After two editions focused on COVID, it’s time to get back to some standard emergency medicine topics. (Yes, there are many more COVID papers to cover, but I am sort of sick of reading them.) This time we cover dog therapy in the ED, imaging for renal colic, hypothermia, vitamin C in sepsis, Achilles tendon ruptures, and much more…
Add to the list of “have I missed this?”
Meggs WJ, Lee SK, Parker-Cote JN. Wernicke encephalopathy associated with hyperemesis gravidarum. Am J Emerg Med. 2019;S0735-6757(19)30625-4. doi:10.1016/j.ajem.2019.09.012 PMID: 31784394
This is a quick case report of a 27 year old woman who was discharged with a diagnosis of hyperemesis gravidarum and gallbladder sludge, but represented 3 days later with altered mental status. The ophthalmoplegia gives the diagnosis away, although they still got both a CT and an MRI. The patient had thiamine deficiency leading to Wernicke’s encephalopathy. This disease has a strong association in our minds with alcoholism, but we (or at least I) tend to forget the other possible causes. Although it is a rare presentation, I include this case report as a nice reminder that many patients are at risk of dietary insufficiencies. We see cancer, eating disorders, and cyclic vomiting on a daily basis. Thiamine, among the other essential nutrients, should remain firmly in the front of the emergency clinician’s brain. I think we have debunked the idea that thiamine must be given before glucose, but we shouldn’t downplay its importance. We routinely add it when giving alcoholics IV fluids. We also need to be thinking about other at risk patients.
Bottom line: Remember that alcoholism is not the only cause of thiamine deficiency.
Have you heard? We use CT way too much
Moore CL, Carpenter CR, Heilbrun ME, et al. Imaging in Suspected Renal Colic: Systematic Review of the Literature and Multispecialty Consensus. Ann Emerg Med. 2019;74(3):391–399. PMID: 31402153 DOI: 10.1016/j.annemergmed.2019.04.021
This is a great paper that combines a systematic review and a modified Delphi process to develop imaging suggestions across a range of renal colic presentations. They include experts from emergency medicine, urology, and radiology. The most important take-away is that CT is only recommended in a small portion of the cases. Many patients with renal colic don’t need any imaging at all – such as a young patient with a classic story, a prior history of stones, and pain that improves with analgesia. If imaging is needed, ultrasound is often preferred over CT. Even so, I think this paper still recommends CT far too often. For example, CT is recommended in every patient with abdominal tenderness (to look for an alternative diagnosis), but ultrasound is often still the first line test if you are looking for something like appendicitis, diverticulitis, cholecystitis, or ovarian pathology.
Bottom line: If renal colic results in a reflex CT, it might be time to modify your practice. For many patients, this is a clinical diagnosis that requires no imaging at all.
You can read more details in this post.
Can we get a dog?
Kline JA, VanRyzin K, Davis JC, et al. Randomized Trial of Therapy Dogs Versus Deliberative Coloring (Art Therapy) to Reduce Stress in Emergency Medicine Providers . Acad Emerg Med. 2020; doi:10.1111/acem.13939 PMID: 32266765 [article] NCT03628820
Commentary: Morgenstern J, Heitz C, Bond C, Milne WK. Hot off the Press: Randomized trial of therapy dogs versus deliberative coloring (art therapy) to reduce stress in emergency medicine providers. Acad Emerg Med. 2020;10.1111/acem.14006. doi:10.1111/acem.14006 PMID: 32374921
I love this paper. In an attempt to reduce stress during shifts, they added a 5 minute break in the middle of the shift so emergency providers could either partake in art therapy (colouring a provided mandala) or dog therapy with their hospital’s therapy dogs. The control group wasn’t perfect, and the results are somewhat mixed, but stress over the course of the shift did seem to decrease in the dog therapy group. The results aren’t strong enough that we should all be running out to invest in departmental dog therapy programs, but I think the study is a nice reminder of the value of a 5 minute break during our crazy stressful jobs. I try to ensure I take 5 to 10 minutes completely away from the clinical area to reset in the middle of each shift.
I include my commentary just so I can share a completed example of the art therapy side of the study. Unfortunately, Jeff’s publication did not include any pictures of the therapy dogs, which was a major oversight.

If this type of paper interests you, you might also like the paper that looked at using art therapy to decrease anxiety for patients:
Rajendran N, Mitra TP, Shahrestani S, Coggins A. Randomized Controlled Trial of Adult Therapeutic Coloring for the Management of Significant Anxiety in the Emergency Department. Acad Emerg Med. 2020;27(2):92‐99. doi:10.1111/acem.13838 PMID: 31957143
This is a small RCT in which 53 patients presenting to the emergency department with anxiety were randomized to either art therapy (a colouring pack with 10 mindfulness coloring book images and 36 colored pencils) or placebo (a pack with pens and blank paper). The mean decrease in the HADS-A anxiety scale at 2 hours was 3.7 in the art therapy group and 0.3 with control (0<0.001). The study is imperfect, being a small single center trial using a convenience sample, but considering the limited potential harms and relatively low cost of this non-pharmacologic intervention for anxiety, it might be worth trying in some settings.
You spin me right round, baby
Right round like a record, baby
Right round round round
Azad T, Pan G, Verma R. Epley Maneuver (Canalith Repositioning) for Benign Positional Vertigo. Acad Emerg Med. 2020;10.1111/acem.13985. doi:10.1111/acem.13985 PMID: 32281203
This is part of the new series of “Brass Tacks reviews” from Academic Emergency Medicine in collaboration with theNNT.com. This paper summarizes a recent Cochrane review on canalith repositioning for BPPV. The Epley maneuver results in a remarkable 35% absolute reduction in symptoms compared to a sham procedure or control, or a NNT of 3. There were no serious harms reported. The evidence is far from perfect, with only 5 trials encompassing 273 patients looking at the Epley maneuver (and most trials were in an ENT office not the emergency department). However, they were all RCTs with decent controls and low risk of bias, so although imperfect, the level of evidence is a lot better than for many things we do in medicine. My problem with this paper is their focus on the Epley maneuver. I know that this is the maneuver that everyone was taught in medical school, but it is much more difficult to perform than the other canalith repositioning maneuvers, and the Cochrane review did not find any difference between the different respositing maneuvers. I use the Semont maneuver. Watch the videos below and you will see why. It is so much easier to perform, and patients can easily do this for themselves at home.
One component of BPPV that I was never taught: how do we prevent it from recurring as soon as the patient goes home? You do all this work to get the canalith back to the right spot, but then the patient turns their head and the problem starts all over again. A pearl I was taught by a physiotherapist was to give the patient a soft cervical collar to wear for 24 hours to prevent big movements of the head that might shift the canalith back to the problem position. I don’t think there is any evidence supporting the practice, but it seems relatively low cost and harm free, so it might be worth a try.
Bottom line: When you diagnose BPPV, the treatment should include a canalith repositioning maneuver. Personally, I think the Semont is better than the Epley.
You can find the NNT review (with a green light) here.
HYVCTTSSS
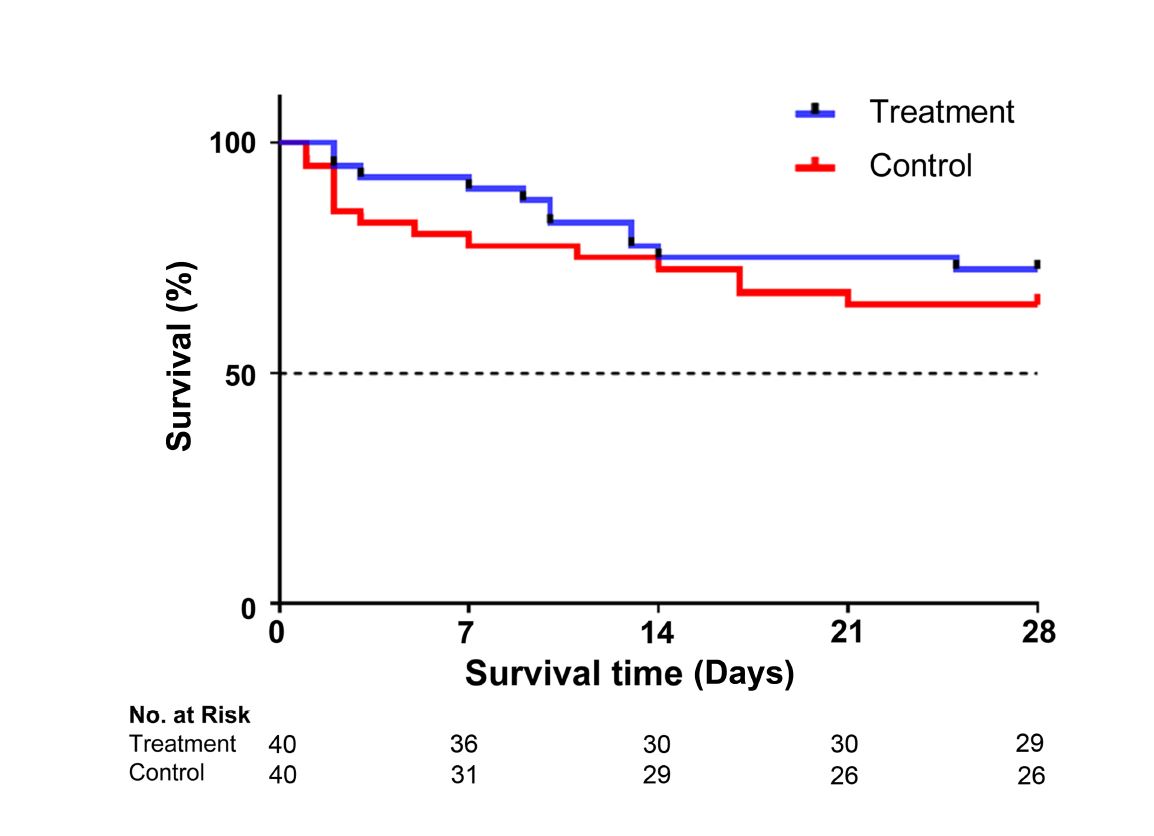
HYVCTTSSS: Chang P, Liao Y, Guan J, et al. Combined treatment with hydrocortisone, vitamin C, and thiamine for sepsis and septic shock (HYVCTTSSS): A randomized controlled clinical trial. Chest. 2020;S0012-3692(20)30552-3. doi:10.1016/j.chest.2020.02.065 PMID: 32243943
Aside from having one of the best trial names of all time (it sounds a little like a Trump covfefe tweet), this trial is not great. However, it is a fine excuse to get caught up on the vitamin C for sepsis evidence. (There is a post that covers all the trials here.) After a somewhat unbelievable before/after chart review showed a 16% reduction in mortality when giving vitamin C, thiamine, and hydrocortisone to septic patients in the ICU, there has been a lot of interest in this ‘metabolic cocktail’. This is the third RCT of the last year, and like the other two, it was negative. HYVCTTSSS randomized patients with severe sepsis or septic shock (plus a procalcitonin level >2) to either the metabolic cocktail (vitamin C 1.5 grams q6h, thiamine 200 mg q12h, and hydrocortisone 50 mg q6h) or saline (although 28 of the 40 patients in the placebo group didn’t even receive the placebo, which is a marker of the poor methodology here.) The trial was stopped early for harm (increased hypernatremia in the treatment group). There was no statistical difference in mortality between the groups (28% with treatment and 35% with control; p=0.47), but the trial is woefully underpowered to make any conclusions. As I said, the two other RCTs were also negative.
Bottom line: It is incredibly unlikely that this treatment reduces mortality, but none of the RCTs are definitive, so we can’t completely rule out the possibility of a benefit yet.
UOAIAAAIAOU
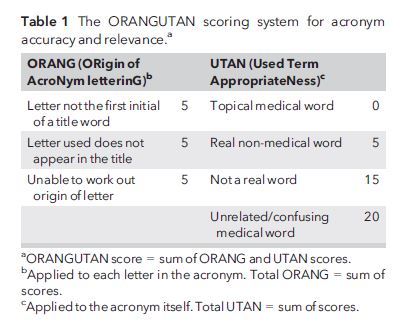
Weale J, Soysa R, Yentis SM. Use of acronyms in anaesthetic and associated investigations: appropriate or unnecessary? – the UOAIAAAIAOU Study. Anaesthesia. 2018;73(12):1531‐1534. doi:10.1111/anae.14450 PMID: 30412290
I have been sitting on this paper for 2 years. I almost include it with every edition, but then it gets bumped for something more relevant. (I know that might surprise some readers, but I do try to make the papers relevant.) However, with the publication of the brilliant HYVCTTSSS trial, this paper clearly shines. Noting the rising use of acronyms in medical studies, these authors set out to describe their use and usefulness in anesthesia related studies. They developed the ORANGUTAN score to rate the quality of acronyms. It is divided into 2 parts. Part 1 is the ORAN (ORigin of AcroNym letterinG) score, in which you get 5 points for any of: “letter not the first initial of a title word”, “letter used does not appear in the title”, and “unable to work out origin of letter”. Part 2 is the UTAN (Used Terms AppropriateNess) score, in which you get 0 points for a topical medical word, 5 points for a non-medical word, 15 points for not being a real word, and 20 points for being an unrelated or confusing medical word. The HYCTTSSS trial gets almost a perfect score! Among the confusing acronyms they encountered, there were “unrelated studies for which the authors had independently chosen identical acronyms, two substudies labelled with a novel acronym to describe their secondary analyses and one instance where a study group with multiple publications, using the same acronym and dataset, have become confused by their own acronym and started publishing with a different one!”
Bottom line: Knowledge translation in science should not be based on how catchy an acronym you were able to create. The study acronyms are a lot like brand names for drugs. They are easier to say and remember, but distract us from the truly important details.
Will plaster disappear from EDs before I retire?
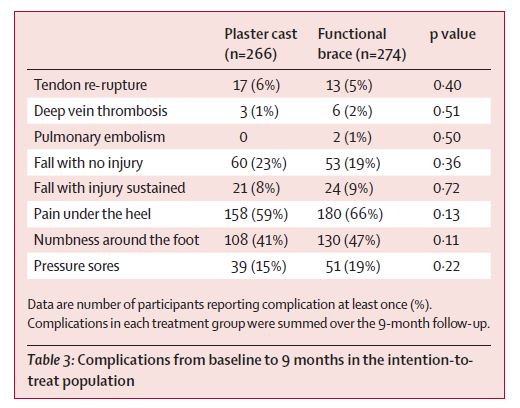
UKSTAR: Costa ML, Achten J, Marian IR, et al. Plaster cast versus functional brace for non-surgical treatment of Achilles tendon rupture (UKSTAR): a multicentre randomised controlled trial and economic evaluation. Lancet. 2020;395(10222):441‐448. doi:10.1016/S0140-6736(19)32942-3 PMID: 32035553 [free full text]
This is a pragmatic, multicentre, randomized, controlled trial from 39 hospitals in the United Kingdom looking to compare functional outcomes, quality of life, and complications with a removable walking boot versus plaster cast after Achilles tendon rupture. They included adult patients with a first time Achilles tendon rupture, excluding those presenting more than 14 days after the injury. The plaster cast was the classic gravity equinus position. To recreate a similar plantar flexion position, they inserted 2 solid heel wedges in the removable walking boot. The walking boot group was allowed to mobilize with full weight bearing immediately. They included 540 patients, although unfortunately another 385 simply declined to participate, making selection bias a concern. As expected, these are predominantly males with a mean age of 49 who ruptured their Achilles tendon playing sport. There was no statistical or clinical difference in the primary outcome, which was a tendon rupture specific quality of life scale. Some secondary quality of life scales were statistically better in the splinting group at 8 weeks but not after that. (This makes sense, as the value of a removable splint is really early comfort and mobility, but the differences seen were really small.) Costs were not different between the groups. Probably most importantly, the rate of rerupture was the same in both groups (6% with plaster vs 5% with a boot). I didn’t know the rerupture rate was so high, so that is a helpful piece of information when counselling my patients, or gambling on the NBA next season. One fascinating thing about this study, that you almost never see, is that they actually stopped it late rather than early. Recruitment was faster than expected, so they included more patients to specifically look for harms. Kudos to these authors.
Bottom line: Considering that I am just about the age where my achilles could rupture if I decide to start playing basketball again, I will keep this paper in my back pocket. Personally, I would much rather a walking boot to a plaster cast if the outcomes are going to be the same.
You don’t even need the dark web
Blok D, Ambrose L, Ouellette L, et al. Selling poison by the bottle: Availability of dangerous substances found on eBay®. Am J Emerg Med. 2019;S0735-6757(19)30608-4. doi:10.1016/j.ajem.2019.09.024 PMID: 31862190
Want to buy some poison? No need to leave home. eBay has all your toxicology needs. These authors searched eBay weekly for 8 months using the term “poison bottle”. These are often sold as collectors items, because poison used to be sold in brightly coloured glass bottles, before we realized those bright colours made them more attractive to children. I would have expected the bottles to be empty, but they found 283 product listings, half of which were completely full, and the remaining were partially full. More than half contained products classified as extremely toxic, like mercury, arsenic, or cyanide. This is likely an underestimate of what is available, as they only used one search term, and only based their results on the listed ingredients. A bottle with an unknown liquid could clearly be deadly, but wasn’t included in these results. Of course, the active ingredients of many of these bottles may have significantly degraded with time, but it is still somewhat concerning how easily these are sold (we are talking about eBay, not the dark web).
Bottom line: Keep up to date on your toxicology. We will never be out of a job.

I like my grey matter on the rocks
The HYPERION Trial: Lascarrou JB, Merdji H, Le Gouge A, et al. Targeted Temperature Management for Cardiac Arrest with Nonshockable Rhythm. The New England journal of medicine. 2019; 381(24):2327-2337. PMID: 31577396 [full text]
Most people are well aware of the two small RCTs that birthed the practice of hypothermia for cardiac arrest, and the large TTM trial that followed. If you aren’t, I review them in this post. However, it isn’t clear to me whether people are aware that hypothermia might be controversial. We spend a lot of time talking about the weaknesses in the data for tPa for stroke, or Tamiflu for influenza, but in my experience hypothermia has sort of got a pass. Needless to say, I have always remained (appropriately, I think) skeptical.
This is an open-label, pragmatic, multi-centre RCT that enrolled 584 comatose adult patients with ROSC after cardiac arrest (both in and out of hospital) with a non-shockable rhythm. They compared hypothermia with a target of 33 degrees to controlled normothermia with a target of 37 degrees. For the primary outcome of survival with good neurologic outcome, the hypothermia group fared better (10% vs 6 %) but the p value was only 0.047 with a fragility index of 1, which is especially problematics in an open label trial, which significantly increases the risk of bias. Perhaps the biggest problem with this trial is that a large number of the patients in the “normothermia” group actually became febrile, so it is impossible the distinguish benefit from hypothermia and harm from hyperthermia.
How you interpret this trial will depend in large part on what you thought about the evidence for hypothermia before this trial came out. I review the previous major hypothermia trials in this post, if you want a review of all the evidence. Overall, this trial marginally increased my belief that hypothermia could provide a benefit, but even with that increase, I think it is more likely that we will ultimately discover that there is no benefit.
Bottom line: This RCT provides some weak evidence that hypothermia or temperature control may improve neurologic outcomes in patients with non-shockable rhythms.
Glucagon – tough to swallow
Long B, Gottlieb M. Is Glucagon Effective for Relieving Acute Esophageal Foreign Bodies and Food Impactions?. Ann Emerg Med. 2020;75(2):299‐301. doi:10.1016/j.annemergmed.2019.03.033 PMID: 31080031
This is a snapshot review of a systematic review and meta-analysis looking at glucagon for esophageal food bolus. We have covered this before, but I continue to get asked by specialists to give my patients medications we know are harmful, so I guess we’d better cover it again. They found 5 papers (2 RCTs and 3 retrospective controlled trials). The risk of bias was rated as low in the 2 RCTs. The results confirm what we knew: glucagon has no benefit (30% vs 33% relief of esophageal impaction). However, there is a significant increase in harm (15% with glucagon compared to 0% with control). Most of the harm is vomiting and retching, but there was also some hypotension and lightheadedness. The majority of these patients had pathology found at endoscopy, so even if glucagon worked (it doesn’t) you wouldn’t be preventing the need for a procedure.
Bottom line: The treatment for esophageal food bolus is endoscopy. Medical management should not be attempted, as the current evidence, although limited, clearly suggests that harms outweigh benefits.
Cheesy Joke of the Month
Why don’t ants get ill? Because they have antibodies.
Morgenstern, J. Research Roundup – June 2020, First10EM, June 22, 2020. Available at:
https://doi.org/10.51684/FIRS.26183