In the Rapid Review series, I briefly review the key points of a clinical review paper (or two). The topic this time: Severe hypothyroidism (aka myxedema coma)
The papers:
Bridwell RE, Willis GC, Gottlieb M, Koyfman A, Long B. Decompensated hypothyroidism: A review for the emergency clinician. Am J Emerg Med. 2021 Jan;39:207-212. doi: 10.1016/j.ajem.2020.09.062 PMID: 33039222
Kwaku MP, Burman KD. Myxedema coma. J Intensive Care Med. 2007 Jul-Aug;22(4):224-31. doi: 10.1177/0885066607301361. PMID: 17712058
What is it?
This is one of those conditions where the name says it all (as long as you use the updated name). It is a state of severe, decompensated depletion of thyroid hormone. Considering the thyroid hormone’s key role in metabolism in essentially every organ system, the result is essentially ‘hypo-’ everything.
Who gets it?
This is a very rare condition, with an incidence of less than 1 case per million people per year. The most common population is women over the age of 60, especially those with a prior history of hypothyroidism.
What does it look like?
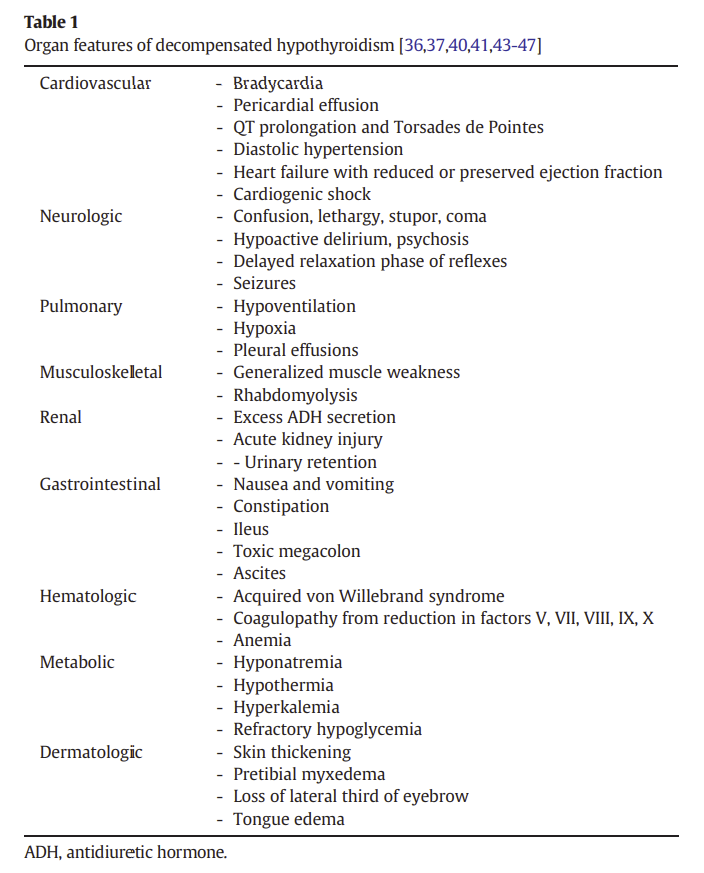
Unfortunately, the presentation is very non-specific, and so the diagnosis is very difficult to make (especially seeing as most emergency clinicians may only see 1 case in their career). The general picture is of someone with a suppressed metabolism – all systems are slowed down. The classic presentation is altered mental status in conjunction with bradycardia, hypotension, and/or hypothermia. Unfortunately, you can’t rely on any single finding. For example, although hypothermia is very common, the combination hypothermia and a febrile response may lead to a normal temperature reading. Furthermore, despite the name “myxedema coma”, most patients have neither coma nor myxedema.
Altered mental status is nearly universal. In addition to coma, patients can present with hypoactive delirium, psychosis, or psychomotor retardation. On neurologic exam, you might identify a delayed relaxation phase on reflexes (aka “hung up reflexes”). About 25% of patients will experience seizures, which can progress to status epilepticus based on underlying hypoglycemia, hypoxia, or hyponatremia.
Other signs and symptoms of hypothyroidism include constipation, fatigue, skin and hair changes, and loss of the lateral third of the eyebrow, among many others. Because pre-existing thyroid disease is common, be sure to examine the thyroid and review the patient’s medication list.
How is it diagnosed?
Considering the rarity of the disease and the range of clinical presentations, severe hypothyroidism will almost always be diagnosed based on laboratory findings. The key is including the diagnosis in your differential and sending bloodwork. Although I spend a lot of time cautioning about the perils of testing in low risk scenarios, the high mortality and nonspecific presentation of decompensated hypothyroidism mean that testing must be relatively liberal.
The TSH will be elevated in between 80% and 100% of patients. However, it will not be elevated in secondary hypothyroidism, and there are many other common factors (such as severe illness, steroids, and inotropes) thand can decrease TSH levels. Therefore, the free T4 level should be ordered in conjunction with the TSH.
Many of us now have rapid access to TSH and free T4 results, and so can wait for confirmatory testing before treating. However, if you work in a hospital without rapid laboratory testing, a clinical diagnosis and empiric therapy will be necessary. In a critically ill patient with altered mental status and either hypothermia or bradycardia, a single dose loading dose of levothyroxine is very safe and could be life saving.
Although TSH and T4 are very sensitive for severe hypothyroidism, the magnitude of the lab value does not correlate well with the severity of clinical presentation. Don’t exclude the diagnosis just because the labs ‘aren’t that bad’, and don’t over react to extreme lab values in a patient who is clinically well.
What other tests are necessary?
Other testing will be required to search for a precipitating cause (discussed below), as well as to complete the workup of altered mental status. The hypothyroidism can also precipitate hypoglycemia and hyponatremia, although I assume you will be checking those values without my saying so.
Is myxedema coma different from decompensated hypothyroidism?
No. However, the older terminology of “myxedema coma” is problematic because most patients don’t have myxedema and most patients aren’t fully comatose, so the terminology sets us up to fail. Severe or decompensated hypothyroidism is probably a better name for that reason.
What causes it?
Although decompensated hypothyroidism can occur spontaneously, it is most often precipitated by a trigger. Infection is the most common trigger, but basically any major stressor can precipitate severe hypothyroidism, including CVAs, GI bleeds, pulmonary embolism, surgery, and trauma. There are also numerous medications, such as amiodarone, lithium, iodinated contrast, opioids, sedatives, SSRIs, beta-blockers, and antipsychotics, which can precipitate decompensated hypothyroidism. Cold weather can also push compensated hypothyroidism into decompensated, which is why most cases occur in the winter.
How is it treated?
There is an accompanying “first 10 minutes” resuscitation post that goes into more detail. These patients will require meticulous supportive care, including appropriate management of their airway, hemodynamics, temperature, electrolytes, and underlying conditions. Definitive management involves administration of thyroid hormone and corticosteroids. Give steroids (hydrocortisone 100mg IV) before levothyroxine, as thyroid hormone can precipitate an adrenal crisis. Levothyroxine (T4) is the first line therapy, with a 100-500 mcg IV loading dose. (Lower doses are often used in elderly patients and those with significant cardiac disease). Some specialists will add T3, but it is controversial, and so should be done in collaboration with your endocrinologist.
What is the prognosis?
This is an incredibly deadly disease, with a mortality rate between 30 and 60%. Delays in diagnosis and management are thought to contribute to that high mortality, so this is a condition where we can potentially make a huge difference in the emergency department.
Other FOAMed
First 10 minute approach to resuscitation
IBCC: Decompensated Hypothyroidism (“Myxedema Coma”)
References
Bridwell RE, Willis GC, Gottlieb M, Koyfman A, Long B. Decompensated hypothyroidism: A review for the emergency clinician. Am J Emerg Med. 2021 Jan;39:207-212. doi: 10.1016/j.ajem.2020.09.062 PMID: 33039222
Kwaku MP, Burman KD. Myxedema coma. J Intensive Care Med. 2007 Jul-Aug;22(4):224-31. doi: 10.1177/0885066607301361. PMID: 17712058
Morgenstern, J. Severe decompensated hypothyroidism (aka myxedema coma) – A rapid review, First10EM, July 5, 2021. Available at:
https://doi.org/10.51684/FIRS.79166