
Morgenstern, J. Dose VF: A double sequential defibrillation game changer?, First10EM, November 8, 2022. Available at:
https://doi.org/10.51684/FIRS.128926
I can almost guarantee that everyone has heard about this paper already. It is an exciting topic. It is resuscitation and gadgets. It is emergency medicine in the New England Journal (which is great, despite how atrocious this journal often is.) So does double sequential defibrillation help? Let’s look at the Dose VF study.
I covered the publication of the pilot study here. As I mentioned in that article, I have a slight conflict of interest. I know the authors of this study personally, and I think they are tremendous people. I don’t think that will impact anything I say. If anything, I may need to apologize to Sheldon if my appraisal comes across as too harsh.
The paper
DOSE VF: Cheskes S, Verbeek PR, Drennan IR, McLeod SL, Turner L, Pinto R, Feldman M, Davis M, Vaillancourt C, Morrison LJ, Dorian P, Scales DC. Defibrillation Strategies for Refractory Ventricular Fibrillation. N Engl J Med. 2022 Nov 6. doi: 10.1056/NEJMoa2207304. Epub ahead of print. PMID: 36342151 NCT04080986
The Methods
DOSE VF is a cluster-randomized, open-label, three group, cross-over trial from six paramedic services in Ontario, Canada.
Patients
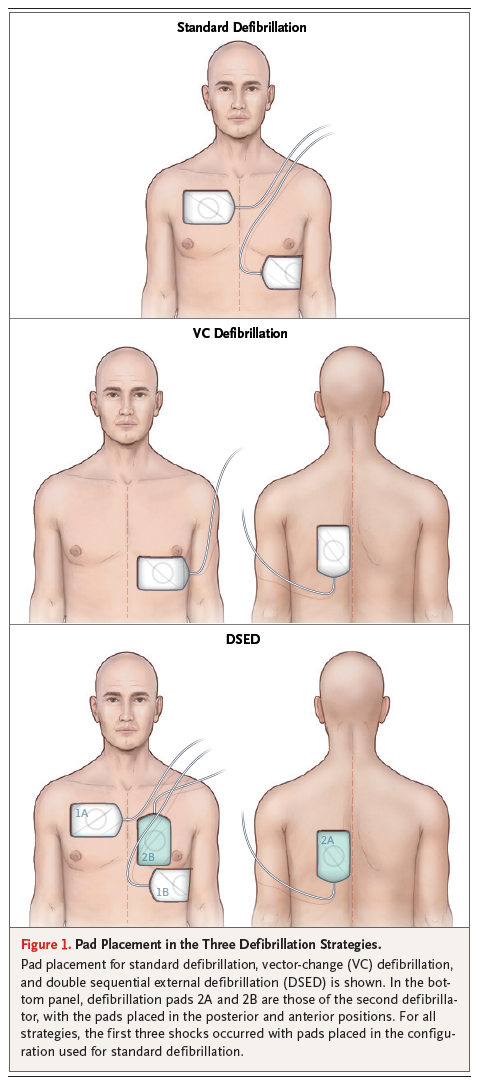
Adult patients with out-of-hospital cardiac arrest with a presumed cardiac cause and refractory ventricular fibrillation (meaning the original rhythm was either v.fib or pulseless v.tach and at least 3 attempts at defibrillation had been unsuccessful). Initial defibrillation was all done through pads placed in the standard anterior-lateral position.
Exclusions: Traumatic cardiac arrest, DNR orders, drowning, hypothermia, hangings, and suspected drug overdose.
Intervention
- Double sequential defibrillation: a second set of pads were applied in the anterior-posterior position, and all shocks after the third were provided from 2 defibrillators with a 1 second delay between the two shocks (to avoid any damage to the defibrillators).
- Vector change defibrillation: pads were changed from their original anterior-lateral position to an anterior-posterior position after the third unsuccessful shock, and all subsequent shocks were done with the new AP pad position.
Comparison
All shocks continued with standard defibrillation (pads in the anterior-lateral position).
General procedures
Prehospital cardiac arrest care in Ontario is provided by paramedics. Initial care is often by primary care paramedics, whose skill set includes basic-life support including CPR and defibrillation, but not intravenous placement or advanced airway management. We also have advanced care paramedics who can start IVs, provide medications, and perform advanced airway interventions, who would be present at most cardiac arrests. We do not have prehospital physicians.
Each paramedic service had their assigned treatment group changed every 6 months.
Aside from the change in defibrillation technique, all paramedics followed our standard provincial protocol, which is essentially the AHA algorithm for the treatment of patients with ventricular fibrillation.
Outcome
The primary outcome was survival to hospital discharge.
The Results
They enrolled 405 patients. The trial was designed to include 930 patients, but it was stopped early because COVID resulted in staffing shortages that were impacting the ability to get patients enrolled in a timely fashion.
The mean age was 64 and 84% were men. 68% of arrests were witnessed, and 58% received bystander CPR.
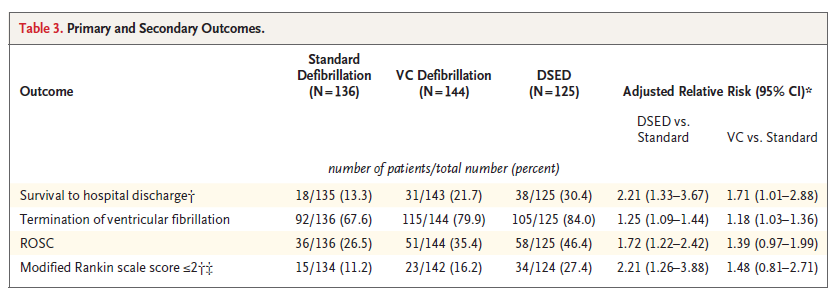
For the primary outcome of survival to hospital discharge, both treatment groups were statistically superior to standard defibrillation. Survival was 30.4% with double sequential, 21.7% with vector change, and 13.3% with standard care. Secondary outcomes also seem to favour the treatment groups, although not all were statistically significant in the vector change group.
EBM thoughts
Although DOSE VF is an important trial, and it will likely change practice, there are many limitations we need to consider.
The biggest, by far, is that this is not a blinded trial. You might not think that matters, as mortality is a pretty objective outcome. However, the termination of resuscitation in cardiac arrest is anything but objective. In Ontario, the ultimate decision lies with a physician who is not on scene (paramedics call ‘base hospital’ for a termination of resuscitation order, and the case is discussed by phone.) Both the decision to call for T.O.R, and the information provided in that phone call, can be highly variable. In the standard care group, you have already provided the exact same shock 3 times. Does it seem worth fighting for more? On the other hand, in the two treatment groups, you have just changed something, and so there is reason to be optimistic. That optimism might have a dramatic impact on the way that the resuscitation unfolds. Unfortunately, nowhere in the manuscript or supplemental material do they list the total time on scene, or total number of shocks delivered among all participants, which might give a sense of whether this bias resulted in measurable changes in on-scene treatment.
NOTE: Dr Cheskes has pointed out that that termination in the field was not allowed (although it did occur in a few patients), which limits the bias I was picturing. (This makes sense, as it would be very unusual to terminate the resuscitation of a refractory ventricular fibrillation in the field.) There are a number of ways to limit bias in unblinded trials, including using blinded outcome assessors, objective outcomes, and rigid protocols to limit practice deviation. For an unblinded study, this methodology is as good as you can get, and I agree that it would have been exceedingly difficult, if not actually impossible, to blind double sequential defibrillation. However, there are still many less overt ways in which unblinding can impact results. I have met many of the paramedics involved in this research, and I guarantee that they were more optimistic when assigned to the double sequential defibrillation groups than they were when continuing with usual care. So although these researchers did everything they could to limit the impacts of the open-label design, I still think we need to be cautious about the impact that this bias can have.
The second biggest issue with this trial is the small number of total events. It can get hidden when talking about percentages, but we are talking about 18 versus 31 versus 38 people surviving to hospital discharge. This is better than many trials I have appraised, but it is still not enough for certainty. The fragility index was 9 for double sequential (1 for vector change), which is better than a lot of medical research.
Like many other trials we have discussed over the last few years, this trial did not stop at a pre-defined endpoint, but instead because of practical issues that arose due to COVID. Changes from the original protocol always increase the risk of bias, and stopping trials early has a tendency to overestimate benefits. It is really unfortunate that these trials end up with a black eye despite all the work the researchers put in. It is even more unfortunate that the science is compromised in a way that leaves us with tremendous uncertainty.
I almost always find sample size calculations problematic. Researchers often seem to fit their calculations to the sample size they think is practical, rather than calculating the trial size needed to show a true, realistic benefit. In the pilot study, there was only a 6-14% increase in the number of patients arriving at the hospital with a pulse. (Cheskes 2020) Many fewer will survive. So the fact that this trial was powered on the assumption that they were going to see an 8% increase in survival to hospital discharge seems overly optimistic, and makes me worried the trial was under-powered from the outset. I understand that there are practical issues when designing trials like this, but this seems like an area of science that is almost always divorced from reality, and we don’t talk about it all that much.
Adherence to the trial protocol was not perfect. 31 patients who were supposed to receive vector change didn’t and had standard shocks instead. 16 patients in the double sequential group received standard shocks and 2 received vector change. One patient in the control group received double sequential. Although this is not great scientifically speaking, anyone who has ever worked in the prehospital environment will realize that it is totally understandable. Prehospital medicine is incredibly difficult. Prehospital research is next to impossible. If anything, the cross-overs seem like they would bias towards no effect.
The initial Twitter discussion of this paper seemed to contain a lot of concern for the loss of warranty when using defibrillators to provide double sequential shocks. For what it is worth, among the 125 patients treated with double sequential defibrillation, there were no reports of damage or malfunction in this trial. Obviously, this is way too small a sample size to claim it will never happen, but damage should at least be uncommon based on these numbers.
Although this shouldn’t have to be listed as a strength, considering the number of trials that we discuss that don’t follow their published protocol, it is nice to see that there were no major discrepancies from the protocol listed on clinicaltrials.gov.
Like almost all research, this trial will raise more questions than it answers. Considering the importance of rapid defibrillation, is there a role for earlier double sequence defibrillation? Should we just go to double sequential right away? Can we design our pads better? If they were bigger and covered a larger vector to begin with, would this be unnecessary? Do our defibrillators provide enough energy? Should we be able to shock at 400 joules, or even higher, off a single machine? These are all interesting questions, but should only be explored in carefully controlled research settings.
Clinical Summary
I think we need to be really cautious in our interpretation. It’s very easy to get excited. This is a result that we definitely want to be true. However, if we had any other trial that was unblinded and stopped early without a pre-specified endpoint, we would be very hesitant to trust the results. When we discuss the dose VF trial, it should always be with an appropriate degree of skepticism and uncertainty.
However, the biggest question in evidence-based clinical practice is almost always: what do we do while we wait for more science? There’s almost always remaining uncertainty. None of our trials are perfect. We are always waiting for better data, but we still have to act. So our real question is not whether double sequential defibrillation definitively works, but rather whether we should use double sequential defibrillation in a refractory ventricular fibrillation patient while we wait for confirmatory trials?
To answer that question, you have to consider the harms and costs of the intervention that you are considering in addition to your degree of certainty that there will be a benefit.
Let’s start with the certainty of benefit. This trial itself should increase certainty, but not dramatically, considering that it is unblinded and the fact that it unfortunately had to stop early. It’s very likely that this trial overestimates any real benefit. However, as compared to other therapies, I think double sequential defibrillation makes more sense. I think the pretest probability of this working is higher than most new therapies. Pharmaceuticals have to contend with complex homeostasis and many unintended biologic consequences. In refractory ventricular fibrillation, our goal is very simple. We just want to hit the reset button on the heart. If we are currently failing because our electrical dose is too low or misaligned, double sequential makes a lot of sense. If this was the only reason that defibrillation might fail, my pretest probability would be very high that double sequential would work, but in reality there are many other reasons that the initial shocks might have failed. The most common is probably that there is an ongoing coronary occlusion, and the heart isn’t going to restart no matter how many times we shock it unless we fix that underlying problem. This is not as simple as hitting the reset button on your computer, but it’s definitely not as complex as a medication. Therefore, I started with a somewhat higher pretest probability than I usually do, and this trial will increase that a small amount.
Harms and costs certainly shouldn’t be downplayed. In the emergency department, I’m not that worried about costs. We have multiple defibrillators around. It does not cost my team very much to bring a second one into the room. However, we shouldn’t downplay the costs in the prehospital environment. Are we going to put multiple defibrillators on every ambulance? If not, you are forcing multiple ambulances to go to these cardiac arrests, that is a major cost to the community and a major potential harm to other sick patients in the community.
The other harm to consider is the possibility of damaging a defibrillator. I think that is a real harm, especially if we stray from the technique used in this paper. However, when using the 1 second gap employed here, the risk is pretty damn low. And what is this harm, really, aside from an added cost? If double sequential defibrillation truly saved 17 patients out of every hundred, but we ended up frying a defibrillator every 1000 patients treated, the cost of replacement defibrillators would clearly be worth it. (This would be way less than the cost per life saved of almost all ICU therapies.) Thus, it is the uncertainty about the benefit that will really shape our decisions.
Finally, we need to consider our current practice. It has never made any sense to continue to provide the same unsuccessful therapy over and over again, so I think all of us have been changing something after 3 unsuccessful shocks, whether it was simply changing pad position, or adding a second machine.
In the emergency department, I think this is a relative no brainer. The costs and harms are relatively low, and the potential benefit is very high. Working in a community hospital without access to ECMO or the cath lab, if I have a patient in refractory ventricular fibrillation after 3 shocks, I will perform one of these techniques, but that actually isn’t a change from current practice. I think the plan that might make the most sense is to apply a new set of pads in the anterior-posterior position after the 3rd unsuccessful shock, provide one vector change shock (to limit the risk of machine damage while still gaining potential benefit), and then if that didn’t work try double sequential for the next attempt. I think the potential benefit is worth the relatively limited risk in a hospital setting. However, I will continue to emphasize that this is not standard of care, and this is not definitely proven, and we definitely need to see follow-up RCTs.
This is much more difficult if you work in the prehospital setting. The costs of double -sequential are much higher, so I think vector-change is probably the go to until you reach the emergency department.
If you work in a center with ECMO and immediate access to the cath lab, this may all be wasted time, as the best possible option might be to take the heart out of the equation until we can treat the underlying cause, but that is also far from proven.
Bottom line
DOSE VF is an RCT that demonstrated a mortality benefit from double sequential defibrillation (as well as vector change defibrillation), but the unblinded nature of the trial and the fact that it was not completed leave us with significant uncertainty.
Other DOSE VF FOAMed
If you want to hear the lead author talk about this paper, check out the AHA webinar Nov 11: https://heart.zoom.us/meeting/register/tZckc–rpz4jEtRYosZiZjdE6AggzbYWNal3
JC: Alternate defibrillation strategies in refractory VF. The DoseVF trial. St Emlyn’s
References
Cheskes S, Dorian P, Feldman M, et al. DOuble Sequential External Defibrillation for Refractory Ventricular Fibrillation: The DOSE VF Pilot Randomized Controlled Trial. Resuscitation. 2020; PMID: 32084567
Cheskes S, Verbeek PR, Drennan IR, McLeod SL, Turner L, Pinto R, Feldman M, Davis M, Vaillancourt C, Morrison LJ, Dorian P, Scales DC. Defibrillation Strategies for Refractory Ventricular Fibrillation. N Engl J Med. 2022 Nov 6. doi: 10.1056/NEJMoa2207304. Epub ahead of print. PMID: 36342151


9 thoughts on “Dose VF: A double sequential defibrillation game changer?”