I started writing this review of dog bite management a long time ago, but I abandoned it because I thought the word was already out. I thought this had been settled; that everyone knew these myths. However, a few recent conversations have highlighted the fact that the management of dog bites is still steeped in controversy with wide practice variations. Therefore, we will dust off some old papers and see what EBM has to say (and it might be a little more complicated than I remembered)…
Part 1: Do dog bites need prophylactic antibiotics?
This is always the big question. Dogs mouths are filthy. The have special bacteria that you have to memorize for board exams (but otherwise are probably meaningless). With all that bacteria, we have to give antibiotics, right? That is certainly how I was taught, but it isn’t clear that that approach is helping our patients.
Medeiros I, Saconato H. Antibiotic prophylaxis for mammalian bites. The Cochrane database of systematic reviews. 2001. PMID: 11406003
This Cochrane review identified 8 RCTs looking at antibiotic prophylaxis after mammalian bites. Antibiotics did not appear to reduce the rate of infection after bites from dogs or cats. (They did reduce the rate of infection after human bites). Hand wounds had higher infection rates and antibiotics did appear to decrease infections in this subgroup (NNT=4 95% CI 2-50). Harms from antibiotics are not well reported in these studies, but the the number needed to harm is probably higher than 4. However, prevention of infection is a very questionable patient oriented outcome. Essentially we are arguing that we should give everyone antibiotics to prevent a few from having to take them later. I am not sure that makes any sense. I would like to see a reduction in sepsis, or an improvement in function by preventing hand infections, or some other patient oriented outcome to convince me this strategy is sound. Bottom line: Based on this Cochrane review, there doesn’t seem to be a role for routine antibiotics. There may be a role for use in hand wounds.
That seems pretty easy. The Cochrane review is negative. The studies aren’t great, but based on what is reported, we probably shouldn’t be using prophylactic antibiotics routinely. However, there is another meta-analysis that is widely cited:
Cummings P. Antibiotics to prevent infection in patients with dog bite wounds: a meta-analysis of randomized trials. Annals of emergency medicine. 23(3):535-40. 1994. PMID: 8135429
This is an older meta-analysis. It also included 8 RCTs, but it comes to the opposite conclusion on the Cochrane review: antibiotics help. Infection in the control group was 16% (somewhat high as compared to the other studies here). Antibiotics decreased infection with a relative risk of 0.56 (95% CI 0.38-0.82).
So why do these 2 meta-analyses come to different conclusions? The Cochrane review included 2 studies not in the Cummings paper. Elenbass (1984) looked only at cat bites, and concluded that antibiotics were helpful. Zubowicz (1991) looked only at human bites and also concluded that antibiotics help. Therefore, these 2 studies can’t explain the discrepancy between the two meta-analyses.
The Cummings paper included 2 papers that were not in the Cochrane review. Callaham (1980) was excluded from the Cochrane review because it was not a randomized trial. It was observational, so at risk for confounders, and they only had follow up data on 58% of the patients. There was no statistical difference between the groups and only 11 total infections, so it can’t explain the discrepancy either. (Callaham 1980)
The other paper included in the Cummings paper is:
Brakenbury PH, Muwanga C. A comparative double blind study of amoxycillin/clavulanate vs placebo in the prevention of infection after animal bites. Archives of emergency medicine. 6(4):251-6. 1989. PMID: 2692580 [free full text]
This is a double blind randomized controlled trial. 185 patients 6 years and older with full thickness animal bites were randomized to either amoxicillin/clavulanate or placebo. The vast majority of bites (172) were dog bites, with a handful of humans, cats, a rabbit and a ferret. Follow up was 77% at day 3. Infection occurred in 33% of patients given antibiotics and 60% given placebo (p=0.009). This is an incredibly high infection rate; much higher than all the other studies, and certainly does not represent the patients I am used to seeing. I think this study uses a very funny definition of wound infection, which would explain why it is such an outlier. “Infection was defined as the presence of erythema and tenderness beyond that expected 24 h after the injury with or without purulent discharge, cellulitis or lymphangitis”. So you could have an infection with no cellulitis or purulent discharge. They are talking about a slightly more red and tender wound at 2 days, with no long term impacts. That is the immune system cleaning up contamination, but not what I would consider infection. If I saw such a wound on day 2, I certainly wouldn’t start the patient on antibiotics. This very loose definition explains the crazy 60% infection rate, but also trivializes the benefit of antibiotics. Of note, antibiotics didn’t help in children (24% with antibiotics and 20% with placebo) and antibiotics also weren’t helpful if the patient presented in less than 9 hours.
As you can see from the forest plot in the Cummings meta-analysis, this Brakenbury study is the only statistically significant result, and drives the conclusion of the meta-analysis:
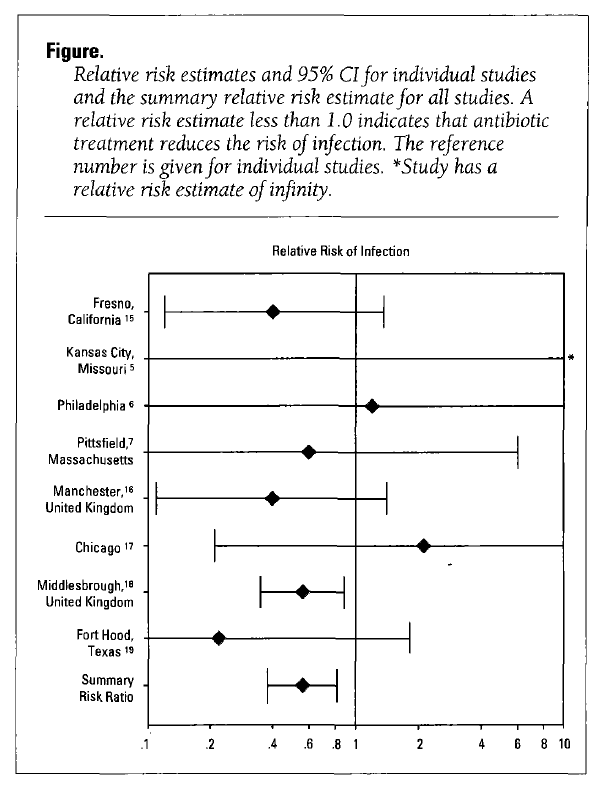
This single trial is the only real difference between the two meta-analyses. Therefore, which meta-analysis you believe will depend a lot on what you think about this one paper. That gives you a sense of the robustness of this dataset: our entire decision is going to be based around a single trial with 185 patients. Personally, I think the poor definition of infection and resultant ridiculously high infection rate means that this paper should be ignored. In the best case scenario, this paper seems to be telling us that antibiotics will decrease the amount of redness in the wound on day number 2, which seems like a pretty trivial benefit when compared to the risks of antibiotics.
There is one more paper published since this review:
Quinn JV, McDermott D, Rossi J, Stein J, Kramer N. Randomized controlled trial of prophylactic antibiotics for dog bites with refined cost model. West J Emerg Med, Dec 2010. 11(5):435-41. PMID: 21293762 [free full text]
This is an RCT looking at 95 immunocompetent patients (out of 230 screened) presenting within 12 hours of a dog bite. Infection occurred in 2 of 44 patients (4%) in the control group and 0 of 46 patients treated with antibiotics. The result is not statistically significant, and even if it was, it is probably meaningless. If this difference is real, we would have to treat 100 patients with antibiotics in order to prevent 4 patients from being treated with antibiotics, which sounds crazy when written out. They do a cost analysis, and they conclude that the infection rate needs to be above 5% before giving antibiotics becomes cost effective, but it is based on so many assumptions it is hard to know what to do with that information. More importantly, if we aren’t helping our patients, what does the cost analysis matter?
Overall bottom line
This data is clearly imperfect. These are small numbers and low quality trials, so I expect some people will disagree with me. Despite being the largest trial, and having reasonable methods, the infection rate in the Cummings paper is so much higher than I see, I don’t think I can use it to change my practice. Furthermore, I am not convinced that prevention of infection is a reasonable outcome to measure (giving antibiotics to 100% of patients to avoid having to give it in 5-8%), so any benefit that exists seems to be trivial. The harms of overusing antibiotics, however, are not trivial. Small RCTs like these always underestimate harms. It does not take many patients with antibiotic associated diarrhea or allergies to outweigh any possible benefit described here. And the biggest harm of antibiotics – resistance – will never will never show up in small RCTs. Resistance is incredibly difficult to quantify in a single study, but it is clearly important, so we need to consider it in our calculations even if it is hard to assign a specific number to the risk.
For now, I follow the Cochrane review and do not routinely provide prophylactic antibiotics, but this area is ripe for one large, high quality RCT. That being said, I practice evidence based medicine, of which clinical expertise and patient preference are essential components. I talk to all my patients and in those at a very high risk of infection (especially prolonged or complicated infection) I will offer antibiotics.
Part 2: Can I suture a dog bite?
The other big question that comes up when managing a dog bite is: should I suture this?
Maimaris C, Quinton DN. Dog-bite lacerations: a controlled trial of primary wound closure. Archives of emergency medicine. 5(3):156-61. 1988. PMID: 3178974 [free full text]
A randomized controlled trial comparing primary closure to leaving the wound open in 169 lacerations (in 96 patients) caused by dog bites. Obviously they were unable to blind this trial. Prophylactic antibiotics were not given. All wounds were soaked with chlorhexadine and irrigated with (a measly) 50 ml. The overall infection rate was 7.7%, and was the same in both groups (7/92 sutured and 6/77 open). Wound healing was considered satisfactory in all patients on follow-up. (The scar was an average of 1mm narrower in the sutured group). Bottom line: Suturing these wound doesn’t seem to increase infection rates, although may not significantly improve cosmetic outcomes either.
Chen E, Hornig S, Shepherd SM, Hollander JE. Primary closure of mammalian bites. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 7(2):157-61. 2000. PMID: 10691074 [free full text]
This is a prospective observational cohort of 145 mammalian bites (88 dog, 45 cat and 12 human) all treated with primary suture closure at the discretion of the treating physician. We don’t know how many mammalian bites were treated without closure, and therefore the degree of selection bias. There were 8 infections (5.5%; 95% CI 1.8% to 9.2%), 4 of the upper extremity and 4 of the head. All of these patients had been given prophylactic antibiotics. There is no comparison group, so this is purely descriptive. Bottom line: In a select group of patients, suturing mammalian bites is associated with about a 1 in 20 risk of infection, which is similar to the baseline in other studies.
Wu PS, Beres A, Tashjian DB, Moriarty KP. Primary repair of facial dog bite injuries in children. Pediatric emergency care. 27(9):801-3. 2011. PMID: 21878832
A retrospective chart review looking at 87 pediatric patients with dog bites to the face. There were no infections. However, more than ½ of these patients were repaired in the OR, so these are not necessarily your standard ED dog bites. 7/40 ED patients and 22/22 OR patients were closed with sutures. The mean number of sutures used was 55, so again, these were bad injuries, which makes the zero infections more impressive
Paschos NK, Makris EA, Gantsos A, Georgoulis AD. Primary closure versus non-closure of dog bite wounds. A randomised controlled trial. Injury. 2014; 45(1):237-240. PMID: 23916901
This study is an RCT that included 168 dog bites and randomized them to either suturing or not. All patients received prophylactic antibiotics. Inclusion criteria included full thickness wounds presenting within 48 hours in patients over 15 years of age. They excluded complex or complicated wounds and patients with immunosuppression. As a result, out of a consecutive sample of 227, they only excluded 18 (and another 25 refused to participate).
There was no difference in infection between the two groups (9.7% vs 6.9%, p = 0.51,odds ratio 1.44, 95% CI 0.48–4.35). Cosmetic appearance at 4 weeks using the Vancouver Scar Scale by a blinded surgeon was significantly better in the sutured group. The big determinant of infection was whether patients presented before or after 8 hours, but suturing didn’t change things in either group.
Overall Bottom Line
All the studies seem to support primary closure, although there are some significant limitations. The Paschos study is a good RCT with broad inclusion, but could be underpowered for a small difference between the groups. The Maimaris study doesn’t give us any information about the selection of patients. None of the trials could be blinded. However, I think that the current best answer is that it is safe to close the vast majority of these wounds. I am more cautious in immunocompromised patients, not because there is any evidence that it is worse, but because there is no evidence, and when the inevitable infection occurs, someone is bound to complain. (I think shared decision making is sufficient). With very large, complicated wounds, I think it is reasonable to involve a surgeon (who will inevitably close them, but perhaps after a much better clean out in the OR.)
Unfortunately, now that I live in New Zealand, I need a different question answered. How do I manage patients bitten by animals in the ocean? I guess I had better get back to PubMed…
Other FOAMed
The NNT: Antibiotics for Prophylaxis of Animal Bites
REBEL EM: Medical Myths in the Management of Dog Bites
References
Brakenbury PH, Muwanga C. A comparative double blind study of amoxycillin/clavulanate vs placebo in the prevention of infection after animal bites. Archives of emergency medicine. 6(4):251-6. 1989. PMID: 2692580 [free full text]
Callaham M. Prophylactic antibiotics in common dog bite wounds: a controlled study. Annals of emergency medicine. 1980; 9(8):410-4. [pubmed]
Chen E, Hornig S, Shepherd SM, Hollander JE. Primary closure of mammalian bites. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 7(2):157-61. 2000. PMID: 10691074 [free full text]
Cummings P. Antibiotics to prevent infection in patients with dog bite wounds: a meta-analysis of randomized trials. Annals of emergency medicine. 23(3):535-40. 1994. PMID: 8135429
Cummings P, Del Beccaro MA. Antibiotics to prevent infection of simple wounds: A meta-analysis of randomized studies The American Journal of Emergency Medicine. 1995; 13(4):396-400.
Elenbaas RM, McNabney WK, Robinson WA. Evaluation of prophylactic oxacillin in
cat bite wounds. Ann Emerg Med. 1984 Mar;13(3):155-7. PubMed PMID: 6696302
Maimaris C, Quinton DN. Dog-bite lacerations: a controlled trial of primary wound closure. Archives of emergency medicine. 5(3):156-61. 1988. PMID: 3178974 [free full text]
Medeiros I, Saconato H. Antibiotic prophylaxis for mammalian bites. The Cochrane database of systematic reviews. 2001. PMID: 11406003
Wu PS, Beres A, Tashjian DB, Moriarty KP. Primary repair of facial dog bite injuries in children. Pediatric emergency care. 27(9):801-3. 2011. PMID: 21878832
Zubowicz VN, Gravier M. Management of early human bites of the hand: a
prospective randomized study. Plast Reconstr Surg. 1991 Jul;88(1):111-4.
PMID: 2052637
Morgenstern, J. Dog Bite Management: The Evidence, First10EM, January 28, 2019. Available at:
https://doi.org/10.51684/FIRS.7401



7 thoughts on “Dog Bite Management: The Evidence”
Excellent review! A lot of myths we have are explained in this post , so thanks for that.
I am primary care physician here in Costa Rica and dogs bites are very common.the use of antibiotics are almost like a “ cuisine recipe” here . The physicians sometimes we can’t take away the idea for the patients with low infection risk don’t need profilaxis antiobiotics.
Thank for this post again