Outside of asthma or COPD, I have never prescribed steroids for community acquired pneumonia. Almost everyone has heard that dexamethasone might decrease mortality in COVID, but it is possible we should be using steroids in CAP as well. Although I have heard rumors of benefit for years, I have never seen steroids prescribed for pneumonia, so this literature deep dive has always sat on the back-burner. Today I will finally try to answer the question of whether we should be prescribing steroids for all our pneumonia patients. (If you don’t want to read the whole article, the answer is no.)
The Systematic Reviews
Based on the various systematic reviews on this topic, it is incredibly surprising that more people aren’t prescribing steroids for pneumonia. They all conclude fairly strongly that there is a benefit – and not just any benefit, but a mortality benefit – with very little harm. How is it that we prescribe so many medications with little to no benefit, but ignore a cheap and relatively safe treatment for a common problem that apparently saves lives?
The 2011 Cochrane review concluded that there was a decreased need for mechanical ventilation, decreased progression to ARDS, and decreased hospital length of stay with steroids, although there was also increased hyperglycemia. All cause mortality was not statistically different, but it was close to showing a benefit with a relative risk of 0.7, but the 95% CI touched 1 (0.4-1.0). (Chen 2011)
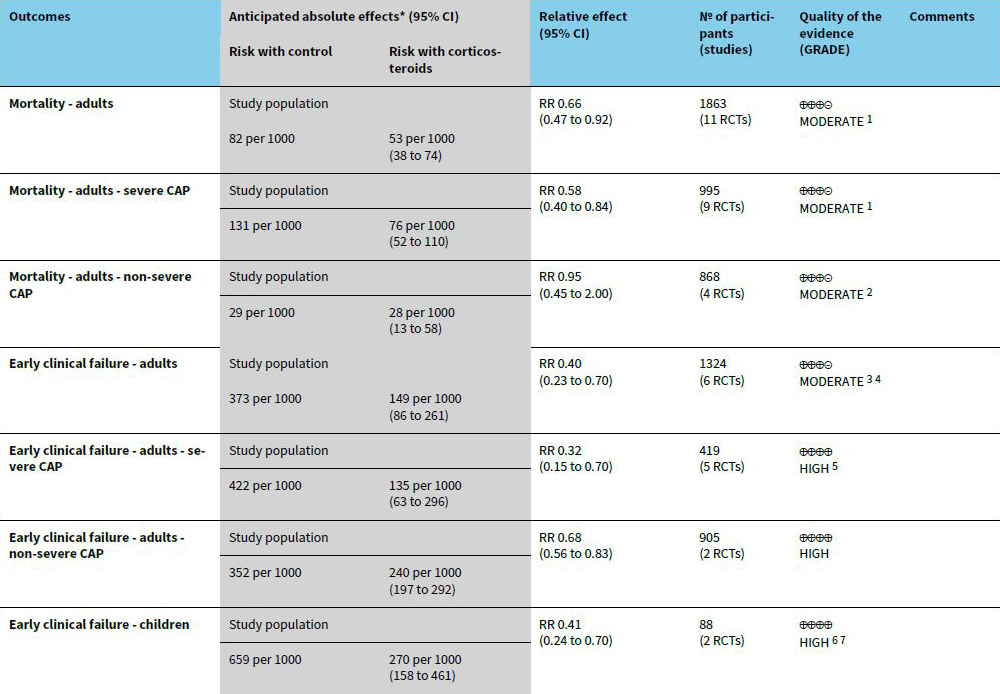
The 2017 Cochrane update added 12 new studies, bringing the total to 17 RCTs encompassing 2264 patients. This time, there was a decrease in all cause mortality (8% vs 5%, RR 0.66, 95% CI 0.47-0.92), based on what they call a moderate quality of evidence. However, when they break it down by subgroup, the mortality benefit is only seen among patients with severe pneumonia, and not with those with “non-severe”. (Stern 2017)
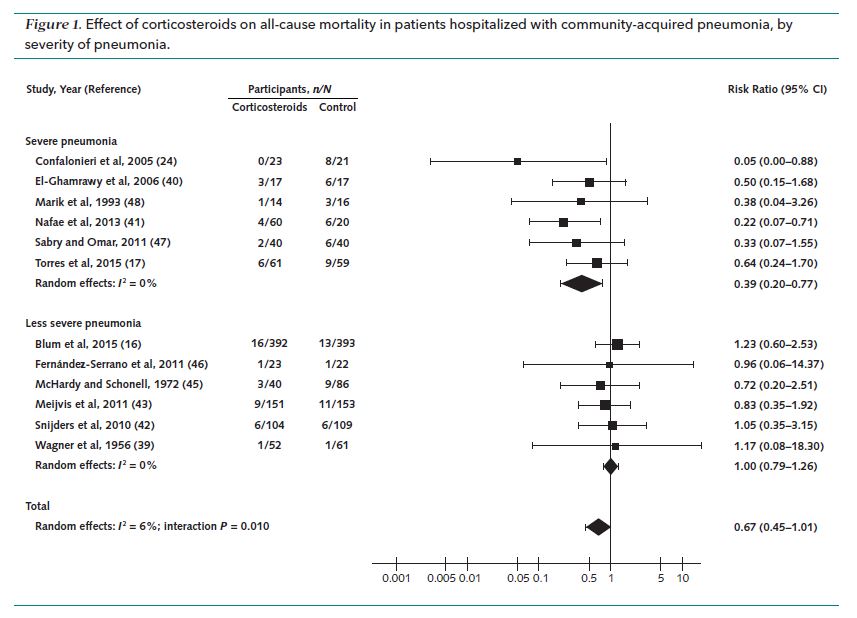
Another systematic review focused only on patients with severe pneumonia and similarly found a decrease in overall mortality (7.5% vs 13%) and a decrease in ICU length of stay. Interestingly, in a subgroup analysis, patients younger than 63 benefited from steroids, whereas those older than 63 did not. Might older patients, with less robust immune responses to pneumonia, gain less from steroids while simultaneously being higher risk for adverse events? (Or maybe this was just another spurious subgroup.) They report no difference in adverse events, but many of the trials didn’t even report harms, so harm data is available for less than one third of the total patients. (Huang 2019)
Overall, those numbers sound pretty good. However, there are a couple reasons to be hesitant. First of all, the trials are all pretty small. The 17 trials in the Cochrane review had a total of 2264 patients, which is only an average of 133 patients per trial. (Stern 2017) Smaller trials, in general, tend to be lower quality. With a predominance of small trials, there is also a much higher chance of publication bias, as it is much more likely that a 100 person trial goes unpublished than a 1,000 person trial.
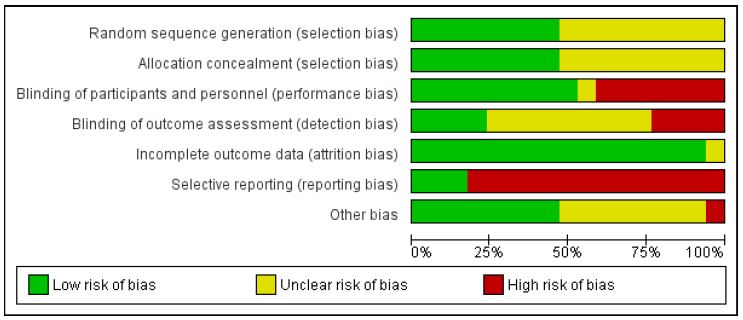
The biggest problem with meta-analyses is that they tend to erase the most important aspect of the individual trials: the various sources of bias. Across all the domains ranked, the Cochrane review rated the risk of bias as high or ‘unable to determine’ for at least half the studies, but it is hard to know how important those sources of bias are without reading the actual studies, so let’s look at some of the RCTs.
The RCTs
I am not going to go through all the available RCTs, but I have selected a handful of the most important trials so that you can get a sense of the strengths and weaknesses of this data.
Confalonieri 2005
This is a small RCT that enrolled 46 adult ICU patients with pneumonia in 6 Italian ICUs and randomized them to either placebo or hydrocortisone (200 mg IV bolus and then an infusion of 10 mg/hour for 7 days).
Results: The non-patient-oriented primary outcome (improvement in the PaO2:FiO2 ratio) was better in the treatment group. Survival to hospital discharge was dramatically different, with a 30% mortality in the placebo group and a 0% mortality with hydrocortisone (p=0.009).
Comments: There are some major problems with this study. It is a very small trial, looking at a very select group of patients. They only included 46 patients despite the trial running at 6 hospitals for 3 years (each trial contributed 2.5 patients a year). Given that these are just adult patients with pneumonia, selection bias is a major concern. Given the small size of the trial, it is not surprising that the groups are not very similar at baseline, but the fact that the average age in the placebo group was 67 as compared to 60 in the treatment group could easily impact the outcomes. There was no set sample size. The plan was to check the data every 20 patients until their primary outcome was accomplished, which is one of the major forms of p-hacking, and really bad science. (This is because a p value is likely to be “statistically significant” at some point by chance alone. You won’t stop the trial if it is ‘negative’, but will if it is ‘positive’, completely invalidating the meaning of the p value.) Furthermore, this study was not registered. That might not matter a lot for this study, although we cannot check whether their protocol changed, but it does increase the chance of similar studies from the era being unpublished, generating publication bias. The numbers are also somewhat unbelievable (probably as a result of the small size and biased stopping method.) These are ICU pneumonia patients and the mortality in the hydrocortisone group was 0%. That is the definition of too good to be true.
Bottom line: This trial is a biased mess and I don’t trust the results.
There are a number of similar small, flawed trials, but this one is the most frequently cited because of its dramatic and somewhat unbelievable results. Let’s move on to somewhat larger and higher quality trials.
Meijvis 2011
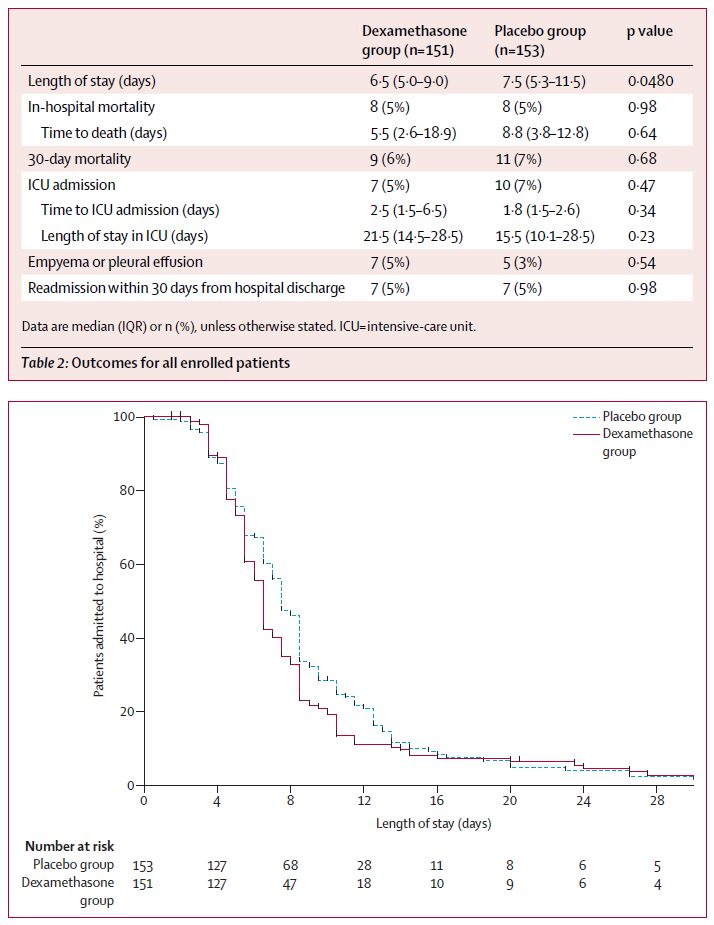
This is a randomized, double-blind, placebo controlled trial that enrolled 304 adult patients with community acquired pneumonia. They excluded ICU patients and patients with risk factors for adverse events from steroids. They compared dexamethasone 5mg IV daily for 4 days to placebo.
Results: Their primary outcome was hospital length of stay, and it was decreased in the dexamethasone group (6.5 versus 7.5 days, p=0.048). There were no differences in mortality, ICU admission, or readmission. They don’t comment on side effects.
Comments: This is a well designed trial, but the primary outcome is imperfect. Length of hospital stay is subjective. Steroids are anti-inflammatories that will change things like fever and heart rate, which in turn will change the physician’s decision about whether to discharge a patient. However, that decision doesn’t necessarily indicate that the patients were any healthier or any more ready to go home. A p value that just barely sneaks under 0.05 is also always suspicious. The p value 0.04 occurs far more often than is mathematically plausible in the medical literature, which means some trials must be cheating to obtain that number. To be clear: there is absolutely no indication that this trial is cheating, but we know that there are too many trials with a p value of 0.04 for all of them to be true. A final concern is that they didn’t report adverse events, which would be important seeing as none of the patient important outcomes were changed in this study.
Bottom line: Although the primary outcome is positive, this trial is negative for all the outcomes that matter to me (and patients) and so would not change my practice. On its own, this trial would not convince me to prescribe steroids.
Nafae 2013
This is a partially blinded RCT that compared hydrocortisone (200mg IV bolus then 10 mg/hr infusion for 7 days) to placebo in 80 adult patients with community acquired pneumonia.
Results: There were more pneumonia complications, as defined by septic shock and ARDS, in the placebo group than the hydrocortisone group (30% vs 6.7%, p<0.05). Mechanical ventilation was not statistically different, but occurred half as often in the treatment group. Hypokalemia was higher with steroids, but other adverse events were not statistically different. Mortality was lower in the hydrocortisone group (7% vs 32%, p<0.05).
Comments: The trial was only single blind. There was no stated primary outcome. This trial is not in a pubmed indexed journal, which is a bit of a red flag. There was no sample size calculation, which increases the chance of p hacking. They don’t discuss important methodologic issues, like allocation concealment. Their definition of pneumonia complications seems objective, but probably isn’t on closer inspection. Septic shock is often defined by vital signs, and may not represent the true perfusion status of the patient. Similarly, a clinical diagnosis of ARDS might be based on imaging, which might be changed by steroids without truly improving patient outcomes. Even mortality could be subjectively influenced, if the vital signs influence prognostic decisions and DNR discussions.
I said I was going to pick out the most important RCTs, and this is a pretty crappy small trial. I include it because it actually makes up 12% of the overall weight of the Cochrane review’s mortality meta-analysis, which I think is very telling about the overall quality of this data. (Stern 2017)
Bottom line: The outcomes look a lot better with steroids in this trial, and the improved outcomes are truly patient oriented, but the quality of the study is very low.
Torres 2015
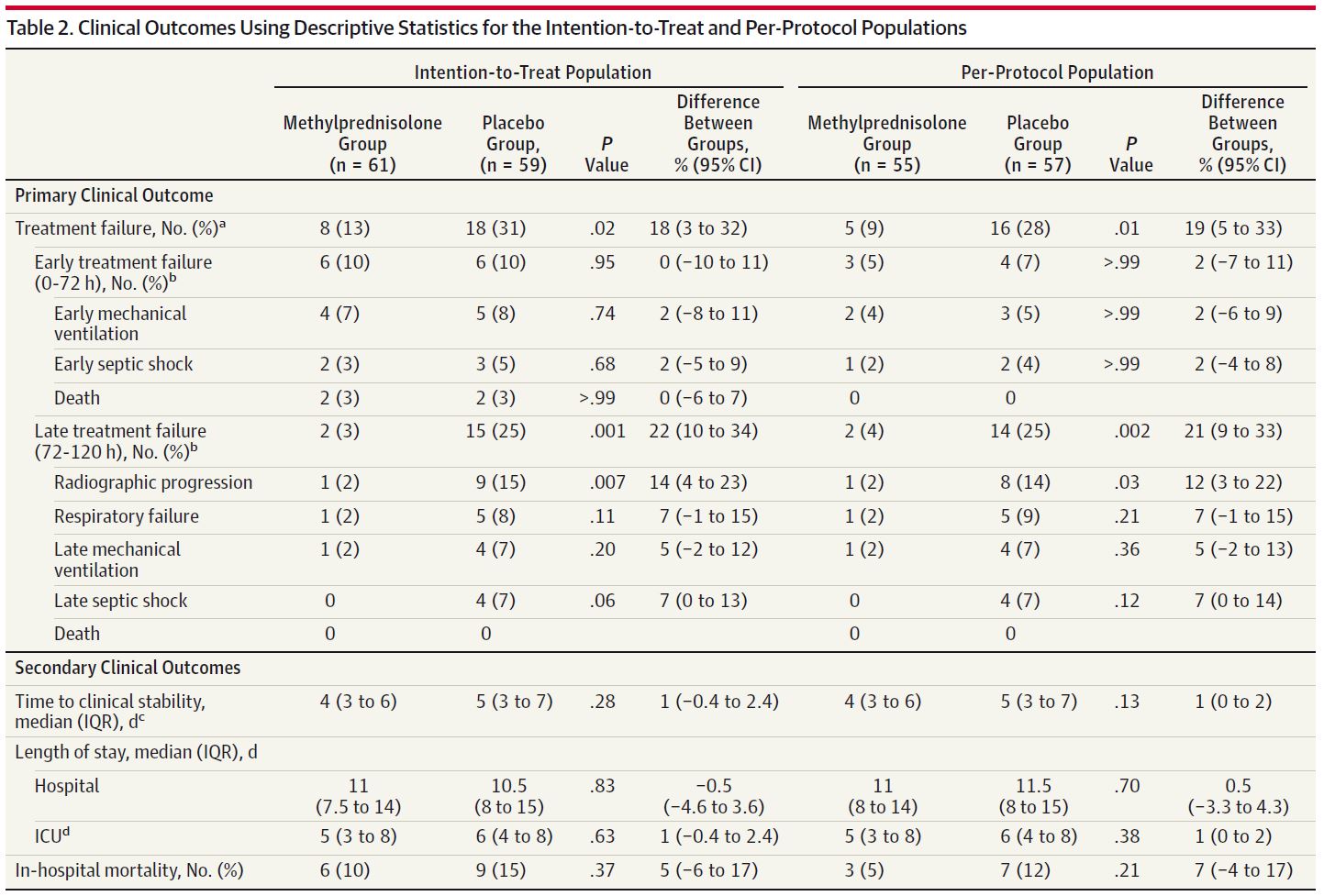
This is a multicenter, double-blind, placebo controlled RCT comparing methylprednisolone (0.5 mg/kg IV every 12 hours for 5 days) to placebo in adult patients with severe pneumonia (ATS guideline definition or PSI V) and a CRP greater than 150 mg/L in 3 hospitals in Spain. They chose to look at high CRP patients as they believed the anti-inflammatory effects of steroids would be most helpful in the patients with the highest inflammatory response.
Results: They screened 519 patients and enrolled 120. There was less “treatment failure” in the steroid group. However, this is a broad composite outcome. There was no difference in early treatment failure, and essentially the entire difference in late treatment failure was the result of a lack of radiographic progression of disease. Death as part of treatment failure (within 5 days) was identical in both groups (3%). In hospital mortality wasn’t statistically different, but does look potentially better in the steroid group (10% vs 15%, p=0.37), but seeing as this is only the difference between 6 and 9 total deaths, it is probably due to chance alone, as the p value suggests.
Comments: It makes sense to try to find a high risk subgroup, but using CRP as an inclusion criteria limits the generalizability of these results. Selection bias is again a major concern. They excluded the majority of patients screened, including 100 for “other reasons” in a 120 person trial. More importantly, they only screened 519 patients over the course of 8 years at 3 hospitals, and I have to believe that there are more than 20 pneumonia patients a year in a normal hospital. They were pretty optimistic in their sample size calculation, assuming they were going to see a 20% reduction in treatment failure, and that potentially leaves the trial underpowered for other outcomes, like mortality. The biggest concern about this trial is that it was not registered until after data was being collected, and even then the registered primary outcome does not seem to be the primary outcome they used in the paper. (NCT00908713)
Bottom line: Although this is a positive trial, the only outcome changed was a radiologic outcome that I don’t think I care about. The patient oriented outcomes were all unchanged, although it is possible the trial was underpowered for smaller, but still important, differences.
STEP Trial – Blum 2015
This is a multicenter, double-blind, placebo controlled, RCT comparing prednisone (50 mg daily for 7 days) to placebo in adult patients with community acquired pneumonia at 7 hospitals in Switzerland.
Results: They enrolled 802 patients (out of 2911 screened). The primary outcome – time to clinical stability – was better in the steroid group (3 days versus 4.4 days, p<0.0001). However, there was no difference in mortality (4% vs 3%), ICU admission (4% vs 6%), recurrent pneumonia (6% vs 5%), or readmission to hospital (9% vs 8%). There was more hyperglycemia in the steroids group (19% vs 11%).
Comments: As a primary outcome, I think that “time to normal vitals signs” is very likely to be misleading or irrelevant in a study of steroids. I expect steroids to improve vitals signs. Neither I nor my patient cares about vitals signs if they aren’t related to important clinical outcomes, and none of the clinical outcomes were better in this trial. As a broken record, I will point out the potential for selection bias with so many patients excluded, and therefore the limited generalizability of these results.
Bottom line: This is the biggest trial we have, and it is well done. Although it is a positive trial based on a disease oriented outcome, there do not appear to be any improvements in patient oriented outcomes. This trial does not convince me to change practice.
IMPROVE-GAP – Lloyd 2019
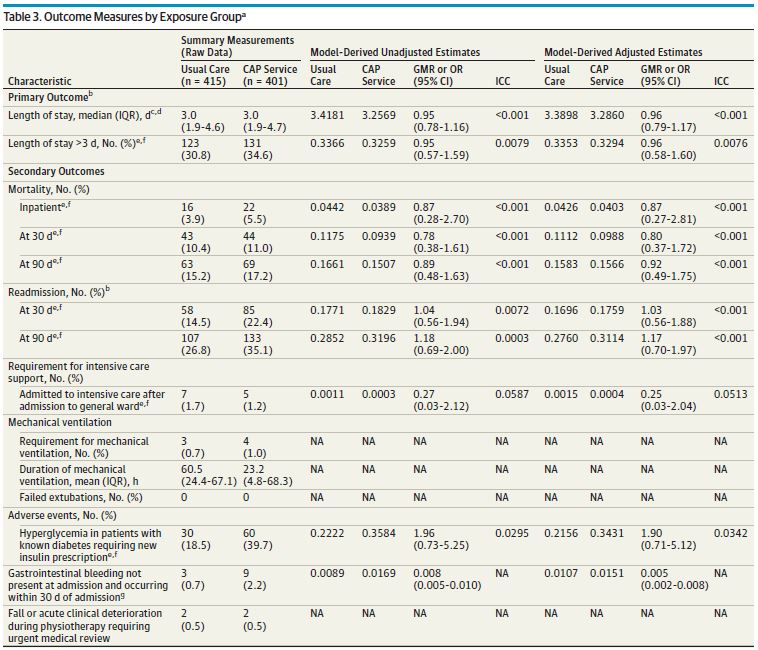
The IMPROVE-GAP trial is a stepped-wedge, cluster randomized trial from 8 general internal medicine units at 2 hospitals in Australia. They attempted to implement a bundle of 4 interventions that all had reasonable evidence to improve outcomes in pneumonia, including steroids, a rule based switch from IV to oral antibiotics, early mobilization, and screening for malnutrition. Obviously the combination of 4 interventions makes it harder to comment on steroids specifically, but the other 3 all seem like reasonable interventions.
Results: They included 816 patients. Unfortunately, as this is a real world trial, the compliance in the groups is far from perfect. Only 75% of the patients got the steroid prescription they were supposed to, and 25% of the patients who were not supposed to receive steroids got at least one dose (although usually a lower dose and for a shorter time than the treatment group). There was no change in the primary outcome of length of stay. There was no change in mortality or readmission, although all the numbers actually look a little worse in the intervention group. The only significant changes were a doubling in new insulin prescriptions in the treatment group and a small increase in GI bleeds (2.2% vs 0.7%).
Comments: A major benefit of this study is that it included almost all pneumonia patients, avoiding the significant selection bias and ascertainment bias that was present in many of the other trials. This might be more representative of the results we can expect in the real world setting. However, by including everyone and testing multiple interventions, it is possible they missed a benefit in a subgroup of patients, or that one treatment was helping while others were hurting.
What about influenza?
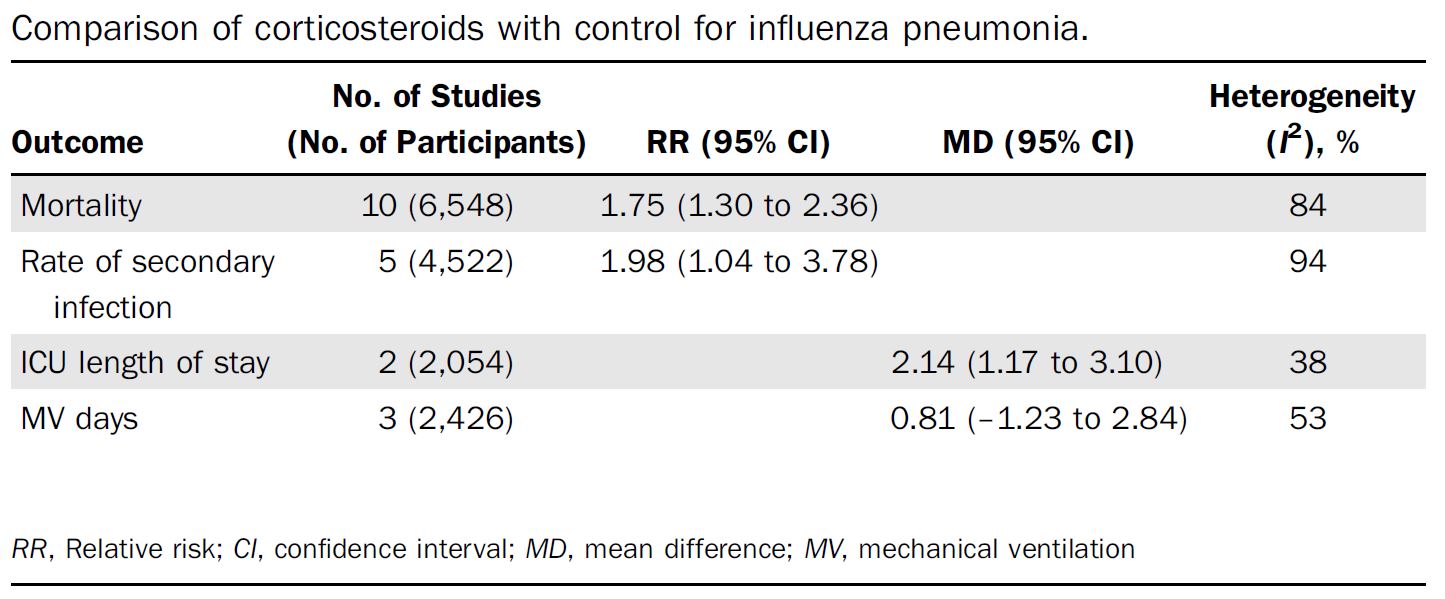
The focus of this review is community acquired pneumonia, but depending on the season, influenza is more common, and may also give us more insight into whether to expect steroids to work in COVID. (This article was written a long time ago, before the COVID research was published. This is the blog post on steroids in COVID.) Unfortunately, the data in influenza is very poor. One systematic review found 10 trials encompassing 6548 patients, and concluded that steroids were associated with an increased risk of mortality, an increased rate of secondary infection, and an increased ICU length of stay in influenza. (Ni 2019) However, there were no RCTs. All the data was observational, and therefore at high risk of bias, and half of the studies were retrospective. I can imagine that it is much more likely that sicker patients will receive steroids, and that confounder alone could completely explain these results. I wouldn’t be rushing to give steroids to influenza patients, but I don’t think this data is strong enough to actually conclude that they are harmful.
What about pediatrics?
According to a 2017 systematic review, there have been 4 RCTs looking at steroids in pediatric pneumonia. There is no change in mortality, because there were no deaths in either group in any of the studies. There was a benefit in terms of “early clinical failure” (RR 0.41, 95% CI 0.24-0.70). However, I don’t think that early clinical failure is necessarily an important outcome. It is made up of radiographic progression and clinical instability. Those sound like important objective outcomes, but I think they could easily mislead. Tachycardia could be a marker of clinical instability. As an anti-inflammatory, I would expect steroids to result in lower heart rates, but that doesn’t necessarily mean that the patient is better. In fact, it would be easy to imagine steroids improving the vital signs, but still resulting in worse outcomes. As an analogy, imagine treating the tachycardia of sepsis with diltiazem. The heart rate will improve, but the patient will probably do worse.
There is observational data that suggests that children do worse when given steroids, but much like the influenza data, my guess is that confounders are primarily to blame. (Ambroggio 2015) That being said, it is important to know that the data is not universally positive when it comes to steroids.
What do the guidelines say?
The joint Infectious Disease Society of America (IDSA) and American Thoracic Society (ATS) guideline suggests that steroids should not be used routinely in patients with nonsevere community acquired pneumonia (strong recommendation, high quality of evidence), should not be used in patients with severe pneumonia (conditional recommendation, moderate quality of evidence), and should not be used in patients with severe influenza pneumonia (conditional recommendation, low quality of evidence). They do endorse the Surviving Sepsis Campaign recommendation that steroids be used in patients with CAP and refractory septic shock. They do acknowledge that multiple trials demonstrate reduced mortality in severe pneumonia, and I don’t think their discussion section is adequate enough to explain the transition from that data to a recommendation against steroids, but after reviewing the studies myself, I understand their conclusion. (Metlay 2019)
Ongoing studies
There are a number of ongoing studies to be aware of (and I will update this post when I find new data).
NCT02517489: The CAPE COD study is a placebo controlled RCT looking at hydrocortisone in community acquired pneumonia. They are supposed to enroll 1200 ICU level patients, and it should be completed by January 2021. They modified the study this year to include COVID patients, which makes sense, but might muddy the results from a CAP standpoint. This would be, by far, our biggest trial to date.
NCT01743755: The Santeon-CAP was an RCT comparing dexamethasone to placebo in adult pneumonia patients. They were supposed to enroll 600 patients, but the study stopped enrollment after only 413. It has been 2 years since the trial stopped and no data has been published yet, which tends to indicate the results were negative, or even harmful.
NCT01283009: The Extended Steroid in CAP(e) (ESCAPe) trial also finished enrolling patients 4 years ago, but the results haven’t been published yet. It is a trial of methylprednisolone in critically ill adult patients with CAP.
Discussion
Most of these things have been mentioned above, but there were a few big issues that came up repeatedly as I tried to grapple with this literature.
Patient vs Disease oriented outcomes
One reason that I ignored a number of these RCTs as they were published was their focus on disease oriented outcomes. Multiple trials have demonstrated decreases in hospital length of stays, improvement in vital signs, or changes on x-ray, but I worry that those outcomes could be misleading, especially in the context of steroids. Simply improving vital signs doesn’t necessarily improve outcomes. (Again, imagine giving diltiazem to correct tachycardia in a patient with septic shock.) Hospital length of stay seems valuable to patients, but decisions about discharge will often be based on fever and the other vitals signs, which will be improved with steroids even if there is no real patient oriented benefit. To accept these surrogate outcomes, we need to see much larger trials demonstrating safety.
Furthermore, length of stay is often based on idiosyncratic differences in care. For example, when looking at the coronary CT angiogram literature, the one “benefit” seen in trials is a decrease in length of stay, but the baseline stays are often 24 hours for patients who never needed admission at all. The same is true in many of these studies, where patients with PSI classes 1-3 are staying in the hospital for 7 days, when they may have never needed the hospital in the first place. (Chalmers 2016)
Mortality is a pretty important and objective outcome, although the subjectivity of mortality in modern ICU settings is an important topic to acknowledge in many critical care studies. The systematic reviews indicate a mortality benefit, but the underlying studies just aren’t that strong. This is analogous to the literature for TXA for GI bleed before the publication of HALT-IT. Like HALT-IT, what we really need here is a large, high quality RCT to definitively determine whether steroids decrease mortality in community acquired pneumonia.
Exclusions
Almost all of these studies excluded patients at high risk of complications from steroids. That includes patients with previous GI hemorrhage, sometimes patients with risk factors for GI hemorrhage, poorly controlled diabetes, and immunosuppression. Those exclusions could be critical when applying this evidence. If we start prescribing steroids in a broader population, we could see the harms outnumber the benefits.
Conversely, these studies also excluded patients with other indications for steroids, such as asthma or COPD, so these results should not influence prescribing in the presence of those conditions.
Although not actually exclusions in these studies, steroids have been studied independently for ARDS and septic shock. Those studied have been discussed extensively elsewhere. The evidence isn’t perfect, but it is far better than the evidence for steroids in pneumonia. Obviously, among the sickest patients, there is significant overlap between these conditions. If you think steroids are a good idea for ARDS or septic shock, you should use them whether or not the underlying cause is pneumonia.
Publication bias?
The Cochrane review states that there is no small study effect based on their funnel plot, but seeing as all the studies are small, I think it is very hard to analyze the funnel. Considering that this area of research is predominated by small trials, and a number were not registered, it seems likely that there are at least some unpublished trials. A small trial with a negative result is unlikely to be received with excitement by any big journals, and researchers often give up after a few rejections. Although it would be no one’s fault in particular, if a number of small negative trials had been systematically eliminated from the corpus, the results of the meta-analyses could easily be wrong.
Different Steroids
As far as science goes, I am a much bigger fan of clinical trials than physiologic reasoning, but the different steroids can have big differences in their physiologic effects. These studies all use different doses, types, and routes of steroid administration. If the specific steroid matters, that would introduce significant clinical heterogeneity, making the combination of these trials in a meta-analysis potentially inappropriate or misleading. This might matter more when treating COVID, when there is good evidence for dexamethasone, but much less strong evidence for any other steroids.
Drug interactions
You might think that a section on drug interactions would talk about the potential harms of steroids, and it could, but a number of experts have suggested that drug interactions could be a major confounder in this data. Steroids are eliminated through the cytochrome P450 pathways and many antibiotics alter the function of these pathways. Perhaps more importantly, some antibiotics – such as azithromycin or moxifloxacin – seem to have at least a degree of intrinsic anti-inflammatory activity. Therefore, whether or not steroids work in a trial might be highly dependent on the antibiotic regimen they are being combined with. If azithromycin is already providing adequate anti-inflammatory effects, steroids may not provide any additional benefit, even if there is a potential benefit when they are combined with amoxicillin. This is all very theoretical, but provides a sense of the complexities that underlie this data. (Flendman 2016)
Subgroups?
The trials have all been quite small so far, so I would not put any faith in subgroups. However, there are almost always some patients at higher risk from harms from certain interventions, and there may also be subgroups with greater chance of benefit. It seems relatively clear that sicker patients, with significant immune responses, will be the ones who might benefit from steroids. One systematic review suggested that older patients don’t benefit from steroids, which might make sense considering a less robust immune response with age. (Huang 2019) I think these subgroups should play a role in guiding future research, but probably don’t have much clinical importance at this time.
Conclusion
Overall, the available evidence is incredibly weak. Although the Cochrane review suggests a mortality benefit, after reading the studies that comprise that review, I have very little faith in the conclusion. I do not think there is any strong reason to be using steroids for community acquired pneumonia at this time. There also isn’t strong evidence against steroids. However, steroids have well documented harms, so without good evidence, they should probably be avoided.
Other FOAMed
SGEM#216: Pump It Up – Corticosteroids For Patients With Pneumonia Admitted To Hospital
PulmCrit: Evidence-based treatment for severe community-acquired pneumonia
Two NNT reviews on the topic: Corticosteroids for Treating Pneumonia and Corticosteroids for Community-Acquired Pneumonia
References
Ambroggio L, Test M, Metlay JP, et al. Adjunct Systemic Corticosteroid Therapy in Children With Community-Acquired Pneumonia in the Outpatient Setting. J Pediatric Infect Dis Soc. 2015;4(1):21-27. doi:10.1093/jpids/piu017 PMID: 26407353
Blum CA, Nigro N, Briel M, et al. Adjunct prednisone therapy for patients with community-acquired pneumonia: a multicentre, double-blind, randomised, placebo-controlled trial. Lancet. 2015;385(9977):1511-1518. doi:10.1016/S0140-6736(14)62447-8
Chalmers JD. Corticosteroids for community-acquired pneumonia: a critical view of the evidence. Eur Respir J. 2016;48(4):984-986. doi:10.1183/13993003.01329-2016 PMID: 27694410
Chen Y, Li K, Pu H, Wu T. Corticosteroids for pneumonia. Cochrane Database Syst Rev. 2011;(3):CD007720. Published 2011 Mar 16. doi:10.1002/14651858.CD007720.pub2 PMID: 21412908
Confalonieri M, Urbino R, Potena A, et al. Hydrocortisone infusion for severe community-acquired pneumonia: a preliminary randomized study. Am J Respir Crit Care Med. 2005;171(3):242-248. doi:10.1164/rccm.200406-808OC PMID: 15557131
Feldman C, Anderson R. Corticosteroids in the adjunctive therapy of community-acquired pneumonia: an appraisal of recent meta-analyses of clinical trials. J Thorac Dis. 2016 Mar;8(3):E162-71. doi: 10.21037/jtd.2016.02.43. PMID: 27076965
Gottlieb M, Seagraves T, Gore SR. Do Corticosteroids Benefit Patients With Influenza Pneumonia?. Ann Emerg Med. 2020;75(1):100-101. doi:10.1016/j.annemergmed.2019.06.021 PMID: 31350095
Huang J, Guo J, Li H, Huang W, Zhang T. Efficacy and safety of adjunctive corticosteroids therapy for patients with severe community-acquired pneumonia: A systematic review and meta-analysis. Medicine (Baltimore). 2019;98(13):e14636. doi:10.1097/MD.0000000000014636 PMID: 30921179
Lloyd M, Karahalios A, Janus E, et al. Effectiveness of a Bundled Intervention Including Adjunctive Corticosteroids on Outcomes of Hospitalized Patients With Community-Acquired Pneumonia: A Stepped-Wedge Randomized Clinical Trial [published online ahead of print, 2019 Jul 8]. JAMA Intern Med. 2019;179(8):1052-1060. doi:10.1001/jamainternmed.2019.1438 PMID: 31282921
Meijvis SC, Hardeman H, Remmelts HH, et al. Dexamethasone and length of hospital stay in patients with community-acquired pneumonia: a randomised, double-blind, placebo-controlled trial. Lancet. 2011;377(9782):2023-2030. doi:10.1016/S0140-6736(11)60607-7 PMID: 21636122
Metlay JP, Waterer GW, Long AC, et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;200(7):e45-e67. doi:10.1164/rccm.201908-1581ST PMID: 31573350
Nafae RM, Ragab MI, Amany FM, Rashed SB. Adjuvant role of corticosteroids in the treatment of community‐acquired pneumonia. Egyptian Journal of Chest Diseases and Tuberculosis 2013;62(3):439–45. [Google Scholar]
Ni YN, Chen G, Sun J, Liang BM, Liang ZA. The effect of corticosteroids on mortality of patients with influenza pneumonia: a systematic review and meta-analysis [published correction appears in Crit Care. 2020 Jun 23;24(1):376]. Crit Care. 2019;23(1):99. Published 2019 Mar 27. doi:10.1186/s13054-019-2395-8 PMID: 30917856
Stern A, Skalsky K, Avni T, Carrara E, Leibovici L, Paul M. Corticosteroids for pneumonia. Cochrane Database Syst Rev. 2017;12(12):CD007720. Published 2017 Dec 13. doi:10.1002/14651858.CD007720.pub3 PMID: 29236286
Siemieniuk RA, Meade MO, Alonso-Coello P, Briel M, Evaniew N, Prasad M, Alexander PE, Fei Y, Vandvik PO, Loeb M, Guyatt GH. Corticosteroid Therapy for Patients Hospitalized With Community-Acquired Pneumonia: A Systematic Review and Meta-analysis. Ann Intern Med. 2015 Oct 6;163(7):519-28. doi: 10.7326/M15-0715. PMID: 26258555
Torres A, Sibila O, Ferrer M, et al. Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory response: a randomized clinical trial. JAMA. 2015;313(7):677-686. doi:10.1001/jama.2015.88 PMID: 25688779
Wirz SA, Blum CA, Schuetz P, et al. Pathogen- and antibiotic-specific effects of prednisone in community-acquired pneumonia. Eur Respir J. 2016;48(4):1150-1159. doi:10.1183/13993003.00474-2016 PMID: 27471201
Morgenstern, J. Steroids for community acquired pneumonia – the evidence, First10EM, January 26, 2021. Available at:
https://doi.org/10.51684/FIRS.59969

5 thoughts on “Steroids for community acquired pneumonia – the evidence”
This is a nice summary and no disagreements.
Nafae et al also has major baseline differences in renal function between placebo and steroids.
The VA Extended Steroid trial results have been available on clinicaltrials.gov for a couple of months – thoroughly negative for all endpoints.
Great Post.
https://www.nejm.org/doi/full/10.1056/NEJMoa2215145 Hydrocortisone in Severe Community-Acquired Pneumonia
Would like to know your thoughts…applies also in the ED?
Thanks
I have the paper downloaded, and it definitely looks like it will require a post and an update here
Justin
Dear Dr Mongerstern
I congrats you for your interesting blog.
You kindly cite my old paper, but you misunderstood some aspects. The plan of that preliminary RCT was to check data every 20 patients merely for patient’s safety reason. At the time our protocol was conceived (1999) there was still a great safety concern on corticosteroids treatment due to previous RCT on high-dose short-term methylprednisolone (Bone RC, et al. N Engl J Med 1987).
The advantage of a sequential trial design is greatest when the consequences of using/avoiding a treatment are serious. This situation applied to our preliminary RCT. Please note that our RCT had the improvement of oxygenation as primary end-point, and it was surprising for us too the finding of a survival advantage. Just after 18 yrs, this year our RCT’s findings has been confirmed by a larger French RCT (Dequin et al. N Engl J Med 2023). Perhaps, your blog’s conclusions should be tuned down?
Have a good one
Marco Confalonieri