In this month’s edition of the research round-up, we have everything from Bayesian analysis to CPR in outer space. With that kind of range, hopefully I have found something interesting for every reader.
ECMO!
The ARREST trial: Yannopoulos D, Bartos J, Raveendran G, Walser E, et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomised controlled trial. Lancet. 2020 Nov 12:S0140-6736(20)32338-2. PMID: 33197396
This is the first ever RCT of ECMO for out of hospital cardiac arrest, which means it is a super important trial, but our conclusions will remain somewhat limited. They included a select group of 30 patients with a good likelihood of survival from cardiac arrest, and randomized them to usual care or ECMO. The results were dramatic, with a huge difference in survival to hospital discharge (43% vs 7%) and survival to 3 to 6 months (43% vs 0%). However, there are some significant limitations in this small, open label trial. Perhaps the biggest source of bias is technological optimism. This is an open label trial and there is a lot of grey area in the decision to stop a resuscitation. The dismal outcomes in the standard care group may simply be a representation of our cynicism about cardiac arrest, even when there are markers of survivability. There were also some potentially important baseline differences between the groups, and clearly we should not be over-hauling entire health systems based on a 30 patient RCT. These results are exciting, and there are reasons to think that ECMO could be a valuable tool here, but optimism is not the same as science, and we will need to see a lot more science before this practice becomes standard.
Bottom line: The first ever RCT of ECMO in OOHCA demonstrates a massive benefit, but there are lots of sources of bias that should temper our optimism.
For the sake of your patients, don’t just do something; stand there!
Morgenstern J, Gottlieb M. Burn-Related Blisters Should Not Be Removed in the Emergency Department. Annals of Emergency Medicine. 2020; 76(6):770-771. [article]
April MD, Koyfman A, Long B. Select Burn Blisters Should not be Left Intact. Annals of Emergency Medicine. 2020; 76(6):771-773. [article]
This is the clinical controversies series from the Annals of Emergency Medicine. Although I always suggest reading and considering all sides of an argument, there is clearly only one correct answer here (hinted at by the authors’ names). I’ve covered this topic before, but it is important to know that the very limited research available has never shown benefit from burn debridement. If anything, the debridement groups are worse. Considering the pain and logistical challenges associated with debridement, we really should have evidence of benefit before putting patients through this. There are many burn specialists with strong opinions on the topic, and I think it falls to them to organize the RCT that proves their theory. For now, we should not be routinely debriding burns in the emergency department.
Bottom line: There is no evidence that debriding burn blisters helps, but it definitely hurts.
Dex: The wonder drug
Villar J, Ferrando C, Martínez D, et al. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respir Med. 2020 Mar;8(3):267-276. doi: 10.1016/S2213-2600(19)30417-5. Epub 2020 Feb 7. PMID: 32043986 ClinicalTrials.gov NCT01731795
This is a multi-center RCT based in 17 ICUs in Spain from the era before COVID. They randomized 277 patients with moderate to severe ARDS to dexamethasone (20 mg daily for 5 days then 10 mg daily for 5 days) or routine care. (This is an open-label trial.) The trial was stopped early due to low enrolment (their target was 314 patients). The main causes of ARDS were pneumonia (50%) and sepsis (25%). This is a pretty select group of patients, with only 25% of eligible patients enrolled. The mean number of ventilator free days was improved with dexamethasone (12.3 vs 7.5 days, ARR 4.8, 95% CI 2.5-7; p<0.0001). Mortality was lower with dexamethasone (21% vs 36%, ARR 15%, 95% CI 5-25%, p=0.005). This is an unblinded trial, which significantly increases the risk of bias. Death is thought of as an objective outcome, which should minimize bias, but death in a modern ICU is not as objective as we would like to think. The majority of deaths occur after a withdrawal of care. That is, we often decide when people will die in an ICU setting. If there is something about a drug that alters our prognosis, that could influence our decisions about withdrawing care, and death becomes a biased outcome. Therefore, even though we think about death as an objective outcome, there is still lots of room for bias in this open label trial. There are already debates about the role of steroids in both sepsis and pneumonia, which make up 75% of the patients here. Based on this one trial, it is impossible to distinguish whether it is ARDS that requires steroids, the underlying conditions, or neither. One interesting point: the dexamethasone group had more extubation failure (8.6% vs 5.1%). This makes me wonder whether the steroids are really helping, or whether they are just altering numbers on the monitor than make us think the patient is doing better. Of course, the mortality benefit seen here is much more important than the extubation failures, but the possibility that steroids just change numbers on a monitor without altering patient oriented outcomes is important when interpreting data from other conditions, like pneumonia.
Bottom line: Probably not a decision for me in the ED, and at least for the next little while all these patients will be getting steroids because of COVID, but I think this remains an open question with the needle leaning somewhat towards treatment.
I’m all about that Bayes
Ranji SR, Shojania KG, Trowbridge RL, Auerbach AD. Impact of reliance on CT pulmonary angiography on diagnosis of pulmonary embolism: a Bayesian analysis. J Hosp Med. 2006 Mar;1(2):81-7. doi: 10.1002/jhm.71. PMID: 17219477
This is an interesting old paper that has some important lessons for us more than a decade later – perhaps especially during the COVID-19 pandemic. It is a chart review study that looks at patients who were undergoing CTPA to rule out PE between 1998 and 2000 (so older CT scanners than we are using now). They then compare the real life outcomes in these patients with the expected outcomes based on the known sensitivity and specificity of CT for PE (and I actually think they might have been generous in their estimates, based on my reading of this literature). These are a mix of inpatients and emergency department patients, so the risk is far higher than we are used to. Broken down into Well’s low, moderate, and high risk, they had 12%, 22%, and 35% CT positivity rates respectively. As you would expect, essentially everyone with a positive CT was started on anticoagulation, and there were another 3% of patients who were treated for PE despite the initial CT being negative. Based on their calculations, about 25% of patients being treated for PE probably had false positive scans and were being given anticoagulants unnecessarily. This happened exclusively in the low and moderate risk groups. False negative scans were less common, but still occurred in about 3% of the low and moderate risk groups and as many as 10% of the high risk group.
Bottom line: This study is an excellent reminder that tests are not objective. They don’t give us perfect answers. You can’t just read the CT report. As I have discussed before, in order to interpret any test, you must know the pretest probability.
Magnesium is an analgesic?
Zolfaghari Sadrabad A, Azimi Abarghouei S, Farahmand Rad R, Salimi Y. Intravenous magnesium sulfate vs. morphine sulfate in relieving renal colic: A randomized clinical trial. Am J Emerg Med. 2020 Jul 21:S0735-6757(20)30629-X. doi: 10.1016/j.ajem.2020.07.035. PMID: 33071088 ACTRN12615001372572
I am not sure I really understand this paper. I guess there was a time that magnesium was thought to be the cure for everything, but it has clearly been replaced by ketamine in the emergency medicine literature. This paper seems to be a decade or two late. Or perhaps it marks the onset of a “retro” resurgence of interest in magnesium by these trend setting researchers. Their basic question: is magnesium as good as morphine in controlling pain from renal colic? I have no idea why you would think so, but they did an double-blind RCT that included 80 adult patients (15-55 years of age) with ultrasound confirmed renal colic, and randomized them to either 0.1 mg/kg IV morphine to a maximum of 5mg or 50 mg/kg of magnesium sulfate to a maximum of 2 grams infused over 20 minutes. Ketorolac was used as a rescue medicine, which seems entirely backwards to me. Ultimately, and to my surprise, the pain control in both groups looks pretty similar (and effective, with pain scores going from 8/10 to less than 4/10 in both groups). Morphine was slightly better at 10 minutes, but overall they look very similar. The biggest problem with this study is their choice of comparator. We know NSAIDs are the best analgesics for renal colic, so leaving ketorolac until the second line seems ridiculous. Also, the dose of morphine is inadequate; 0.1mg/kg is a fine starting dose, but 50% of the population will need more than that, and they didn’t even give that dose because of their cap at 5 mg. Magnesium has long been thought to relax smooth muscle, so there is at least a plausible physiological explanation for the effect, but this is a small study that certainly doesn’t convince me that I should be using magnesium routinely. I might be willing to try it in a carefully selected patient, perhaps because of significant allergies to our usual medications. Perhaps most importantly, this study only started after the ultrasound was performed, which significantly limits its application. Magnesium is somewhat plausible in renal colic, but won’t help at all for the many other causes of flank pain that we see, so it would be unethical to use it over proven analgesics like morphine or NSAIDs in the undifferentiated patient.
Bottom line: In this small RCT, both intravenous magnesium and a small dose of morphine decreased pain due to renal colic.
Is pulse oximetry racist??
Sjoding MW, Dickson RP, Iwashyna TJ, Gay SE, Valley TS. Racial Bias in Pulse Oximetry Measurement. N Engl J Med. 2020 Dec 17;383(25):2477-2478. doi: 10.1056/NEJMc2029240. PMID: 33326721
As was recently highlighted by questions about the COVID vaccine in pregnant women, excluding groups of people from medical research can have significant consequences. It turns out that many of our medical devices, such as pulse oximeters, were developed in populations lacking racial diversity, and have not been fully validated outside of those populations. This paper discusses two retrospective cohort studies looking at almost 50,000 oxygen saturation readings from almost 10,000 adult inpatients either receiving supplemental oxygen (in the initial cohort) or in one of 178 ICUs (in the second cohort). A pulse oximetry reading was compared to a gold standard arterial blood gas drawn within 10 minutes. Among patients with a pulse ox reading of 92-96%, a surprising number had arterial blood gas oxygen saturations below 88%. The number was much higher among Black patients than White. In the initial smaller cohort, the rate was 3.5% among White patients and 11.7% among Black patients. In the larger multi-centre cohort, the rate was 6.2% among White patients and 17% among Black patients. There isn’t any comment on the reliability of the pulse ox waveform, and I think we all know that these devices can be unreliable. However, if this is referring to patients with a reliable tracing, I am surprised at how inaccurate the numbers were, although maybe I shouldn’t be, as it is somewhat incredible that we even are able to measure the oxygen through the skin with just a light. I think this is an important lesson to learn for all our patients. Don’t be overly reliant on the pulse ox. There is also a very important general rule about bias in medicine. Whether it is women or non-White individuals, there are many ways that subtle research biases can have pretty profound clinical impacts. You can hear more from Laurn Westafer on the FOAMcast podcast. PulmCrit also wrote about this, and apparently we have known about this issue for more than a decade.
Bottom line: Medical research needs to be far more inclusive, and for the meantime we need to be cautious in our interpretation of pulse oximetry.
Latent safety threats in trauma
Petrosoniak A, Fan M, Hicks CM, White K, McGowan M, Campbell D, Trbovich P. Trauma Resuscitation Using in situ Simulation Team Training (TRUST) study: latent safety threat evaluation using framework analysis and video review. BMJ Qual Saf. 2020 Oct 23:bmjqs-2020-011363. doi: 10.1136/bmjqs-2020-011363 PMID: 33097610
This is a tricky one to capture in a single paragraph. Luckily, there is a full write up that you can find here. They taped complex trauma in situ simulation sessions over the course of a year, and reviewed the recordings to identify latent safety threats. They identified a total of 843 threats over 12 cases, or a total of 70 per case. 60% of these were considered critical. This is a single center simulation study, but I think everyone will recognize the issues that they identified. It is worth reviewing their findings and reflecting on the ways in which your own resuscitation room / teams can be improved. For example, they note that the vital signs monitor was not visible from everywhere in the room. (This has been a problem for intubation in every emergency department I have worked in.) They solved this by adding 2 extra monitors so that every team member can be aware of the vital signs. They also note that finding equipment for critical procedures was difficult, and not every team member knew where everything was. To solve this, rather than storing equipment individually, they made packs – so that the scalpel, bougie, and endotracheal tube required for a cricothyrotomy would be all in a single bag rather than stored in 3 different locations. There are a number of other lessons here, and I really think that every resuscitationist can learn a lot from reviewing this paper. I imagine you will also hear about these issues from Andrew Petrosoniak and Chris Hicks at conferences in the future, and I am excited to hear them expand on these findings.
Making night shifts better
Wallace PJ, Haber JJ. Top 10 evidence-based countermeasures for night shift workers. Emerg Med J. 2020 Sep;37(9):562-564. doi: 10.1136/emermed-2019-209134. PMID: 32332056
This paper got it’s own blog post, but provides a nice practical, evidence based summary of things we can do to improve night shifts. Their 10 big recommendations were:
- Schedule for circadian rhythm
- Nap prior to your night shift
- Maximize bright light on shift
- Take a nap if you can
- Drink caffeinated beverages early in the shift
- Avoid large meals
- Minimize light on the commute home
- Consider melatonin
- Sleep in a dark environment
- Sleep in a cool environment
You can read more here, or just take the time to read the paper, because this is information we all need.
The reverse vagal maneuver
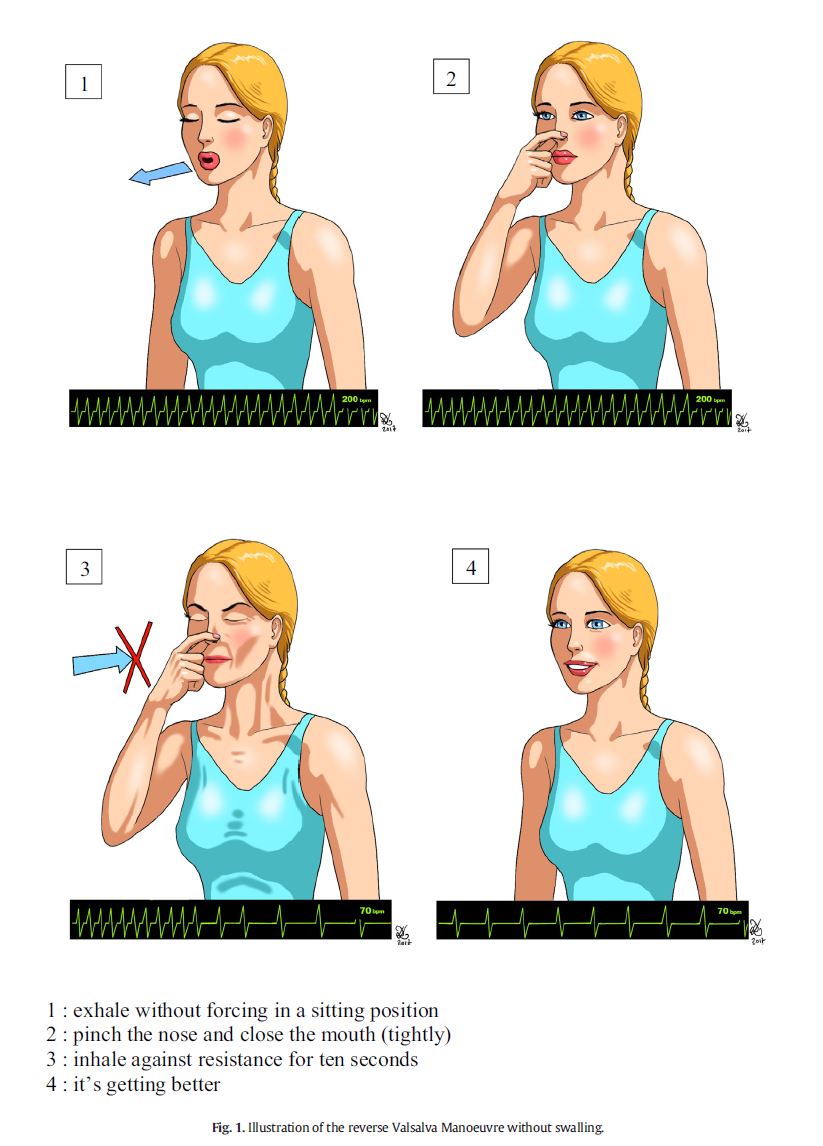
Gaudart P, Cazes N, Simon K, Larger D, Deharo JC. The reverse vagal manoeuvre: A new tool for treatment of supraventricular tachycardia? Am J Emerg Med. 2020 Dec 26;41:66-69. doi: 10.1016/j.ajem.2020.12.061. PMID: 33387931
This is just a case series of 11 patients describing a new vagal maneuver. It worked in 10 of the 11 cases, but given the selection bias inherent in case reports I wouldn’t be too focused on the numbers. I include the paper just because the maneuver seems interesting, easier to perform than other vagal maneuvers, and relatively harm free, so it might be worth trying clinically. Basically, with the patient sitting upright, you have them exhale normally, pinch their nose and close their mouth tightly, and then try to inhale against that closed airway for 10 seconds.
CPR in space
Hinkelbein J, Kerkhoff S, Adler C, et al. Cardiopulmonary resuscitation (CPR) during spaceflight – a guideline for CPR in microgravity from the German Society of Aerospace Medicine (DGLRM) and the European Society of Aerospace Medicine Space Medicine Group (ESAM-SMG). Scand J Trauma Resusc Emerg Med. 2020 Nov 2;28(1):108. doi: 10.1186/s13049-020-00793-y. PMID: 33138865
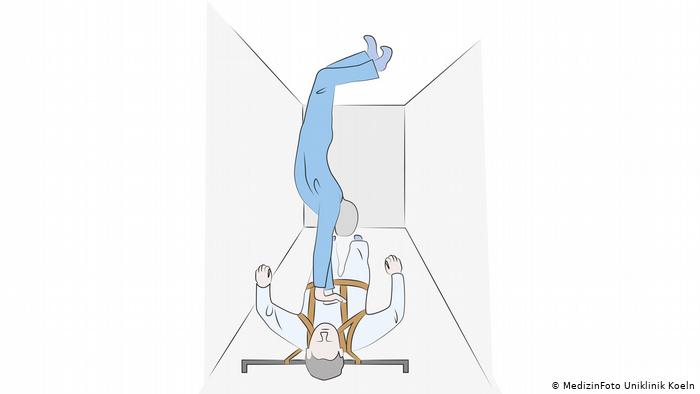
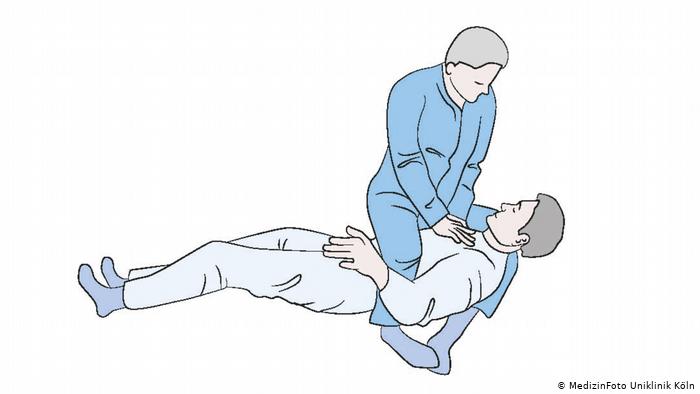
Usually I just pick articles that are interesting to me, but occasionally a paper will come out with such broad reaching implications that I am simply forced to include it. This paper provides us with guidelines on CPR in outer space. They tell us about a few different options for performing CPR in microgravity – because remember, if you push on the patient’s chest, you will just go floating off in the opposite direction. You could use straps, but that sounds somewhat boring. I like the “headstand technique”, where you push the patient against the ground (or any wall – they are all the same), put your feet against the opposite wall, and your hands on their chest, so it looks like you are doing a handstand on their chest. I think some athletic individual should try this in a normal hospital setting and report back to me.
You could also use the “reverse bear hug method”, which sort of looks like the Heimlich maneuver, but your hands are higher. Their recommended approach is the “Evetts-Russomano” method, which just looks bizarre, but I guess you have to do what you have to do.
Seriously, though, I wonder about reversible causes and ongoing care after ROSC in outer space. Considering how expensive it is to get every piece of equipment out to space, is an AED worth it? Electrocution is immediately reversible, so that might make an AED worthwhile. (The repairs I saw during Apollo 13 were pretty janky and make me think electrocution is a real possibility, although I think the total available voltage on the space station is pretty low). Considering the length of travel in confined spaces, astronauts probably have PE risk factors, which could be reversible if they stock lytics. Realistically, though, if someone has a cardiac arrest in outer space, what are their chances of survival?
Cheesy Joke of the Month
Yesterday I was washing the car with my son.
He said: Dad, could you please just use a sponge?
You can find more research round-ups and critical appraisals here
Morgenstern, J. Research Round-up (January 2021), First10EM, January 25, 2021. Available at:
https://doi.org/10.51684/FIRS.61045