
Morgenstern, J. COVID therapy: Neutralizing monoclonal antibodies, First10EM, January 22, 2022. Available at:
https://doi.org/10.51684/FIRS.124898
I have avoided COVID therapies for a while, because so many people are already covering the topic, and honestly I am a little sick of COVID. However, with the OMICRON wave, everyone seems to have questions about therapies for COVID, so a quick evidence review seems appropriate. This article will cover the evidence for neutralizing monoclonal antibodies (sotrovimab, bamlanivimab, or casirivimab+imdevimab) in COVID-19.
There are multiple forms of monoclonal antibodies being used in the treatment of COVID-19. Sotrovimab, bamlanivimab, and casirivimab+imdevimab are neutralizing antibodies that bind to SARS-CoV-2’s spike protein and prevent the virus from infecting human cells. They are a form of passive immunity. (You develop these antibodies yourself if you get vaccinated.)
Brand names make things confusing in medicine. Casirivimab + imdevimab is known as REGEN-COV in the United States and Ronapreve in Europe. Bamlanivimab has also gone by the chemical name LY-CoV-555. Apparently sotrovimab just goes by the brand name Sotrovimab.
A philosophical interlude
If this is the first post in this series that you are reading, it might be worth reading the philosophical interlude from part 1 of the series which explains why my conclusions sometimes differ from those of the Ontario Science Table.
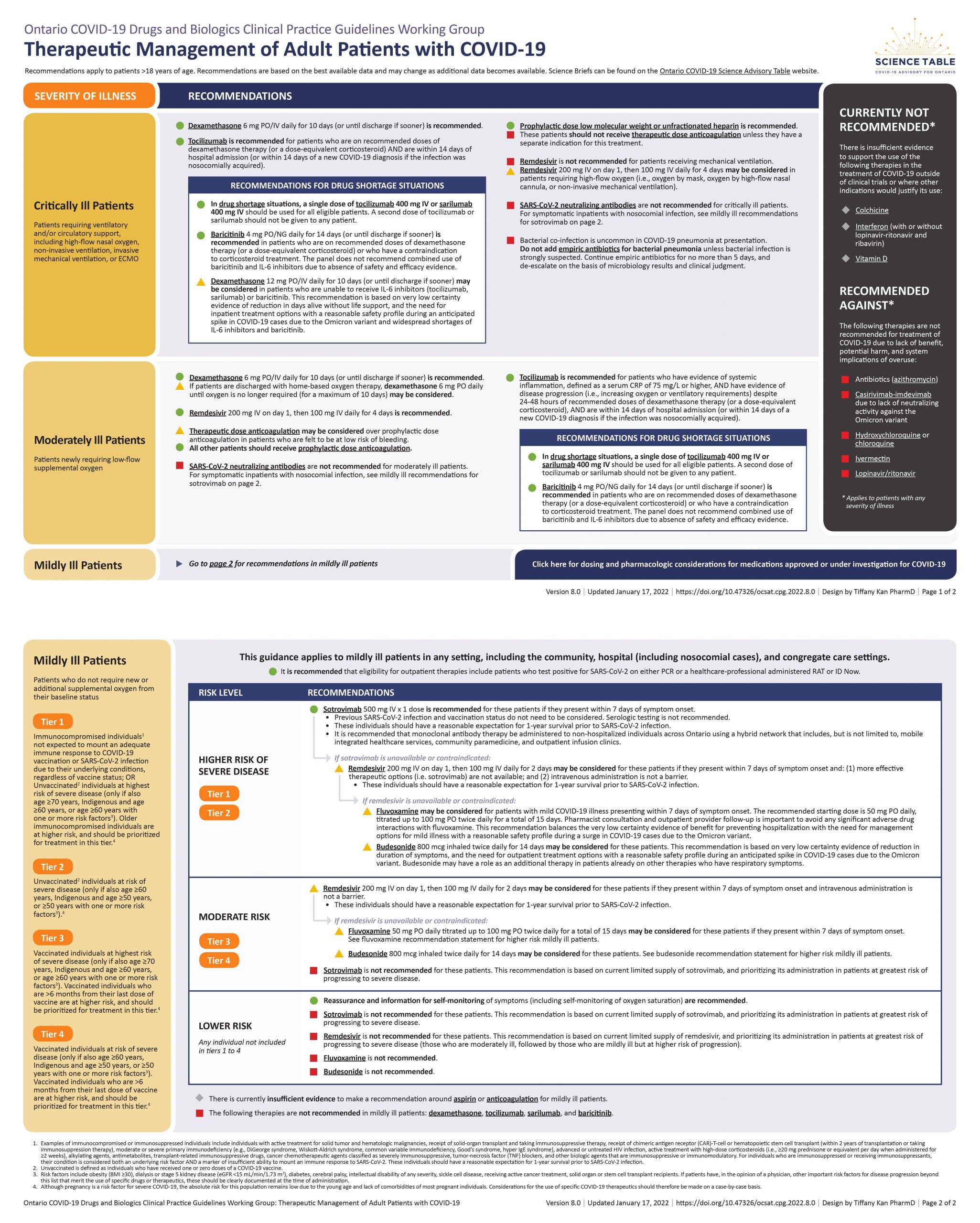
The Ontario Science Table recommendation
Sotrovimab
- Not recommended in critically ill or moderately ill patients.
- Recommended in patients with mild disease if they present within 7 days of symptom onsent, have a reasonable expectation of 1 year survival prior to COVID infection, and have a high risk of severe disease (tier 1 or 2 in their guidelines).
Casirivimab + Imdevimab
- Not currently listed in the guidelines.
Bamlanivimab is recommended against due to inadequate neutralizing activity against SARS-CoV-2 variants of concern.
(Science table recommendations available here)
The evidence for neutralizing monoclonal antibodies
Sotrovimab
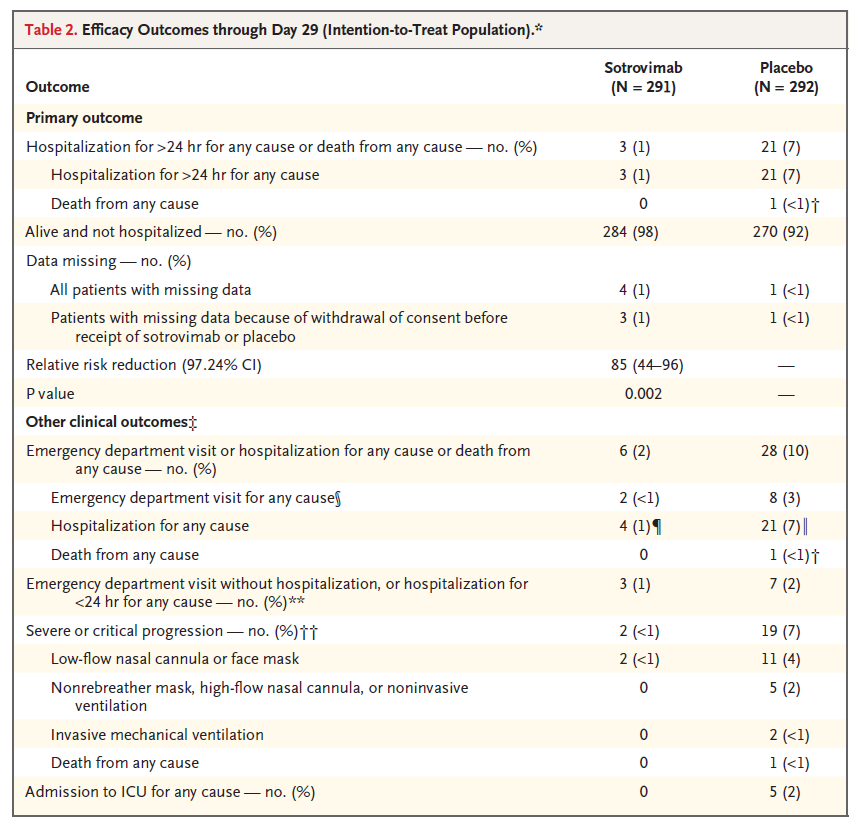
Sotrovimab was studied in a multi-center, double-blind, placebo controlled RCT of adult outpatients with confirmed COVID-19, presenting within 5 days of symptom onset, and at least 1 risk factor for disease progression. (Gupta 2021) They were randomized to sotrovimab 500mg IV or placebo. The primary outcome listed on clinicaltrial.gov (and the preprint) is different from the one stated in the NEJM publication, which should never occur, as research manuscripts are not meant to be works of fiction. The trial was stopped early (meaning it is likely to overestimate any benefits claimed). They randomized 868 total patients, of which 583 are included in the primary analysis. In terms of the currently listed primary outcome of hospitalization or death, it occured in 1% of the sotrovimab group and 7% of the placebo group (p=0.002). The secondary outcomes all also seem to favour sotrovimab. There are a few red flags in this study, which leaves the result far from certain. However, this study is much better than many we have seen in COVID, using a placebo, being blinded, and focusing on a patient important outcome. Bottom line: This RCT looks very promising. No single study will ever be definitive, so more research is definitely needed, but these results are probably convincing enough to use sotrovimab while waiting for more research.
Casirivimab + Imdevimab
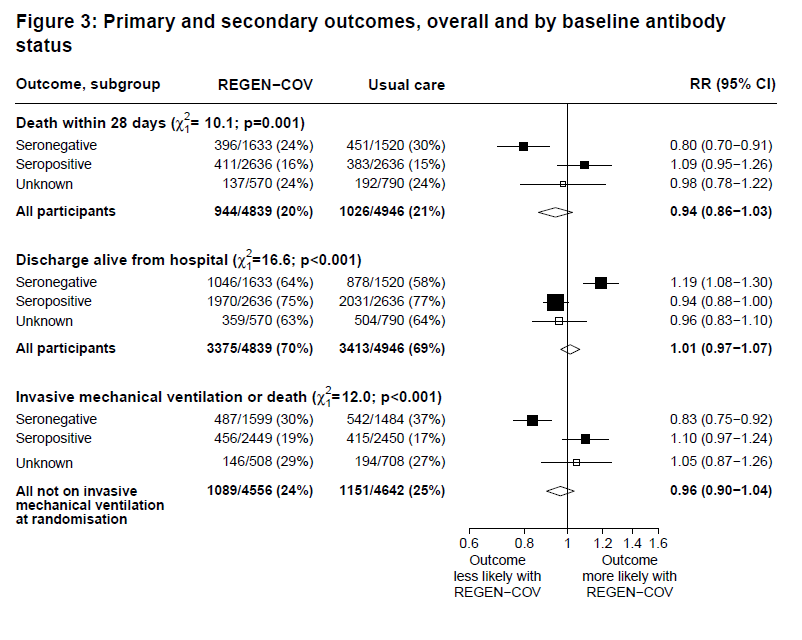
For some reason, despite being published in a preprint version in June 2021, the RECOVERY trial results are still not published in a peer reviewed journal. (Horby 2021) That is a bit of a red flag. Based on the preprint, the RECOVERY trial enrolled hospitalized patients over the age of 12 with confirmed or suspected COVID-19. 4839 patients were randomized to receive a single dose of casirivimab + imdevimab (8000 mg IV) and 4946 were randomized to usual care. (This was not a placebo controlled trial). The primary outcome was 28 day all-cause mortality, and there was no difference (20% vs 21%, p=0.17) There was also no difference in need for mechanical ventilation (24% vs 25%). However, 54% of this population had SAR-CoV-2 antibodies at baseline. Looking just at the seronegative population, there was a reduction in mortality (24% vs 30%, RR 0.80 0.70-0.91, p-value = 0.001). There was also a reduction in the need for mechanical ventilation (30% vs 37%, RR 0.83 CI 0.75-0.82, p < 0.001). Most subgroup analyses turn out to be wrong in medicine, and so they shouldn’t be used to guide clinical practice. If you tend to believe this subgroup analysis, then it is essential to also recognize the opposite side of the coin: if casirivimab + imdevimab is beneficial in seronegative patients, it also looks like it kills patients who are seropositive, which has massive implications for implementation, especially after vaccination. Bottom line: This is a clearly negative trial. It is unblinded, and so at high risk of bias. However, it includes an interesting and possibly important subgroup analysis that warrants future study.
Another trial looked at casirivimab + imdevimab in outpatients. (Weinreich 2021) It was a multi-center, placebo-controlled RCT. The protocol changed part way, so the data is somewhat messy. There were over 5500 patients randomized in the trial, but they only include 4057 in their primary data set. This data set included adult outpatients with laboratory confirmed COVID, within 7 days of symptom onset, and who had at least 1 risk factor for severe COVID. Patients were randomized to either 1200 mg of casirivimab + imdevimab, 2400 mg, or placebo. For the primary outcome (COVID specific hospitalization or death), there was a significant reduction (about 1% in both of the treatment groups and 3-4% in the placebo groups). Unfortunately, they used the inherently biased “COVID-19 related hospitalization” as part of their composite outcome with death, and as far as I can tell do not present all cause hospitalization numbers anywhere. Therefore, any hospitalization caused by an adverse event is systematically scrubbed from this data, and it is impossible to know whether the treatment actually decreases hospitalizations. They also don’t report other important, objective outcomes like need for oxygen, need for ICU, or need for mechanical ventilation. Symptom duration looks to be about 4 days shorter with treatment. This trial was funded, designed, and analyzed by the drug company, significantly increasing bias. Bottom line: This data, as presented, is very unconvincing, especially considering it is coming from the manufacturer of the drug. If the same benefit was present using all-cause hospitalization, I would count this as a win for the treatment, although it still has to be considered lower quality evidence with the number of protocol changes and active involvement of the manufacturer.
Casirivimab + imdevimab has also been looked at as a preventative agent. (O’Brien 2021) 1505 household contacts of patients with COVID-19 were randomized to 1200 mg of casirivimab + imdevimab or placebo subcutaneously. Importantly, all participants underwent serologic testing, and almost 1,000 who had serologic evidence of prior COVID infection were excluded. For the primary outcome of symptomatic COVID infection through 28 days, there was a significant reduction with casirivimab + imdevimab (1.5% vs 7.8%, p<0.001). Risk of bias is high considering the trial was funded by the manufacturer. Bottom line: Casirivimab + imdevimab may decrease symptomatic COVID infection in seronegative household contacts of confirmed COVID-19 cases, but the confidence in this outcome should be low given this is a single study and it is industry funded.
Bamlanivimab
Bamlanivimab is no longer suggested, as it does not bind effectively to the spike protein of the delta variant. (Planas 2021) As a result, I have not delved deeply into this literature. The BLAZE-2 study concluded that bamlanivimabreduced symptomatic COVID-19 infections in long term care facilities with at least 1 active COVID-19 infection (8.5% vs 15.2%, p < 0.001). (Cohen 2021)
Comments
Neutralizing monoclonal antibodies have a much stronger physiologic basis than many of the other COVID therapies we are testing. My pretest probability for these trials was set somewhat higher than it was for something like fluvoxamine. However, if they are going to work, they are likely to work early in the disease (when viral load and replication is high) rather than late in the disease (when inflammatory side effects take over). In my mind, this was confirmed by the clearly negative results of the RECOVERY trial.
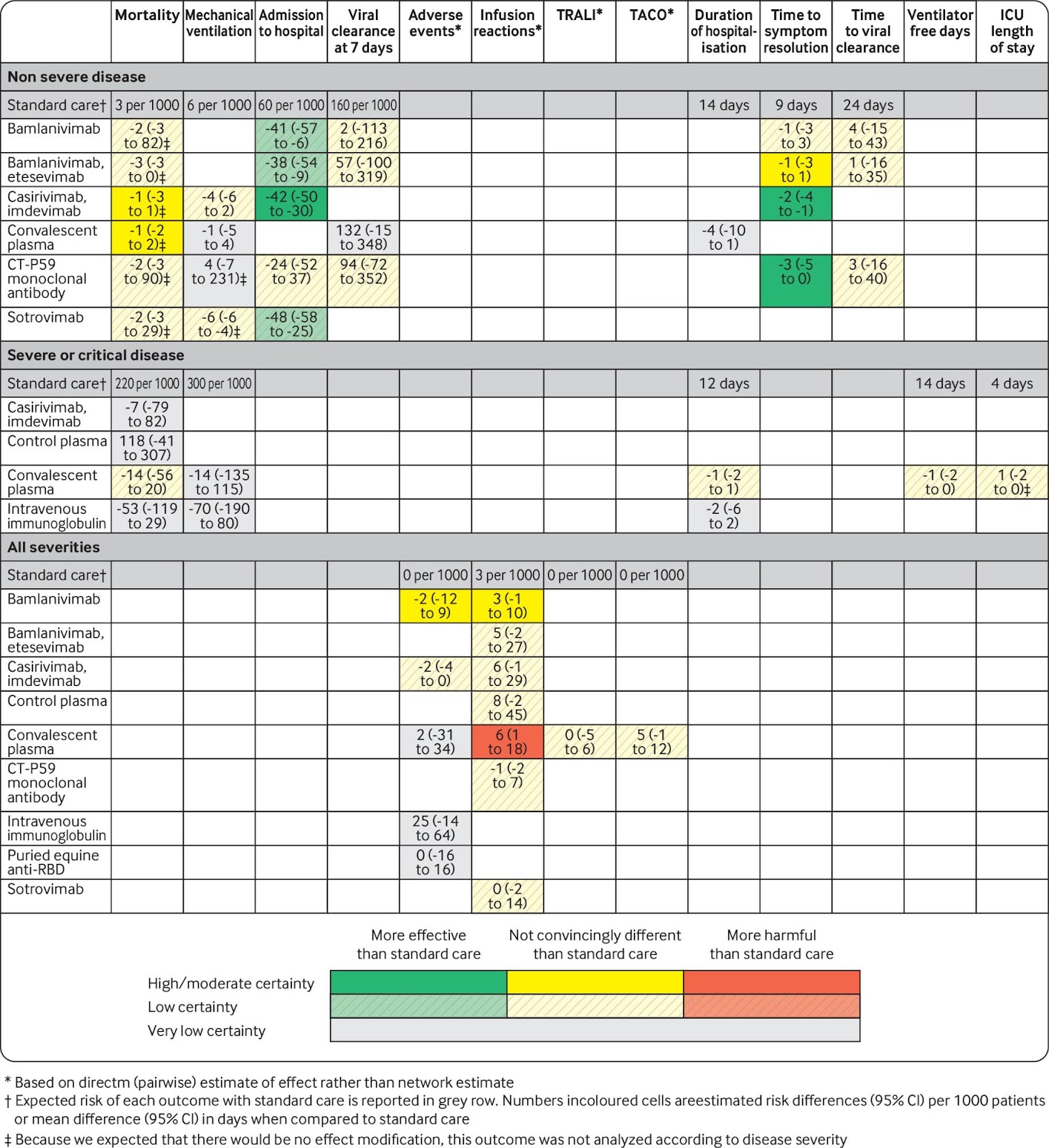
There is an excellent living systematic review and meta-analysis on the topic by Siemieniuk at el (2021). As always, meta-analyses tend to imply more certainty than really exists by glossing over issues of bias and just presenting numerical summaries. However, the table paints a pretty decent picture of the current evidence. There is no evidence these drugs are going to help patients who already have severe disease, which makes sense. These drugs are also clearly not wonder drugs, with no convincing differences in death or need for mechanical ventilation. However, they seem to be pretty consistent in showing a decrease in hospitalization and symptom reduction. The consistency in the hospitalization numbers across different agents in the class makes me more confidence in this outcome (although some of these hospitalization number are not real, as the study only looked at ‘COVID-specific hospitalizations’).
In general, we should not base clinical practice on subgroup analyses. They turn out to be wrong much more often than they turn out to be right. (There are numerous citations for this in the EBM bibliography.) It is tempting, during a pandemic, to ignore this classic EBM caution. Lives are at stake. However, in medicine, lives are always at stake, and getting this wrong will end up hurting patients. We have a long history demonstrating that subgroups are wrong much more often than they are right, so if you act on a subgroup you are likely to be wrong.
If you want to accept positive subgroups, you must also accept negative subgroups. If casirivimab + imdevimab looks positive in seronegative patients in the RECOVERY trial, it is only because it looks negative in seropositive patients. You cannot accept one claim without the other. Therefore, if you wanted to act on this subgroup, you would absolutely have to be running serology on all patients to avoid the harm in those who are seropositive.
In all these posts, I have cautioned about difficulties with extrapolation, given vaccination and novel variants. I think the impact of vaccination may be even more important here. In the RECOVERY trial, the patients who were seropositive did much worse. If real, it would indicate that these therapies may be harmful in vaccinated patients or those with prior infections, which in 2022 is the vast majority of patients. I have seen unvaccinated status drop off the criteria list for these treatments, but that might be a big mistake based on the RECOVERY results. (Either that, or the RECOVERY subgroup analyses are just false positives, like most subgroup analyses.) Either way, the best bet would be no benefit or harm in seropositive patients, and so it clearly shouldn’t be used.
Bottom line
Despite the incredible demand for these monoclonal antibodies, the evidence is far weaker than you would hope. If they have a role, it seems to be in outpatients, with the goal of avoiding hospitalization. We can’t be certain this effect is real, but it was seen consistently across agents, so I have moderate confidence. I think it is reasonable to use these agents in high risk outpatients, but with open acknowledgement of the significant remaining uncertainty and need for ongoing trials.
Based on the current data, it is pretty clear that neutralizing monoclonal antibodies should not be used in the inpatient population. The only study (RECOVERY) was clearly negative. I think it would be a mistake to base clinical practice on the subgroup findings of that trial, but if people are, they clearly need to be doing serology first, because otherwise they will end up causing harm.
Other FOAMed
Other First10EM COVID therapeutics updates can be found here
Ontario Science Table Recommendations
No Evidence that REGN-COV2 (Regeneron) Antibody Cocktail Has Clinical Benefits
RECOVERY Trial: The REGN-COV Antibody Cocktail in COVID19
BLAZE-1: COVID-19 Neutralizing Antibody (Bamlanivimab)
PulmCrit – I’m so confused about bamlanivimab
References
Cohen MS, Nirula A, Mulligan MJ, Novak RM, Marovich M, Yen C, Stemer A, Mayer SM, Wohl D, Brengle B, Montague BT, Frank I, McCulloh RJ, Fichtenbaum CJ, Lipson B, Gabra N, Ramirez JA, Thai C, Chege W, Gomez Lorenzo MM, Sista N, Farrior J, Clement ME, Brown ER, Custer KL, Van Naarden J, Adams AC, Schade AE, Dabora MC, Knorr J, Price KL, Sabo J, Tuttle JL, Klekotka P, Shen L, Skovronsky DM; BLAZE-2 Investigators. Effect of Bamlanivimab vs Placebo on Incidence of COVID-19 Among Residents and Staff of Skilled Nursing and Assisted Living Facilities: A Randomized Clinical Trial. JAMA. 2021 Jul 6;326(1):46-55. doi: 10.1001/jama.2021.8828. PMID: 34081073
Horby PW, Mafham M, Peto L, et al. Casirivimab and imdevimab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-abel, platform trial.; 2021:2021.06.15.21258542. https://doi.org/10.1101/2021.06.15.21258542
Gupta A, Gonzalez-Rojas Y, Juarez E, Crespo Casal M, Moya J, Falci DR, Sarkis E, Solis J, Zheng H, Scott N, Cathcart AL, Hebner CM, Sager J, Mogalian E, Tipple C, Peppercorn A, Alexander E, Pang PS, Free A, Brinson C, Aldinger M, Shapiro AE; COMET-ICE Investigators. Early Treatment for Covid-19 with SARS-CoV-2 Neutralizing Antibody Sotrovimab. N Engl J Med. 2021 Nov 18;385(21):1941-1950. doi: 10.1056/NEJMoa2107934. Epub 2021 Oct 27. PMID: 34706189
O’Brien MP, Forleo-Neto E, Musser BJ, Isa F, Chan KC, Sarkar N, Bar KJ, Barnabas RV, Barouch DH, Cohen MS, Hurt CB, Burwen DR, Marovich MA, Hou P, Heirman I, Davis JD, Turner KC, Ramesh D, Mahmood A, Hooper AT, Hamilton JD, Kim Y, Purcell LA, Baum A, Kyratsous CA, Krainson J, Perez-Perez R, Mohseni R, Kowal B, DiCioccio AT, Stahl N, Lipsich L, Braunstein N, Herman G, Yancopoulos GD, Weinreich DM; Covid-19 Phase 3 Prevention Trial Team. Subcutaneous REGEN-COV Antibody Combination to Prevent Covid-19. N Engl J Med. 2021 Sep 23;385(13):1184-1195. doi: 10.1056/NEJMoa2109682. Epub 2021 Aug 4. PMID: 34347950
Planas D, Veyer D, Baidaliuk A, Staropoli I, Guivel-Benhassine F, Rajah MM, Planchais C, Porrot F, Robillard N, Puech J, Prot M, Gallais F, Gantner P, Velay A, Le Guen J, Kassis-Chikhani N, Edriss D, Belec L, Seve A, Courtellemont L, Péré H, Hocqueloux L, Fafi-Kremer S, Prazuck T, Mouquet H, Bruel T, Simon-Lorière E, Rey FA, Schwartz O. Reduced sensitivity of SARS-CoV-2 variant Delta to antibody neutralization. Nature. 2021 Aug;596(7871):276-280. doi: 10.1038/s41586-021-03777-9. Epub 2021 Jul 8. PMID: 34237773
Siemieniuk RA, Bartoszko JJ, Díaz Martinez JP, Kum E, Qasim A, Zeraatkar D, Izcovich A, Mangala S, Ge L, Han MA, Agoritsas T, Arnold D, Ávila C, Chu DK, Couban R, Cusano E, Darzi AJ, Devji T, Foroutan F, Ghadimi M, Khamis A, Lamontagne F, Loeb M, Miroshnychenko A, Motaghi S, Murthy S, Mustafa RA, Rada G, Rochwerg B, Switzer C, Vandvik PO, Vernooij RW, Wang Y, Yao L, Guyatt GH, Brignardello-Petersen R. Antibody and cellular therapies for treatment of covid-19: a living systematic review and network meta-analysis. BMJ. 2021 Sep 23;374:n2231. doi: 10.1136/bmj.n2231. PMID: 34556486
Weinreich DM, Sivapalasingam S, Norton T, Ali S, Gao H, Bhore R, Xiao J, Hooper AT, Hamilton JD, Musser BJ, Rofail D, Hussein M, Im J, Atmodjo DY, Perry C, Pan C, Mahmood A, Hosain R, Davis JD, Turner KC, Baum A, Kyratsous CA, Kim Y, Cook A, Kampman W, Roque-Guerrero L, Acloque G, Aazami H, Cannon K, Simón-Campos JA, Bocchini JA, Kowal B, DiCioccio AT, Soo Y, Geba GP, Stahl N, Lipsich L, Braunstein N, Herman G, Yancopoulos GD; Trial Investigators. REGEN-COV Antibody Combination and Outcomes in Outpatients with Covid-19. N Engl J Med. 2021 Dec 2;385(23):e81. doi: 10.1056/NEJMoa2108163. Epub 2021 Sep 29. PMID: 34587383
Photo by Annie Spratt on Unsplash

{kind=link}
One thought on “COVID therapy: Neutralizing monoclonal antibodies”