
Morgenstern, J. Research Roundup October 2022, First10EM, October 31, 2022. Available at:
https://doi.org/10.51684/FIRS.128733
A true rarity: An RCT demonstrating a mortality benefit, but is it too good to be true?
Matchett G, Gasanova I, Riccio CA, Nasir D, Sunna MC, Bravenec BJ, Azizad O, Farrell B, Minhajuddin A, Stewart JW, Liang LW, Moon TS, Fox PE, Ebeling CG, Smith MN, Trousdale D, Ogunnaike BO; EvK Clinical Trial Collaborators. Etomidate versus ketamine for emergency endotracheal intubation: a randomized clinical trial. Intensive Care Med. 2022 Jan;48(1):78-91. doi: 10.1007/s00134-021-06577-x. Epub 2021 Dec 14. PMID: 34904190
This RCT demonstrates a mortality benefit of ketamine over etomidate when used as an induction agency in emergency intubations in select ICU patients. However, there are many issues with the study which limit confidence in the results. It is a single center unblinded trial which uses a convenience sample (the airway team were encouraged to enroll patients, but were under no obligation to.) This hospital uses a special airway team led by anesthesiology for all emergency intubations in the ICU, which won’t translate well into most other practice settings. When patients were enrolled, they were randomized to either etomidate (0.3-0.3 mg/kg IV) or ketamine (1-2 mg/kg IV). The primary outcome was mortality at 7 days, and the headline news is that 77% of the etomidate group was alive as compared to 85% of the ketamine group (HR 1.6, 95% CI 1.2-2.2). By day 28, survival between the groups was closer and no longer statistically significant (64.1% vs 66.8%), but the difference would be clinically important. There were a number of other differences which are hard to explain in the trial, such as the fact that the ketamine group actually had a significantly higher rate of post-induction hemo-dynamic collapse. As I almost never use etomidate, this trial can’t really change my practice. Even if you are an avid user of etomidate, I am not sure this trial should change your practice, given that it is an unblinded, single center trial with many sources of bias. However, a large mortality difference in an RCT is definitely something to pay attention to, and certainly warrants follow-up blinded research.
Not surprisingly, this paper has been covered by basically everyone who talks about research, so if you want to hear some other opinions, check out the SGEM, REBEL EM, or St. Emlyn’s.
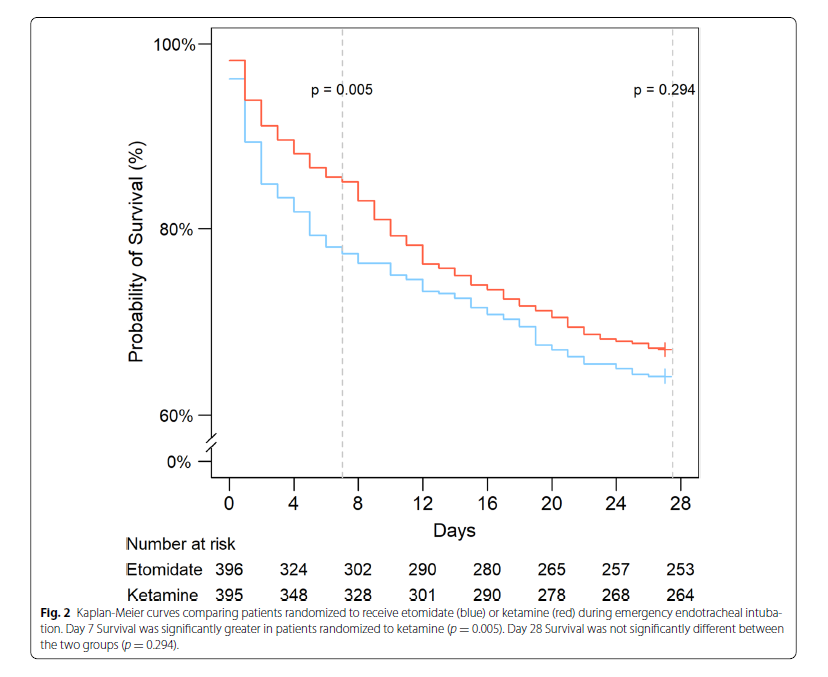
Bottom line: Although this RCT demonstrates a 7 day mortality benefit of using ketamine over etomidate, the level of certainty in the results is low.
The PEACH trial: Not such a peach
Peter-Derex L, Philippeau F, Garnier P, et al. Safety and efficacy of prophylactic levetiracetam for prevention of epileptic seizures in the acute phase of intracerebral haemorrhage (PEACH): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Neurol. 2022 Sep;21(9):781-791. doi: 10.1016/S1474-4422(22)00235-6. PMID: 35963261
This is a double blind trial comparing levetiracetam to placebo in patients with non-traumatic intracerebral hemorrhage. To date, the evidence for seizure prophylaxis has generally been negative, so there is some excitement for this positive trial, but I think we need to severely temper that excitement. This trial only includes a total of 50 patients (42 in their primary analysis), when it was supposed to include 102. You might hear the headline, which is that there was a statistical decrease in seizures from 43% to 16% with levetiracetam. However, that headline is completely misleading. This paper shouldn’t change anything about the way you manage these patients. I am sympathetic to trials stopped because of COVID, but this trial was stopped early without specific criteria, which is problematic. Perhaps because of that, there are significant baseline differences between the groups, such as the placebo group having larger hematomas and worse stroke scores. Most importantly, there was no difference in seizures – at least seizures you would recognize. At 72 hours, there were exactly 0 seizures in both groups. It was only EEG changes that differed between the groups, but we have no idea if those EEG changes are a marker of long term outcomes (even clinical seizures might not be). I also question the trustworthiness of the data, as the primary outcome reported in the manuscript does not match the primary outcome in the clinicaltrials.gov protocol.
Bottom line: You might hear about this trial, but this is definitely not practice changing evidence. It needs follow-up with bigger trials looking at clinically important outcomes.
Breaking good news: an essential skill for avoiding too much medicine?
Danczak A. Breaking good news: an essential skill for avoiding too much medicine? BMJ. 2018 Sep 11;362:k3843. doi: 10.1136/bmj.k3843. PMID: 30206143
This is a great essay, and it is worth reading in its entirety. In medicine, many of us develop the habit of framing good news as bad, and even if we don’t, our patients often hear it that way. “Negative” test results mean that we found no pathology, which is good news. However, this good news leaves uncertainty, and is often interpreted as a significant remaining possibility of illness; that the doctor just hasn’t found the problem yet. Medical education fosters this attitude. Diagnosis is taught as if there is always a disease to be found, but experienced doctors know this is rarely the case. This author argues that we need better training in “breaking good news”. The language we use matters a lot. Truly positive phrases, such as “you chest sounds healthy”, and interpreted better than negative or uncertain ones, such as “I don’t hear anything wrong”. It is also important to be explicit about the value of the tests we order before we order them. Is this test meant to rule in or rule out? (I have made this mistake many times, by not explaining the value of a Ddimer test, and having a patient panic when it comes back positive. This is even worse in an era where patients can access their test results online before they are explained by the physician.)
Bottom line: I think that the impacts of our language on our patients is an area that needs a lot more attention. This paper doesn’t give us definitive answers, but does provide a lot of food for thought.
Less is more when it comes to intravenous fluids
de-Madaria E, Buxbaum JL, Maisonneuve P, et al. Aggressive or Moderate Fluid Resuscitation in Acute Pancreatitis. N Engl J Med. 2022 Sep 15;387(11):989-1000. doi: 10.1056/NEJMoa2202884. PMID: 36103415
The last decade has served a relatively steady stream of data suggesting that we use way too much IV fluids with almost all of our patients. This most recent RCT – the WATERFALL study – looked at adult patients with mild to moderate acute pancreatitis, and randomized them to either ‘aggressive’ or ‘moderate’ fluid resuscitation. The aggressive group received a 20 mL/kg bolus followed by 3 mL/kg/hour. The moderate group received a 10 mL/kg bolus and 1.5 mL/kg/hour. They used Ringer’s lactate in both groups. The trial was stopped early, after enrolling 249 patients, because an interim analysis suggested harm in the form of increased fluid overload in the aggressive group. Their primary outcome was the development of severe pancreatitis, and occurred in 22% of the aggressive group and 17% of the moderate group (aRR 1.30, 95%CI 0.78-2.18). Fluid overload occurred in 20% of the aggressive group, as compared to 6% of the moderate group (aRR 2.85, 95%CI 1.36-5.94). Of course, fluid overload is a surrogate outcome, but important outcomes also look worse with the aggressive approach. For example, respiratory failure was 7% vs 2%, but not statistically significant. This is an open-label trial, which significantly limits certainty, but it fits with all of the other literature I have seen on intravenous fluids.
Bottom line: Less is more when it comes to intravenous fluids.
Is there any wonder why we have all lost faith in infection control practitioners?
Joshi A, Jiang Y, Jones P. Does wearing a surgical mask influence face touching by healthcare workers? A retrospective cohort study. Emerg Med Australas. 2022 Sep 18. doi: 10.1111/1742-6723.14082. Epub ahead of print. PMID: 36117397
In one of the dumber phases of the COVID pandemic, some infection control practitioners told us not to wear masks ‘because they would make us less safe by making us want to touch our faces more often’. (It feels like people probably shouldn’t just be pulling recommendations out of their ass when faced with a global pandemic, but I guess that is a rant for another day.) This is an interesting retrospective study in which they reviewed emergency department security camera footage to determine the rate at which masked healthcare professionals touch their face. In total, there were 99 nurses, 50 doctors, and 38 other staff observed. Masks were not universally worn during the study period, with 37% of the doctors, 24% of the nurses, and 58% of the other staff wearing masks in the observed footage. The data suggests that prior estimates of face touching are over blown, as the median number of face touches per session was 0, for a median of 0 seconds. There were some outliers, with a maximum of 29 touches, and my favourite: someone who managed to touch their face for 536 seconds. I am picturing someone deep in thought stroking their beard for 9 straight minutes? The results were not statistically significant, but face touching was actually lower with masks, OR 0.55, 95% CI 0.3-1.01, p=0.055). The chance of a healthcare worker touching their mucosa was statistically lower when wearing a mask. This data is from New Zealand in 2020 and early 2021, when COVID was essentially unheard of in the country. That explains the low overall mask usage, but probably doesn’t really affect the primary question. If anything, I would guess that if you were actually seeing sick patients, you would be more focused on not touching your face, so this data is likely an overestimate.
Bottom line: This study probably shouldn’t have been required, because it was a really stupid argument to begin with, but at least we can put this part to rest: masks aren’t going to make you touch your face more, and if anything, they prevent you from touching the important areas, because they are covered. In future pandemics, we should require infection control practitioners to base their recommendations on science.
Tips for radial artery art lines
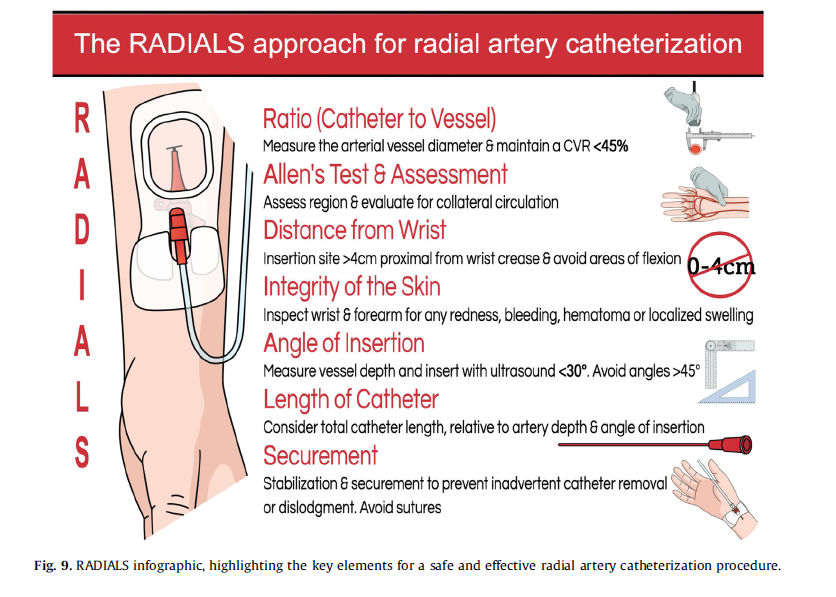
Imbrìaco G, Monesi A, Spencer TR. Preventing radial arterial catheter failure in critical care – Factoring updated clinical strategies and techniques. Anaesth Crit Care Pain Med. 2022 Aug;41(4):101096. doi: 10.1016/j.accpm.2022.101096. Epub 2022 Apr 28. PMID: 35490863
Despite being ubiquitous in critical care, I think arterial lines might be the most under-utelized piece of equipment in emergency medicine. My guess is that we avoid them because they can be technically difficult, time consuming, and a history of failures weighs in the back of many of our minds (perhaps because many of us trained prior to the introduction of routine ultrasound). This paper is a nice review of techniques to optimize radial arterial line placement. It is worth a reading in full, but my quick take-away are:
- Ultrasound is clearly the way to go, with less overall failure, more first-attempt successes, and fewer pokes.
- One less discussed benefit of the ultrasound is the ability to move more proximally, away from the wrist crease, decreasing mechanical complications later as the patient moves their hand.
- The more of the catheter you can get in the vessel, the more likely the line is to succeed over the long run. Understanding a little math here helps. If the artery is 1cm deep to the skin and you approach at a 45 degree angle – 1.4cm of the catheter will be in the skin and soft tissues; if you approach at a 30 degree angle 2 cm will be in the soft tissues. Ultrasound can help visualize this, and the use of longer catheters is recommended.
- Despite resulting in more catheter in the vessel, steeper angles of attack are associated with higher failure rates. Avoid angles greater than 45 degrees.
- Bevel-down results in higher success with fewer back-wall punctures.
- Use local anesthetic. A median nerve block might help, and might actually cause radial artery vasodilation.
- We don’t see it in the ED, but a large number of these devices get yanked out at some point during the ICU stay. It is important to secure them well.
- Stay away from the wrist. A radial artery within 2cm of the wrist fold is associated with an increased risk of complications.
Hands on defibrillation: Even if it’s safe, would it actually help?
Stephens AF, Šeman M, Nehme Z, Voskoboinik A, Smith K, Gregory SD, Stub D. Ex vivo evaluation of personal protective equipment in hands-on defibrillation. Resusc Plus. 2022 Aug 3;11:100284. doi: 10.1016/j.resplu.2022.100284. PMID: 35942482
Given the importance of limiting pauses in chest compressions, there has been interest (from some people) in performing hands on defibrillation. This study mostly gets included because self-experimentation (the authors put themselves at risk) is interesting. The study itself uses a pig model, and looks at 3 different scenarios: 1) adding pressure to the pads only, with a closed fist, as one might if trying to improve contact for cardioversion; 2) adding pressure over the pads, but with fingers on the skin, as if one made a mistake in scenario #1; 3) hands in the middle of the chest, on skin, as if doing chest compressions. In each setup, they tested multiple PPE options (different types of gloves, double gloving, etc.). There are lots of numbers in the paper. Shocking while doing chest compressions without gloves seems like a bad idea, as the measured current was potentially high enough to induce cardiac arrest. However, my best summary of all the numbers is that as long as you are wearing gloves, you won’t be exposed to 2 mA of current, and therefore would be well below the level of danger (but you might feel something). Whether all this effort is worth it is another question altogether. The papers I have seen on the topic have all focused on safety. Personally, I have some questions about efficacy. Chest compressions dramatically impact the anatomy of the chest, and often cause contact issues with pads, which seems like it could impact the vector and efficacy of defibrillation. I think we need to be questioning the efficacy of this approach, and not just its safety. If you need to stop compressions anyway to ensure efficacy, why not just raise your hands briefly off the chest? More than that, to ensure good compressions, we need to be swapping out compressors every 2 minutes, and defibrillation is a natural stop point. Why introduce another unnecessary pause? Personally, my guess is that latex gloves will be enough to keep us safe, but that the whole concept may be flawed and unnecessary. On the other hand, ‘manual compression augmentation’, when pressure is applied over the pads to ensure good contact and decrease impedance makes some sense to me. However, we already have a device specifically designed for this task – traditional paddles. If you need to improve contact, why not use the paddles, rather than your hands?
Bottom line: This data suggests that as long you are wearing gloves, hands on defibrillation is probably safe. However, I think we need to question its overall value before adopting such a practice.
Suturing doesn’t need sterile gloves
Zwaans JJM, Raven W, Rosendaal AV, Van Lieshout EMM, Van Woerden G, Patka P, Haagsma JA, Rood PPM. Non-sterile gloves and dressing versus sterile gloves, dressings and drapes for suturing of traumatic wounds in the emergency department: a non-inferiority multicentre randomised controlled trial. Emerg Med J. 2022 Jul 26:emermed-2021-211540. doi: 10.1136/emermed-2021-211540. Epub ahead of print. PMID: 35882525
I think most people already believe this, but this is actually only the second RCT comparing clean to sterile gloves for suturing in the ED. It is a very large mutli-centre non-inferiority RCT was published in the Emergency Medicine Journal. They included 1480 (of 2468 eligible) adult patients with lacerations requiring sutures in an emergency department, and randomized them to either have their wound closed by a doctor wearing sterile gloves or non-sterile gloves. All wounds were irrigated with tap water (which has been studied elsewhere, but if you are a believer in sterile gloves you might also be a believer in sterile irrigation). The primary outcome was wound infection, and was assessed by a physician blinded to the allocation group of the patient between 5 and 15 days later. They set a non-inferiority margin of 2% – meaning that they were OK with 2% more infections in the non-sterile group – but I am not sure this is a clinically appropriate margin. (This is always a problem with non-inferiority trials.) Unfortunately, the study was supposed to include 2140 patients, but they stopped early because apparently they weren’t seeing lacerations in the ED anymore (something about merging the ED with local GP offices). Mostly, the patients were young males without commorbidities (so low risk for wound infection). The wound infection rate in the sterile treatment group was 6.8% (95% CI 4.0% to 7.5%) vs 5.7% (95% CI 5.1% to 8.8%) in the non-sterile treatment group. The mean difference of the wound infection rate of the two groups was −1.1% (95% CI −3.7% to 1.5%). Despite being stopped early, this is the best evidence available on the topic, and is most consistent with no difference between using sterile gloves and not. It cannot completely exclude a small decrease in infections, but given the added costs and complexities of sterile laceration repair, I think non-sterile gloves are the way to go for almost all patients. Clinical judgment always applies though, and it might be reasonable to use sterile gloves in patients with much higher risk of infection. Keep your eyes out for a full review on this topic, as part of a very lengthy review of the evidence for wound care coming this fall.
Bottom line: Gloves from that box on the wall are good enough for suture repair.
More evidence against hypothermia
Wolfrum S, Roedl K, Hanebutte A, Pfeifer R, Kurowski V, Riessen R, Daubmann A, Braune S, Söffker G, Bibiza-Freiwald E, Wegscheider K, Schunkert H, Thiele H, Kluge S. Temperature Control After In-Hospital Cardiac Arrest: A Randomized Clinical Trial. Circulation. 2022 Sep 28:101161CIRCULATIONAHA122060106. doi: 10.1161/CIRCULATIONAHA.122.060106. Epub ahead of print. PMID: 36168956
This is big RCT, but with many problems. It is an RCT comparing post-arrest hypothermia (32-34 degrees) to normothermia in inpatient cardiac arrest. This is really important, as most prior trials have focused on outpatient cardiac arrest, where outcomes are generally dismal to begin with. It is really hard to demonstrate a benefit from therapy if 98% of the patients you enroll die in both groups. Therefore, this inpatient data, where outcomes are much better, is really important. Unfortunately, this trial has many problems. More than a quarter of the patients in the hypothermia group didn’t hit their target temperatures by 12 hours. More importantly, it was stopped early without any prespecified criteria. This is especially problematic, because they powered the trial based on the completely unrealistic thought that they would see a 16% absolute decrease in all cause mortality. That is just an unheard of benefit, and it means that we are left with a trial that is woefully under-powered. That being said, there isn’t even a hint of benefit, with 72% of both groups dying, and neurologic outcomes also being identical.
Bottom line: Despite the significant imperfections of this trial, it is important data (as we lack data on hypothermia after inpatient cardiac arrest), and it adds to the growing body of evidence that suggests hypothermia provides no benefit.
Good news for medical school applicants: A sub-60 IQ is not an disqualifying feature
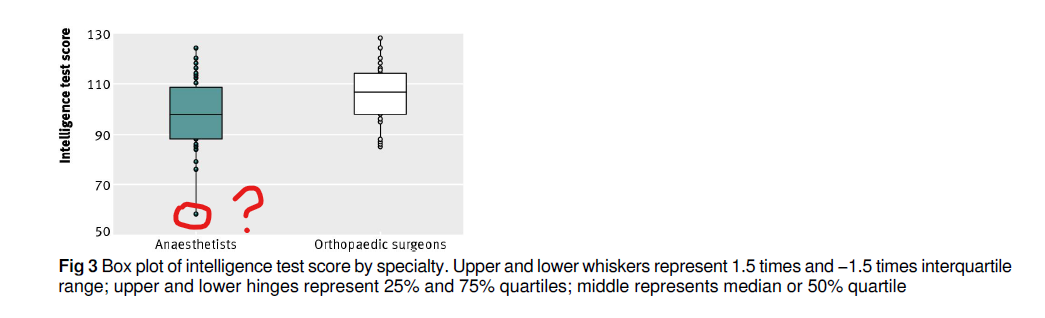
Subramanian P, Kantharuban S, Subramanian V, Willis-Owen SA, Willis-Owen CA. Orthopaedic surgeons: as strong as an ox and almost twice as clever? Multicentre prospective comparative study. BMJ. 2011 Dec 15;343:d7506. doi: 10.1136/bmj.d7506. PMID: 22174322
This feels like a paper I should have covered before, but I don’t see it anywhere in my database. Apparently there is a popular saying in British hospitals: “typical orthopaedic surgeon—as strong as an ox but half as bright.” This study aimed to test that aphorism. They include 36 orthopedic surgeons, and compare them to 46 anesthetists. Unfortunately, all orthopedic surgeons were male (and only 6 of the 46 anesthetists were female, which is a troublesome mix for this hospital.) Because grip strength in correlated with biologic sex, they decided to eliminate the females from the study, but that introduces significant selection bias, as they might have eliminated the 6 smartest anesthetists. Perhaps unsurprisingly, considering that the study was done by surgeons, they determined that orthopedic surgeons were statistically smarter and stronger. IQ was 105 in the surgeon group and 98 in the anesthetists group, which considering that 100 is exactly average for all humans, seems surprisingly low (especially considering what doctors usually think of themselves). I am particularly concerned about 1 outlier in the anesthetist group. I really hope the sub-60 IQ was just a result of a night shift, because otherwise I might have some concerns. I have no baseline to know how impressive their grip strength was, but it was 47 kg versus 43, which may or may not be clinically relevant. I was very disappointed by the lack of an ox control group, which given the aphorism they set out to test, sort of undermines the validity of the entire trial.
Cheesy Joke of the month
I used to tell dad jokes
He’s dead now though




6 thoughts on “Research Roundup October 2022”