
Morgenstern, J. How should we irrigate lacerations? Does it even matter?, First10EM, November 7, 2022. Available at:
https://doi.org/10.51684/FIRS.128617
In part 2 of the laceration evidence series, we are going to tackle all of the evidence around wound irrigation and cleansing. The value of irrigation seems pretty obvious. Traumatic wounds are contaminated, and we should do our best to clean them. “The solution to pollution is dilution.” Therefore most of the (relatively limited) evidence focuses on exactly how we should irrigate. That being said, we should always question our assumptions, so in addition to questions about how we should be irrigating, we will also consider the very basic question of whether irrigation helps at all.
Does irrigation matter at all?
Irrigation of traumatic wounds seems like an obvious necessity. The wounds are dirty. We can probably assume that rinsing the dirt out helps. That being said, digging into the science often demonstrates some major flaws in my assumptions. Honestly, I sort of expected this section to be completely empty, but to my surprise, there are at least five studies that asked: is irrigation even necessary?
The first is a prospective observational study of 1923 facial and scalp lacerations, excluding patients with immunocompromise, diabetes, renal disease, or who presented more than 6 hours after their injury. (Hollander 1998) At the discretion of the treating physician, 1090 were irrigated and 833 were not. In this department, almost all irrigation was done with normal saline, and a syringe was the most common technique. The wound infection rate was not statistically different, at 0.9% in the irrigation group and 1.4% in the no irrigation group (ARR 0.5%, 95% CI 1.5% to -0.5%; p=0.28). Cosmetic outcomes were also not different, although they report a ‘trend’ towards worse outcomes with irrigation based on a p-value of 0.07. Of course, the fundamental issue with this trial is the lack of randomization. I imagine people chose to irrigate wounds with obvious contamination, and skipped that step in clean wounds, significantly biasing the results. (The data can’t say irrigation doesn’t help, but it does suggest that doctors are good at selecting a subset of wounds that don’t require irrigation.) The other big issue with this study is the inclusion of only face and scalp wounds, which almost never get infected. If their rate of infection was going to be close to 0 no matter what they did, the trial was biased to show no difference, and the result may not generalize to other areas of the body. On the other hand, we see a lot of these kinds of wounds, and it’s nice to know that you probably don’t need to dump buckets of water on the face of the poor child with an eyebrow laceration.
Luckily, we don’t have to rely solely on observational data. A 2012 Cochrane review looking at wound irrigation with water found 3 RCTs comparing water irrigation to no cleansing at all, and there was no difference in the rate of infection, although with massive confidence intervals and therefore a very high degree of uncertainty (RR 1.06, 95% CI 0.07 to 16.5). (Fernandez 2012)
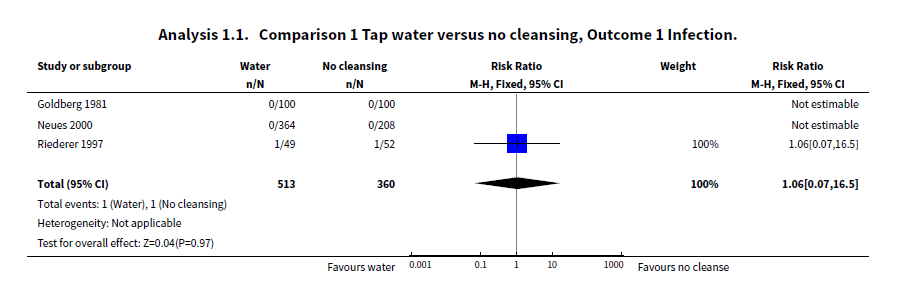
Edit Jan 2023: It has been pointed out to me that I misinterpreted this Cochrane review. (Thank you Kyle.) This review is looking at aftercare, comparing wound cleansing to no wound cleaning. It is not looking at irrigation at the time of initial management. Edit Jan 2025: Actually, I think this comment is incorrect. I have reviewed the citations, and there are definitely included studies that look only at irrigation prior to laceration repair. I think the confusion is that the review includes both. There is an updated Cochrane review in 2022 with more studies, but the same result. (Fernandez 2022)
If you want to extrapolate from the surgical literature, there is a systematic review of 4 RCTs comprising 1194 patients that found no statistical difference in surgical site infections with saline wound irrigation, although the difference might have been big enough to be clinically important (risk ratio 0.73, 95% CI 0.37 to 1.43), so there is obviously still a lot of uncertainty. (Ambe 2020) For the most part, I have tried to avoid this extrapolation, because I think it fails in both directions. Most surgical wounds are sterile, so we should expect low infection rates, and therefore almost any intervention should fail. However, when surgical wounds become contaminated, they are more likely to be contaminated with pathogens, and so interventions might be more important. Considering how common traumatic lacerations are, it seems like we should develop evidence specific to emergency department patients where such evidence doesn’t exist.
Bottom line: I was surprised that data existed at all, but the evidence we have is still severely limited. There is no evidence of benefit from irrigation. However, there is definitely not enough evidence to prove that irrigation is unnecessary. Personally, I still consider irrigation part of my usual care, but this data tells me that clinical judgment is probably enough to select a group of patients with a low rate of infection who don’t require irrigation (which is probably what we have all been doing anyway).
Does pressure matter?
Textbooks and review articles usually suggest specific volumes of irrigant and specific pressures. However, most citations seem to point to laboratory research or animal models, which have a history of not translating well into clinical trials involving humans. My focus is only clinical evidence.
There is one study, with very questionable methodology, and it is only presented in a letter to the editor. (Longmire 1987) It is a single center study of 335 emergency patients with lacerations. Randomization was mostly done by coin flip, but if the physician was wearing gloves, they spun a scalpel instead. (If you were wondering, this is not considered an ideal randomization procedure). There was no blinding, and a huge proportion of patients were lost to follow-up, with a statistically significant difference in loss to follow-up between the groups. The trial compared irrigation with normal saline using a bulb syringe (low pressure) to normal saline using a syringe system targeting 13 psi. There was a statistically significant decrease in infections in the high pressure group (6.9% versus 1.3%, p=0.017), but considering they lost more than 4 times as many patients as had their primary outcome and the trial was non-blinded, I don’t think these results mean much.
Based on the premise that more pressure, and more consistent pressure, is better, a device called “Dey-Wash” was developed, which is a 220 mL canister of saline pressurized with propellant. This was compared to normal saline irrigation using a 30 mL syringe and a 20 gauge catheter in a multi-centre RCT including 542 emergency department patients with simple lacerations. (Chisholm 1992) Although this new device was somewhat faster, there was no difference in wound complications: 3.6% with the syringe and 5.0% with the device, p=0.5.
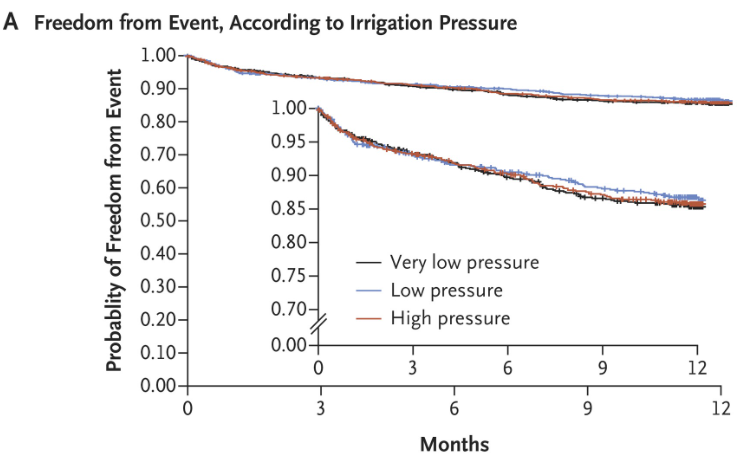
Open fractures are obviously very different from simple lacerations, so I am hesitant to include this trial. However, the FLOW trial is by far the best RCT on pressure irrigation I could find. (Not surprising when Gordon Guyatt is the senior author.) They randomized 2551 patients with open fractures to high pressure (>20psi), low pressure (5-10 psi), or very low pressure (1-2 psi) irrigation with either castile soap or normal saline. (FLOW 2015) There were no differences at all based on pressure. (The soap group had slightly worse outcomes, based on a composite, than the saline group.)
I have seen a number of review papers talk about an increased risk of infection due to tissue damage if high pressure irrigation is used. However, the only study that I have seen cited seems to be an animal study, which does say there was tissue damage, but says “the remarkable cleansing capacity of high pressure irrigation appears to outweigh this side-effect, since heavily contaminated wounds subjected to this treatment heal per primum without infection”. (Wheeler 1976) I can’t verify these claims, as I can’t find a copy of the paper, but I don’t think a study of a couple pigs from 1976 should be influencing clinical practice in 2022.
The RCT from 1987 demonstrated a clinically important difference, but the methodology is so poor that I don’t trust the results. Personally, my practice is heavily influenced by the FLOW study, as I imagine that if pressure was important, it would be even more important in open fractures than it is in simple lacerations. (My thinking is also supported by the studies demonstrating that tap water is equivalent to other forms of irrigation, which we will discuss below). Furthermore, it would be very hard for pressure to matter if irrigation itself is unnecessary.
Bottom line: The evidence around pressure for irrigation is very underwhelming, and I don’t think we should draw firm conclusions, but I personally doubt pressure matters.
How much volume is needed?
It is very common to see recommendations to use approximately 50 to 100 mL of irrigation for every centimeter of the laceration. (Nicks 2010; Forsch 2017) However, I have followed citations as far as I can in every paper and textbook in which I encountered this recommendation, and I can’t find a single clinical trial to support the recommendation. (As a side note, for the love of god, if you include a citation in a review paper or a textbook chapter, please ensure the citation has something to do with the claim you are making. Too many citations seem to have been produced by a random number generator.)
Bottom line: There is no clinical data to guide how much irrigation is enough. If no irrigation is needed at all, it wouldn’t be surprising that studies looking at the volume and pressure show no benefit. If I am irrigating a wound, I use at least as much water as I would if I was washing my hands, and definitely don’t stop until all visible contamination is gone.
Does it matter what we irrigate with?
There are so many options when it comes to irrigation, it is hard to summarize them all succinctly. Most emergency physicians have moved towards tap water, which I will cover in its own section below. Before getting there, let’s consider the various anti-septic options available, such as chlorhexidine and povidone-iodine.
In a single center, non-randomized (treatment assigned by month) trial of 531 patients with simple lacerations, normal saline irrigation was compared to both a 1% povidone-iodine solution and a 1% pluronic-F68 (Shur-Clens). (Dire1990) There was no statistical difference in infection, with 6.9% of the saline group, 4.3% of the povidone-iodine group, and 5.6% of the Shur-Clens group having infections at follow-up. Being non randomized, this is a low quality study. A 2.6% absolute difference in infection rate would be clinically important, but I have little faith in these results.
A single centre, quasi-randomized trial of 418 patients with hand laceration requiring sutures, randomized patients to either have povidone iodine (in a dry powder form) applied to the wound or not. (Roberts 1985) There were no differences in infection (4.6% vs 5.3%) or imperfect healing (36% vs 41%). Unfortunately, in addition to the fact that more than 25% of patients were lost to follow-up, all wounds were cleaned with chlorhexidine prior to this application, and then debrided, so I don’t think the results tell us all that much.
Another study of this dry powdered povidone iodine spray, which is actually rather complicated because it seems to be embedded into another study of whether antibiotics are helpful, looked at 631 patients from a single emergency department. (Naunton Morgan 1980) All patients had ‘toilet’ performed to the wounds, which is not further described. It seems like there might be a difference, but it is hard to summarize because there are 4 different groups. There was not a statistical difference in patients with head and neck wounds, but there was in both groups with lacerations to the hands and forearm. My big concern is that the infection rate in the control group seems incredibly high here (almost 20%), whereas the treatment group has an infection rate that is more consistent with the rest of the literature, at around 5%. I am also not sure how dry povidone iodine spray compares to irrigation with the same.
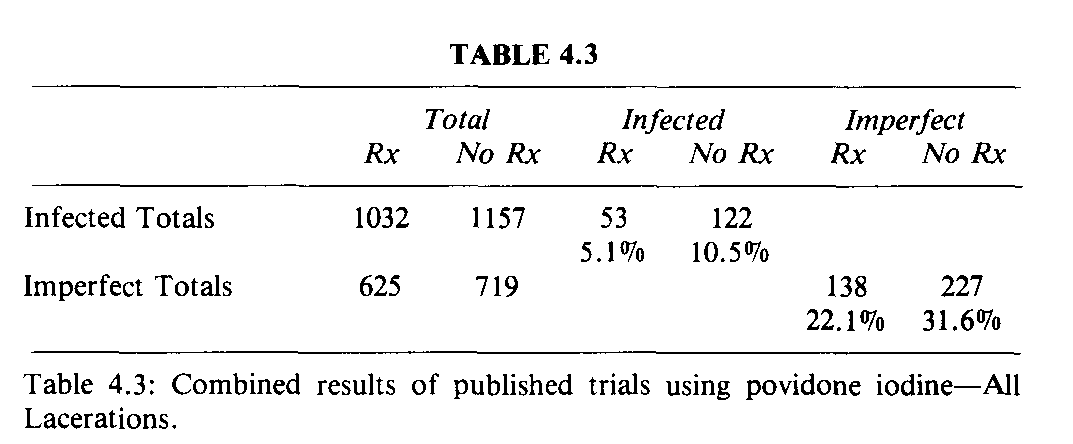
There are a handful of seemingly similar studies from the late 1970s and early 1980s that I can’t get copies of. (Bickerstaff 1984, Gosnold 1977, Gosnold 1979, Morgan 1979) They all look at the use of povidone iodine, but mostly in powder form rather than as irrigation. Roberts (1985) provides a table with a summary of their results, in which there does seem to be a benefit (5% vs 10% infections, which is statistically significant when I plug it into online calculators). However, basic numbers obviously don’t tell us about potential biases, and therefore the certainty of this result. Based on the studies I have access to, I imagine this is low certainty evidence.
Gravett (1987) is a single centre RCT of 500 emergency department patients with lacerations requiring sutures. In the treatment group, they instilled 1% povidone-iodine into the wound, and rubbed it in for 60 seconds with gauze. The control group did not receive this step, but both groups had their wound cleaned with the antiseptic benzalkonium chloride, and both groups also had the skin outside the wound cleaned with povidone-iodine. Given that both wounds were cleaned with an antiseptic, I was surprised that the infection rate was significantly lower in the povidone-iodine group (5% vs 15%, p<0.01). To further complicate matters, both groups had antibiotic ointment applied, which could limit any difference caused by the povidone-iodine. Once again, the infection rate in the control group seems astronomically high. Also, they lost more than 20% of their patients to follow-up (maybe people were upset with how many infections this ED was causing?)
In a single-blind RCT looking at simple traumatic lacerations in 444 ED patients over the age of 16, with similar exclusion criteria to all these studies, normal saline was compared to povidone iodine. (Ghafouri 2016) This is not actually a study of irrigation. All of the wounds were irrigated with normal saline. In the povidone iodine group, they just cleaned the surrounding skin after irrigation. The stats are funny in this study, but they did not find a statistically significant difference between the groups. Obviously, the study isn’t relevant, as it doesn’t look at irrigation with povidone iodine – but it is often cited as if it does, so I decided to include it here.
In another single center RCT, patients with heavily contaminated (visible particulate matter) wounds requiring debridement were randomized to one of three groups. (Lammers 1990) In the first, wounds were soaked for 10 minutes in 1% povidone-iodine. In the second group, wounds were soaked for 10 minutes in normal saline. In the third group, no treatment was performed. The primary outcome of this trial was a surrogate outcome looking at bacterial counts before and after treatment. I believe their original outcome was the number of patients with what they considered enough bacteria to cause an infection. Both saline and povidone-iodine decreased the number of patients with this threshold from 80% to 60%, while the no treatment group stayed the same. However, they added another outcome, looking at total average bacterial counts, and in the saline group counts went way up. They did look for clinical outcomes based on chart review (so very low certainty), and they say that 13% of the control group, 13% of the povidone iodine group, and 71% of the saline group ended up with wound infections. I don’t think you can take much from this study. First, they were soaking rather than irrigating. Second, the numbers are tiny. (That 71% infection rate with saline just means 5 of 7 patients had infections. Add to that the fact this is a single-centre, non-blinded trial, with no description of randomization or allocation concealment techniques, and these results are next to meaningless.
A 2016 review of chlorhexidine for wound management found no relevant clinical evidence. (Wound Healing and Management Node Group 2016) There are lab and animal studies only. They conclude “there is insufficient evidence on the safety of and effectiveness of chlorhexidine in reducing bio-burden and promoting wound healing in concentrations designed for wound care (i.e. 0.05% or more dilute) to make a recommendation on its use as a wound care product.” This review was looking at all wounds, not just lacerations, but it fits with what I could find, which is essentially nothing that convincingly guides our practice.
A 2022 systematic review found the same studies I did, so I think this is all of the evidence we have to go one, which is obviously not enough to make any kind of definitive conclusions. (Soeselo 2022)
Many have raised concerns that antiseptics might be damaging to tissues and therefore impair healing, but I don’t find the citations used all that convincing. For example, one of the most commonly cited articles is Brennan (1985), which used a rabbit ear model, and did show changed in blood flow with some antiseptics that lasted many days, but there were no effects from chlorhexidine or low concentration povidone iodine, so I doubt these changes seen in an animal model really mean anything clinically.
Since I was a medical student, I have been told that it is inappropriate to use povidone-iodine or chlorhexidine to clean wounds. I was told it impaired healing and caused tissue damage. That claim seems to be way over-stated, and the best available evidence (which is very limited) actually seems to suggest that povidone-iodine might decrease infection rates.
Bottom line: The evidence for irrigation with antiseptics is very poor. That being said, I see no evidence of harm (which I have often been told is the case), and the early trials using a povidone-iodine powder suggest a possible benefit. We are left with significant uncertainty. I do not use antiseptics routinely, but after reading this literature, I will probably start using povidone-iodine in cases where I am worried about infection (contaminated wounds in patients with diabetes, for example).
Tap water for irrigation
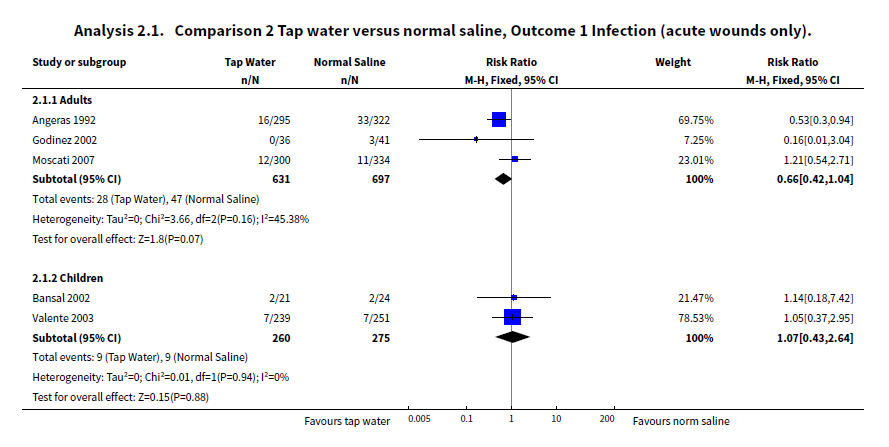
There have been a number of studies looking at simple tap water for wound irritation. As mentioned above, a 2012 Cochrane review found that tap water was no different from no cleansing at all. (Fernandez 2012) The same review found 7 trials comparing tap water to saline. For acute wounds, the use of tap water was not statistically different from saline, but the relative risk of 0.66 could be clinically important and favored tap water (95% CI 0.42-1.04, p=0.07). The same review looked at distilled and boiled water, with no statistical differences, but there was only a single trial, and the numbers are way too small to draw conclusions with any certainty.
The highest quality study is a single-centre, double-blind RCT that enrolled 663 patients with uncomplicated lacerations (excluding patients with any immunocompromise, current use of antibiotics, bone or tendon involvement, and wounds greater than 9 hours old). (Weiss 2013) Wounds were all irrigated with 500 mL at 8 psi (through a 35 mL syringe attached to a 18 gauge IV), and tap water was compared to normal saline. There was no statistical difference in infections between the groups, but again tap water looks a little better (3.5% vs 6.4%, ARR 2.9%, 95% CI -0.4% to 5.7%). The biggest problem with the study is probably that the definition of infection is subjective, but that should have a limited impact given the double-blind nature of this trial with excellent randomization procedures.
Based on some very rough calculations, I believe that when the Cochrane review is updated to include this trial, the benefit from tap water will now be statistically significant. (If someone with the statistical skill wants to do this meta-analysis with me, let me know.) Even if the difference is not statistically significant, tap water is pretty clearly not going to be any worse than saline, and when factoring in cost (let alone the environmental impact of throwing out all those plastic bottles than saline comes in), I imagine it comes out as the clear winner.
As far as I can tell, tap water has never been compared directly with povidone-iodine.
These findings make sense, as the tap water at most hospitals where this kind of research is being performed is very unlikely to contain pathogenic bacteria. In fact, one study looked at this exact question, collecting tap water from difference areas in the department, and they did not isolated any pathogenic bacteria. (Riayt 1997) I would imagine the safety of tap water depends a lot on the infrastructure of the community you live in. Even in Canada, we have many communities with tap water that is unsafe for drinking, and I would not try to extrapolate these results to those communities. However, for the average modern city, our tap water is safe for both drinking and cleaning wounds (but preferably not at the same time).
Bottom line: Tap water is definitely no worse than saline, and may in fact be better. When you consider the costs and environmental impacts of sterile saline, tap water is almost certainly better. The most interesting part of this data is that, based on the limited data we have, tap water irrigation is also no different than no irrigation at all, which really does raise questions of the value of irrigation in general.
Discussion
All of these studies are interdependent, which adds significant complexity. If the volume or pressure of irrigation matters, studies looking at the type of irrigant may give us false results if they used inappropriate volumes or pressures. Conversely, we may not be able to demonstrate the value of a specific volume or pressure if we are using the wrong irrigant. Therefore, despite the largely negative trials, there is still plenty of room for research. Practically speaking, though, these studies generally look like usual practice, which tends to indicate your choices around irrigation are largely irrelevant. Basically everything results in similar outcomes for our patients, based on the limited evidence we have right now.
Of course, it is important to be cognizant of the limitations of our evidence. All of these studies are small, and despite not being statistically significant, some of the differences might be clinically significant. A single large, high quality RCT could easily over-rule everything we have to date. (And the combined data on povidone-iodine is probably enough for me to increase use in my practice.)
Perhaps more importantly, these studies excluded a large proportion of the population we treat. Patients with older wounds, diabetes or any form of immunosuppression, complex wounds, or heavily contaminated wounds were largely excluded. That doesn’t mean that irrigation will help those populations, but it means that we don’t know. I treat a lot of lacerations without irrigation, but the higher the chance the wound has of becoming infected, the more effort I put into clearing it, even if it is all theatrics for the patient.
The paucity of evidence on this topic is actually somewhat embarrassing for our specialty. This is one of the most common things we see. We could have enough patients for an RCT in just a few months. This is something we just need to get done.
“The assessment and protocol of management [of lacerations], however, seems ritualistic rather than evidence based.” (Khan 2006)
Other FOAMed
TheNNT.com – Tap Water vs. Sterile Saline for Wound Irrigation
EM Docs: Antediluvian Methods? An Evidence-Based Approach to Wound Irrigation
Tap Water or Sterile Saline for Acute Laceration Irrigation?
References
Ambe PC, Rombey T, Rembe JD, Dörner J, Zirngibl H, Pieper D. The role of saline irrigation prior to wound closure in the reduction of surgical site infection: a systematic review and meta-analysis. Patient Saf Surg. 2020 Dec 22;14(1):47. doi: 10.1186/s13037-020-00274-2. PMID: 33353558
Bickerstaff KI, Regnard C. Prophylactic povidone-iodine spray in accidental wounds. J R Coll Surg Edinb. 1984 Jul;29(4):234-6. PMID: 6384493
Brennan SS, Leaper DJ. The effect of antiseptics on the healing wound: a study using the rabbit ear chamber. Br J Surg. 1985 Oct;72(10):780-2. doi: 10.1002/bjs.1800721004. PMID: 4041708
Chisholm CD, Cordell WH, Rogers K, Woods JR. Comparison of a new pressurized saline canister versus syringe irrigation for laceration cleansing in the emergency department. Ann Emerg Med. 1992 Nov;21(11):1364-7. doi: 10.1016/s0196-0644(05)81903-1. PMID: 1416333
Dire DJ, Welsh AP. A comparison of wound irrigation solutions used in the emergency department. Ann Emerg Med. 1990 Jun;19(6):704-8. doi: 10.1016/s0196-0644(05)82484-9. PMID: 2344089
Fernandez R, Griffiths R. Water for wound cleansing. Cochrane Database Syst Rev. 2012 Feb 15;(2):CD003861. doi: 10.1002/14651858.CD003861.pub3. Sep 14;9:CD003861. PMID: 22336796
Fernandez R, Green HL, Griffiths R, Atkinson RA, Ellwood LJ. Water for wound cleansing. Cochrane Database Syst Rev. 2022 Sep 14;9(9):CD003861. doi: 10.1002/14651858.CD003861.pub4. PMID: 36103365; PMCID: PMC9473482.
FLOW Investigators, Bhandari M, Jeray KJ, Petrisor BA, Devereaux PJ, Heels-Ansdell D, Schemitsch EH, Anglen J, Della Rocca GJ, Jones C, Kreder H, Liew S, McKay P, Papp S, Sancheti P, Sprague S, Stone TB, Sun X, Tanner SL, Tornetta P 3rd, Tufescu T, Walter S, Guyatt GH. A Trial of Wound Irrigation in the Initial Management of Open Fracture Wounds. N Engl J Med. 2015 Dec 31;373(27):2629-41. doi: 10.1056/NEJMoa1508502. Epub 2015 Oct 8. PMID: 26448371
Forsch RT, Little SH, Williams C. Laceration Repair: A Practical Approach. Am Fam Physician. 2017 May 15;95(10):628-636. PMID: 28671402
Ghafouri HB, Zare M, Bazrafshan A, Abazarian N, Ramim T. Randomized, controlled trial of povidone-iodine to reduce simple traumatic wound infections in the emergency department. Injury. 2016 Sep;47(9):1913-8. doi: 10.1016/j.injury.2016.05.031. Epub 2016 May 24. PMID: 27269416
Gosnold JK. Infection rate of sutured wounds. Practitioner. 1977 Apr;218(1306):584-5. PMID: 859805
Gosnold JK. Prophylaxis of wound infection. Practitioner. 1979 Aug;223(1334):271-3. PMID: 388404
Gravett A, Sterner S, Clinton JE, Ruiz E. A trial of povidone-iodine in the prevention of infection in sutured lacerations. Ann Emerg Med. 1987 Feb;16(2):167-71. doi: 10.1016/s0196-0644(87)80008-2. PMID: 3800090
Hollander JE, Richman PB, Werblud M, Miller T, Huggler J, Singer AJ. Irrigation in facial and scalp lacerations: does it alter outcome? Ann Emerg Med. 1998 Jan;31(1):73-7. doi: 10.1016/s0196-0644(98)70284-7. PMID: 9437345
Khan MN, Naqvi AH. Antiseptics, iodine, povidone iodine and traumatic wound cleansing. J Tissue Viability. 2006 Nov;16(4):6-10. doi: 10.1016/s0965-206x(06)64002-3. PMID: 17153117
Lammers RL, Fourré M, Callaham ML, Boone T. Effect of povidone-iodine and saline soaking on bacterial counts in acute, traumatic, contaminated wounds. Ann Emerg Med. 1990 Jun;19(6):709-14. doi: 10.1016/s0196-0644(05)82486-2. PMID: 2344090
Longmire AW, Broom LA, Burch J. Wound infection following high-pressure syringe and needle irrigation. Am J Emerg Med. 1987 Mar;5(2):179-81. doi: 10.1016/0735-6757(87)90121-5. PMID: 3828025
Morgan WJ. The effect of povidone-iodine (Betadine) aerosol spray on superficial wounds. Br J Clin Pract. 1979 Apr;33(4):109-10. PMID: 475952
Naunton Morgan TC, Firmin R, Mason B, Monks V, Caro D. Prophylactic povidone iodine in minor wounds. Injury. 1980 Sep;12(2):104-6. doi: 10.1016/0020-1383(80)90132-1. PMID: 7009430
Nicks BA, Ayello EA, Woo K, Nitzki-George D, Sibbald RG. Acute wound management: revisiting the approach to assessment, irrigation, and closure considerations. Int J Emerg Med. 2010 Aug 27;3(4):399-407. doi: 10.1007/s12245-010-0217-5. PMID: 21373312
Riyat MS, Quinton DN. Tap water as a wound cleansing agent in accident and emergency. J Accid Emerg Med. 1997 May;14(3):165-6. doi: 10.1136/emj.14.3.165. PMID: 9193982
Roberts AH, Roberts FE, Hall RI, Thomas IH. A prospective trial of prophylactic povidone iodine in lacerations of the hand. J Hand Surg Br. 1985 Oct;10(3):370-4. doi: 10.1016/s0266-7681(85)80064-4. PMID: 3908603
Saeg F, Schoenbrunner AR, Janis JE. Evidence-Based Wound Irrigation: Separating Fact from Fiction. Plast Reconstr Surg. 2021 Oct 1;148(4):601e-614e. doi: 10.1097/PRS.0000000000008331. PMID: 34415884
Singer AJ, Hollander JE, Subramanian S, Malhotra AK, Villez PA. Pressure dynamics of various irrigation techniques commonly used in the emergency department. Ann Emerg Med. 1994 Jul;24(1):36-40. doi: 10.1016/s0196-0644(94)70159-8. PMID: 8010547
Soeselo DA, Yolanda R, Zita M, Theresia S, Astiarani Y, Santi BT. Antiseptic versus non-antiseptic solutions for preventing infection in acute traumatic wounds: a systematic review. J Wound Care. 2022 Feb 2;31(2):162-169. doi: 10.12968/jowc.2022.31.2.162. PMID: 35148627
Weiss EA, Oldham G, Lin M, Foster T, Quinn JV. Water is a safe and effective alternative to sterile normal saline for wound irrigation prior to suturing: a prospective, double-blind, randomised, controlled clinical trial. BMJ Open. 2013 Jan 16;3(1):e001504. doi: 10.1136/bmjopen-2012-001504. PMID: 23325896
Wheeler CB, Rodeheaver GT, Thacker JG, Edgerton MT, Edilich RF. Side-effects of high pressure irrigation. Surg Gynecol Obstet. 1976 Nov;143(5):775-8. PMID: 982257
Wound Healing and Management Node Group. Evidence summary: Wound management – Chlorhexidine. Wound Practice and Research. 25(1). Available at: https://journals.cambridgemedia.com.au/wpr/volume-25-number-1/evidence-summary-wound-management-chlorhexidine



2 thoughts on “How should we irrigate lacerations? Does it even matter?”