Morgenstern, J. More medical dogma: The ‘golden period’ for laceration repair, First10EM, October 24, 2022. Available at:
https://doi.org/10.51684/FIRS.128601
This is the beginning of a long series looking at all the evidence around laceration repair in the emergency department. This evidence will also be covered in depth on the Emergency Medicine Cases Journal Jam podcast. We will look at preparation of wounds, including irrigation and the use of sterile gloves. We will talk about the many techniques we use to close wounds, from steri-strips to staples. We will question entrenched dogma, such as the need for wound eversion. And we will get into the weeds of aftercare, from dressings to topical antibiotics. Unfortunately, the quantity of content probably outweighs the quantity of evidence. It’s a bit of a spoiler, but be prepared for a recurrent refrain of “we just don’t know”.
Although the details vary, classic teaching in emergency medicine is that after a certain point in time, it is too risky to suture lacerations closed. We are told that the risk of infection goes up dramatically after 6, or is it 8, or maybe 12 hours? Therefore, these ‘late presenters’ should just be left alone to heal by secondary intent (or through a delayed primary closure, although I have never heard of that happening in real life). This recommendation never made physiologic sense to me. Why exactly would time matter? Contamination is contamination. Bacteria will multiply whether the skin is open or closed. Bacteria are microscopic. I guarantee you they are not being ‘trapped’ in the wound with a few sutures. And even if they were, they were already present when the patient presented at 1 hour, so how does time change anything? If anything, closing the wound creates a nice warm, moist environment for bacterial growth. Of course, our primary protection against infection is the immune system, but it is functioning in either scenario. More importantly, what is our alternative if the patient does present late? We are told to leave the wound open, but why would that decrease infection? If anything, because of the risk of continued exposure to contaminants, open wounds seem like the ones more likely to become infected.
Apparently, the idea of a golden period for laceration repair dates back to work by Paul Leopold Friedrich in 1898. I cannot find the original publication, which I think would be fascinating, but also possibly futile as I can’t read German. Basically, he cut the skin of guinea pigs, artificially contaminated them with bacteria, and then excised the entire wound (sort of like debridement on steroids?) at different time frames. If the excision happened after 6 hours, all of the guinea pigs died, and the concept of a golden period was born. Clearly, this is not at all applicable to our patients.
I have seen this concept quoted in a large number of sources. Unfortunately, there is almost never a citation to support the claim, and when there is, it either leads to another secondary source, or to a paper that is completely irrelevant. If these authors have good reason for making the claim, it is completely obscure to me, despite weeks of digging. So let’s look through the research that is available.
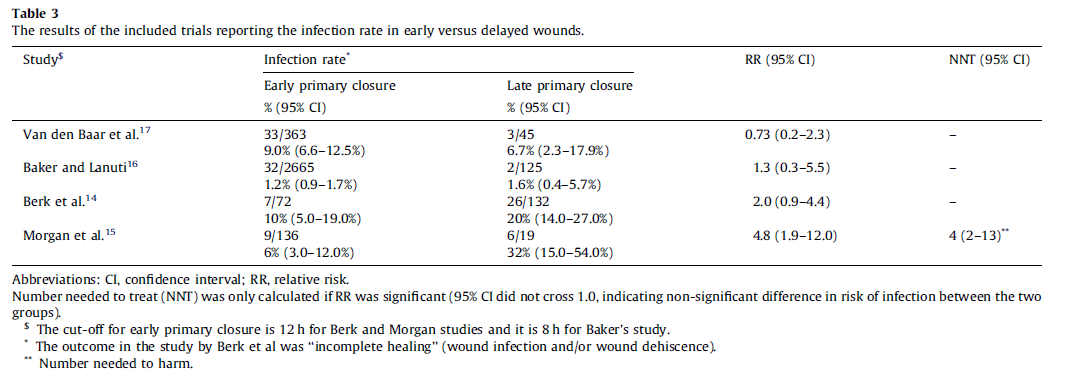
There is a systematic review of emergency department patients with simple lacerations, comparing outcomes in patients who presented early versus late. (Zehtabchi 2012) Definitions vary widely in the literature, so they just used whatever criteria the original papers used, which was either 6 or 12 hours. They found 4 studies, all of which were single center observational trials. There are a number of sources of heterogeneity in these studies, including use of antibiotics, which ranged from 100% of patients receiving prophylactic antibiotics to patients only being treated if they developed an infection. When comparing the rate of infection in the early closure versus late closure group, 3 of the studies were statistically insignificant, while one small study (with only 19 patients in the late group) had a relative risk of 4.8 (95% CI 2-13). The authors do not perform a meta-analysis, which I think is reasonable considering the significant heterogeneity of the studies found.
In a large, multicenter prospective observational trial looking to identify risk factors for infection in emergency department patients with lacerations, 3957 patients were enrolled, only 2663 had follow-up data (which is a problem), and the overall infection rate was 2.6%. (Quinn 2014) In keeping with other data, head and neck lacerations are less likely to be infected, while lower limb lacerations are more likely. Larger lacerations, increased contamination, and diabetes were all also associated with increased infection rates. On the other hand, the infection rate was the same in those presenting before and after 6 hours (3.7% vs 3.0%). Only 85 patients presented after 12 hours, and only 1 of them (1.2%) developed an infection. However, only 13 of these late presenters were closed, with the rest left to heal by secondary intention, so this data doesn’t really help us answer our primary question.
Another observational study of 5521 emergency department patients with lacerations found a 3.5% overall infection rate. (Hollander 2001) They found that diabetes was the biggest risk factor for infection, with wound width, and presence of foreign body also increasing risk, while lacerations on the head and neck decreased infection risk. Time from injury was not statistically significant. The average time from injury was 3.3 hours in infected patients and 2.6 in not infected (p=0.08).
Therefore, we have very little data to suggest that wounds that present late have an increased rate of infection. In fact, most of the data suggests the opposite. However, all of the studies have a high risk of bias. Confounders are probably key in this data, because people very rarely choose to delay care if they have other options. Furthermore, if someone does present late, clinicians often treat them differently, biasing observational data. We are left with significant uncertainty.
However, I don’t think any of this data really matters. These trials are asking the wrong question. It doesn’t matter whether delayed wounds have a higher infection rate than early wounds. It’s not like we are asking patients to wait before we repair their lacerations. This question only arises when a patient, for whatever reason, arrives late. At that point, it doesn’t matter if their infection rate is higher than it would have been if they had presented 6 hours ago. We don’t have time machines. The question we need to ask is, given that this patient has presented late, how does that affect management? Does suturing increase the rate of infection in this population?
As far as I can tell, there is not a single trial that compares primary to secondary intention healing in patients with lacerations who presented in a delayed time frame. There are also no trials comparing primary closure to delayed primary closure. A Cochrane review in 2013 looking for randomized trials comparing primary closure with delayed closure of non bite traumatic wounds didn’t find any that fit their inclusion criteria. (Eliya-Masamba 2013) I reviewed the papers they found and excluded, and agree that none have any relevance.
I am not sure that extrapolation from the surgical literature is at all meaningful in this scenario, but at least it gives us something to work with. As far as I can tell, there is really no good evidence for avoiding primary closure. There are numerous RCTs suggesting that primary closure after incision and drainage of cutaneous abscesses results in faster healing without complications and a similar rate of recurrence. (Singer 2011) A Cochrane review looking at primary closure after pilonidal cyst surgery found no difference in infection rate (and the point estimate actually favours closure), with a lower rate of treatment failure. (Al-Khamis 2010) A systematic review of primary versus delayed closure in complicated appendicitis found no difference in the rate of wound infection. (Henry 2005) However, the surgical literature is mixed. Another systematic review of delayed primary closure for dirty abdominal incisions found a significant decrease in skin and soft tissue infections (odds ratio, 0.65; 95% CI, 0.40-0.93; P = .02). (Bhangu 2013) However, the risk of bias was high across all studies, heterogeneity was high, and the result was not statistically significant using a random-effects model, so this result is very uncertain.
Summary
It is not even clear if the infection rate increases when patients present late after their injury. The highest quality data we have seems to suggest they don’t. If infection rates don’t change, there is no reason to treat these lacerations any differently than our usual lacerations.
However, the evidence is imperfect, and it is possible that there is a small increase in infection in patients presenting many hours after their original injury. If the infection rate was higher, we would have to ask: what is the best treatment option when faced with a wound at high risk of infection? There is not a single emergency department trial to help us answer this question, so there is no perfect answer. However, the surgical literature suggests better outcomes, without increased rates of infection, if you just suture right away. Physiologically speaking, that makes sense to me. Knowing basic biology, there is no reason that sutures should affect infection rates in this group of patients. What is your alternative? Open wounds definitely have a high rate of infection, and worse outcomes for other important factors, like cosmesis.
There are other reasonable questions to ask. Do patients presenting late warrant antibiotics? Does it impact your wound preparation or aftercare instructions? There doesn’t seem to be any science to answer those questions either. Personally, I just inform the patient that they might have a slightly higher risk of infection because of the delay, but repair the laceration exactly like I always do, and ask the patient to monitor closely for signs of infection.
Other FOAMed
SGEM 63: Goldfinger (more dogma of wound care)
Closing the Gap: The Golden Period
References
Al-Khamis A, McCallum I, King PM, Bruce J. Healing by primary versus secondary intention after surgical treatment for pilonidal sinus. Cochrane Database Syst Rev. 2010 Jan 20;2010(1):CD006213. doi: 10.1002/14651858.CD006213.pub3. PMID: 20091589
Bhangu A, Singh P, Lundy J, Bowley DM. Systemic review and meta-analysis of randomized clinical trials comparing primary vs delayed primary skin closure in contaminated and dirty abdominal incisions. JAMA Surg. 2013 Aug;148(8):779-86. doi: 10.1001/jamasurg.2013.2336. Erratum in: JAMA Surg. 2013 Oct;148(10):987. PMID: 23803860
Eliya-Masamba MC, Banda GW. Primary closure versus delayed closure for non bite traumatic wounds within 24 hours post injury. Cochrane Database Syst Rev. 2013 Oct 22;(10):CD008574. doi: 10.1002/14651858.CD008574.pub3. PMID: 24146332
Henry MC, Moss RL. Primary versus delayed wound closure in complicated appendicitis: an international systematic review and meta-analysis. Pediatr Surg Int. 2005 Aug;21(8):625-30. doi: 10.1007/s00383-005-1476-8. Epub 2005 Oct 13. PMID: 16044261
Hollander JE, Singer AJ, Valentine SM, Shofer FS. Risk factors for infection in patients with traumatic lacerations. Acad Emerg Med. 2001 Jul;8(7):716-20. doi: 10.1111/j.1553-2712.2001.tb00190.x. PMID: 11435186
Quinn JV, Polevoi SK, Kohn MA. Traumatic lacerations: what are the risks for infection and has the ‘golden period’ of laceration care disappeared? Emerg Med J. 2014 Feb;31(2):96-100. doi: 10.1136/emermed-2012-202143. Epub 2013 Jan 12. PMID: 23314208
Singer AJ, Thode HC Jr, Chale S, Taira BR, Lee C. Primary closure of cutaneous abscesses: a systematic review. Am J Emerg Med. 2011 May;29(4):361-6. doi: 10.1016/j.ajem.2009.10.004. Epub 2010 Mar 26. PMID: 20825801
Zehtabchi S, Tan A, Yadav K, Badawy A, Lucchesi M. The impact of wound age on the infection rate of simple lacerations repaired in the emergency department. Injury. 2012 Nov;43(11):1793-8. doi: 10.1016/j.injury.2012.02.018. Epub 2012 Mar 15. PMID: 22424703




7 thoughts on “More medical dogma: The ‘golden period’ for laceration repair”