has immunosuppression.
Other FOAMed
Laceration Aftercare Instructions – lacerationrepair.com
Closing the gap – Laceration after care
References
Atiyeh BS, Ioannovich J, Al-Amm CA, El-Musa KA. Management of acute and chronic open wounds: the importance of moist environment in optimal wound healing. Curr Pharm Biotechnol. 2002 Sep;3(3):179-95. doi: 10.2174/1389201023378283. PMID: 12164477
Caro D, Reynolds KW, De Smith J. An investigation to evaluate a topical antibiotic in the prevention of wound sepsis in a casualty department. Br J Clin Pract. 1967 Dec;21(12):605-7. PMID: 6082563
Cowling T, Jones S. Topical antibiotics for infected wounds: A review of the clinical effectiveness and guidelines. Ottawa: CADTH; 2017 Mar. (CADTH rapid response report: summary with critical appraisal).
Cummings P, Del Beccaro MA. Antibiotics to prevent infection of simple wounds: a meta-analysis of randomized studies. Am J Emerg Med. 1995 Jul;13(4):396-400. doi: 10.1016/0735-6757(95)90122-1. PMID: 7605521
Dat AD, Poon F, Pham KB, Doust J. Aloe vera for treating acute and chronic wounds. Cochrane Database Syst Rev. 2012 Feb 15;(2):CD008762. doi: 10.1002/14651858.CD008762.pub2. PMID: 22336851
Dire DJ, Coppola M, Dwyer DA, Lorette JJ, Karr JL. Prospective evaluation of topical antibiotics for preventing infections in uncomplicated soft-tissue wounds repaired in the ED. Acad Emerg Med. 1995 Jan;2(1):4-10. doi: 10.1111/j.1553-2712.1995.tb03070.x. PMID: 7606610
Douglas LG. Stitches and water. Plast Reconstr Surg. 1988 Aug;82(2):364. doi: 10.1097/00006534-198808000-00044. PMID: 3399573
Dumville JC, Gray TA, Walter CJ, Sharp CA, Page T, Macefield R, Blencowe N, Milne TK, Reeves BC, Blazeby J. Dressings for the prevention of surgical site infection. Cochrane Database Syst Rev. 2016 Dec 20;12(12):CD003091. doi: 10.1002/14651858.CD003091.pub4. PMID: 27996083
Eshghi F, Hosseinimehr SJ, Rahmani N, Khademloo M, Norozi MS, Hojati O. Effects of Aloe vera cream on posthemorrhoidectomy pain and wound healing: results of a randomized, blind, placebo-control study. J Altern Complement Med. 2010 Jun;16(6):647-50. doi: 10.1089/acm.2009.0428. PMID: 20569031
Goldberg HM, Rosenthal SA, Nemetz JC. Effect of washing closed head and neck wounds on wound healing and infection. Am J Surg. 1981 Mar;141(3):358-9. doi: 10.1016/0002-9610(81)90196-3. PMID: 7212184
Gupta A, Avci P, Dai T, Huang YY, Hamblin MR. Ultraviolet Radiation in Wound Care: Sterilization and Stimulation. Adv Wound Care (New Rochelle). 2013 Oct;2(8):422-437. doi: 10.1089/wound.2012.0366. PMID: 24527357
Harrison C, Wade C, Gore S. Postoperative washing of sutured wounds. Ann Med Surg (Lond). 2016 Sep 2;11:36-8. doi: 10.1016/j.amsu.2016.08.015. PMID: 27668079
Heal C, Buettner P, Raasch B, Browning S, Graham D, Bidgood R, Campbell M, Cruikshank R. Can sutures get wet? Prospective randomised controlled trial of wound management in general practice. BMJ. 2006 May 6;332(7549):1053-6. doi: 10.1136/bmj.38800.628704.AE. Epub 2006 Apr 24. PMID: 16636023
Hood R, Shermock KM, Emerman C. A prospective, randomized pilot evaluation of topical triple antibiotic versus mupirocin for the prevention of uncomplicated soft tissue wound infection. Am J Emerg Med. 2004 Jan;22(1):1-3. doi: 10.1016/j.ajem.2003.09.009. PMID: 14724869
Jull AB, Cullum N, Dumville JC, Westby MJ, Deshpande S, Walker N. Honey as a topical treatment for wounds. Cochrane Database Syst Rev. 2015 Mar 6;(3):CD005083. doi: 10.1002/14651858.CD005083.pub4. PMID: 25742878
Khoosal D, Goldman RD. Vitamin E for treating children’s scars. Does it help reduce scarring? Can Fam Physician. 2006 Jul;52(7):855-6. PMID: 16893147
Korting HC, Schöllmann C, White RJ. Management of minor acute cutaneous wounds: importance of wound healing in a moist environment. J Eur Acad Dermatol Venereol. 2011 Feb;25(2):130-7. doi: 10.1111/j.1468-3083.2010.03775.x. Epub 2010 Jul 6. PMID: 20626534
Lindsey D, Nava C, Marti M. Effectiveness of penicillin irrigation in control of infection in sutured lacerations. J Trauma. 1982 Mar;22(3):186-9. doi: 10.1097/00005373-198203000-00002. PMID: 7040695
McHugh SM, Collins CJ, Corrigan MA, Hill AD, Humphreys H. The role of topical antibiotics used as prophylaxis in surgical site infection prevention. J Antimicrob Chemother. 2011 Apr;66(4):693-701. doi: 10.1093/jac/dkr009. Epub 2011 Feb 3. PMID: 21393223
Noe JM, Keller M. Can stitches get wet? Plast Reconstr Surg. 1988 Jan;81(1):82-4. PMID: 3336642
O’Brien L, Jones DJ. Silicone gel sheeting for preventing and treating hypertrophic and keloid scars. Cochrane Database Syst Rev. 2013 Sep 12;2013(9):CD003826. doi: 10.1002/14651858.CD003826.pub3. PMID: 24030657
PhillipsT, OngenaeK, KanjL, Slater-FreedbergJ. A randomised study of an Aloe vera derivative gel dressing versus conventional treatment aMer shave biopsy excisions. Wounds 1995;7(5):200-2.
Singer AJ, Hollander JE, Quinn JV. Evaluation and management of traumatic lacerations. N Engl J Med. 1997 Oct 16;337(16):1142-8. doi: 10.1056/NEJM199710163371607. PMID: 9329936
Singer AJ, Dagum AB. Current management of acute cutaneous wounds. N Engl J Med. 2008 Sep 4;359(10):1037-46. doi: 10.1056/NEJMra0707253. PMID: 18768947
Tanaydin V, Conings J, Malyar M, van der Hulst R, van der Lei B. The Role of Topical Vitamin E in Scar Management: A Systematic Review. Aesthet Surg J. 2016 Sep;36(8):959-65. doi: 10.1093/asj/sjw046. Epub 2016 Mar 14. PMID: 26977069
Toon CD, Lusuku C, Ramamoorthy R, Davidson BR, Gurusamy KS. Early versus delayed dressing removal after primary closure of clean and clean-contaminated surgical wounds. Cochrane Database Syst Rev. 2015 Sep 3;2015(9):CD010259. doi: 10.1002/14651858.CD010259.pub3. PMID: 26331392
Toon CD, Sinha S, Davidson BR, Gurusamy KS. Early versus delayed post-operative bathing or showering to prevent wound complications. Cochrane Database Syst Rev. 2013 Oct 12;(10):CD010075. doi: 10.1002/14651858.CD010075.pub2. Update in: Cochrane Database Syst Rev. 2015;(7):CD010075. PMID: 24122544
Voorhees EG, Rosenthal D, Hirata RM, Weber CJ. Early postoperative showering. Mil Med. 1982 Nov;147(11):967-8. PMID: 6817188



5 thoughts on “Laceration evidence part 7: Aftercare instructions”
Hi Justin,
Really helpful series. The issue I worry about with getting wounds wet is when I’ve used glue (which I know you love). Would you/evidence support patients getting glued wounds wet/washing them?
Thanks,
Jo
I don’t think aftercare instructions were included in any of the skin adhesive studies, so I can’t give you an answer based on that evidence.
But a purely science based answer is that water has no effect on Dermabond. Water doesn’t have any impact on the polymer. We actually know this clinically, even if we forget it in our aftercare instructions. If we accidentally glue a patient’s eye closed, or a patient comes in glued together with super-glue, do we ask them to soak it in water? Of course not, because water has no effect on these products. I have also had to glue myself closed many times, and have never had problems with water.
Personally, I tell patients that they can bath and shower as soon as they get home. Getting the wound wet is perfectly fine, but don’t scrub the area, and avoid applying any creams or lotions to the area (because the petroleum jelly based products will likely impacts the polymer).