
Morgenstern, J. Research Roundup (November 2021), First10EM, November 29, 2021. Available at:
https://doi.org/10.51684/FIRS.123367
As anticipated, my “monthly” summaries have become even less frequent, as I discovered that there are a few things in life even more enjoyable than reading the medical literature. I won’t apologize for choosing my 9 month old over evidence based medicine, but I will continue to put out these summaries whenever I can.
Ketamine for agitation – some RCTs
Lin J, Figuerado Y, Montgomery A, Lee J, Cannis M, Norton VC, Calvo R, Sikand H. Efficacy of ketamine for initial control of acute agitation in the emergency department: A randomized study. Am J Emerg Med. 2021 Jun;44:306-311. doi: 10.1016/j.ajem.2020.04.013. PMID: 32340820
Barbic D, Andolfatto G, Grunau B, Scheuermeyer FX, Macewan B, Qian H, Wong H, Barbic SP, Honer WG. Rapid Agitation Control With Ketamine in the Emergency Department: A Blinded, Randomized Controlled Trial. Ann Emerg Med. 2021 Aug 2:S0196-0644(21)00433-9. doi: 10.1016/j.annemergmed.2021.05.023 PMID: 34353650
I am going to group these two papers together, and just provide a very brief summary here. If you want more details, you can read the full blog post. These two RCTs are remarkably similar. They both randomized about 80 patients to either ketamine, or a combination of haloperidol and a benzodiazepine. They are not perfect trials (for example neither is completely blinded). However, the results are believable. Ketamine will provide slightly faster sedation (about 10-20 minutes depending on your dosing of the haloperidol and benzo), but probably also has more side effects. The biggest problem with these trials is that they are small; much too small to tell us about the side effects we really care about. Although there was probably more apnea and hypoxia with ketamine in these trials, these were actually relatively minor, as patients didn’t end up in the ICU. I am probably willing to accept a brief apnea spell or transient hypoxia for more rapid control of severely agitated patients, but we will need much bigger trials to see if one of these options is actually safer. It is weird to me that neither paper reports on injuries to patients or staff, as ‘safety’ is generally the reason we are rapidly controlling these patients. Whichever option you choose, if the patient is sick enough to consider ketamine, they probably need to be placed in a resuscitation room with one to one nursing and close monitoring.
Bottom line: There is now some RCT evidence to support the use of ketamine in severe agitation, but the data is far from perfect. I tend to follow Reuben Strayer’s advice: if the patient is so agitated that I would consider intubating them just for control, ketamine is a good option. Otherwise, I tend to stick with other options (and continue to hope that they will bring droperidol back to Canada.)
Racial Bias in Pulse Oximetry – part 2
Valbuena VSM, Barbaro RP, Claar D, et al. Racial Bias in Pulse Oximetry Measurement Among Patients About to Undergo ECMO in 2019-2020, A Retrospective Cohort Study. Chest. 2021 Sep 27:S0012-3692(21)04065-4. doi: 10.1016/j.chest.2021.09.025. PMID: 34592317
I first covered the topic of racial bias in pulse oximetry in January 2021. Apparently we have ‘known about’ this issue for a long time, but I certainly didn’t. I will probably do a deeper dive into the literature, but in case you thought that prior paper was a one-off, here is another study showing the same. It is registry data looking at adult patients with ARDS or COVID-19 being placed on ECMO. PulseOx values were compared to arterial blood gas values within 6 hours of starting on ECMO. (They tried to get measurements as close as possible, but the changes that might be expected in such unstable patients are the biggest weakness of this study.) We also don’t have any information on the type of pulse oximeter being used. From 3569 ECMO runs, they include 1562 that had available pairs of pulse ox and ABG measurements, and only 372 with adequate racial information. The mean difference between SpO2 and SaO2 was 0.6% overall, 0.3% in White patients, and 1.7% in Black patients. Among White patients, 10% of patients with an SpO2 between 92% and 96% actually had an SaO2 less than 88%. In Black patients, this number was 22% (p=0.03). Looking at patients with an SpO2 above 96%, 7% of White patients and 21% of Black patients had an SaO2 less than 88%. The numbers are relatively small, so confidence intervals are wide. (Numbers in Asian and Hispanic patients were not significantly different from White patients.) There are a number of issues with this data. Sociologic race labels are unlikely to correlate perfectly with skin tone, which is thought to be the underlying mechanism. However, the conclusions seem correct, and should increase caution in the interpretation of pulse ox values, especially among patients with darker skin.
Bottom line: The pulse oximeter is nowhere near as accurate as we would like. Occult hypoxemia occurs in a significant proportion of all patients sick enough to undergo ECMO, and it is much higher among Black patients. This is a good reminder never to let clinical decisions hinge on single data points.
Industry-funded medical education is always promotion
Fugh-Berman A. Industry-funded medical education is always promotion-an essay by Adriane Fugh-Berman. BMJ. 2021 Jun 4;373:n1273. doi: 10.1136/bmj.n1273. PMID: 34088736
The title sort of says it all. Despite heaps of evidence that industry funding of CME is really just biased advertising, we continue to allow it to happen. This essay reviews some of the evidence that tells us that industry sponsored CME is biased and has significant impacts on prescribing choice. Most importantly, doctors are unable to detect this bias, and generally do not believe industry sponsored CME is biased. Bias in CME is often very subtle. Drug companies employ experts in marketing and psychology, which means that our attempts to mitigate bias by having presenters declare conflicts of interest are generally ineffective. Industry spent $750 million on funded CME in 2018 in the United States alone – and these companies are not doing so altruistically. They know they are getting a return on their investment. Despite the massive problems with funded CME, 80% of professional organizations in Canada still accept industry funded CME. Ultimately, the only real solution is to call a spade a spade, and stop allowing these industry infomercials dressed up as CME sessions to exist. They need to be completely banned, because you are being sold poor care, and you don’t even realize it.
Twelve tips for applying the science of learning
Gooding HC, Mann K, Armstrong E. Twelve tips for applying the science of learning to health professions education. Med Teach. 2017 Jan;39(1):26-31. doi: 10.1080/0142159X.2016.1231913. Epub 2016 Sep 25. PMID: 27665669
Paper number 2 in this ad hoc medical education section is a great summary of some key lessons from the science of learning, which will be valuable whether you are an educator, or just on the lifelong journey of education required by this profession. (Some of these points were covered in my post on the book “Making it Stick”, but as you might have learned from that post, spaced repetition is essential.) Their 12 tips are:
- Reduce extraneous load whenever possible (extraneous load is cognitive work not directly related to the complexity of the information itself, such as complicated and hard to interpret slides)
- Help learners manage intrinsic load and assist learners with germane load (germane load is the cognitive work of organizing new information into schemas)
- Create opportunities for retrieval practice appropriate for the content to be learned
- Space retrieval practice over time and interleave content
- Explicitly prepare learners to transfer knowledge to new settings
- Engage learners in deliberate practice
- Help learners to create learning-oriented goals
- Teach learners to recognize their emotional state and its role in their learning
- Create learning spaces that are psychologically safe
- Attend to the social nature of learning
- Create authentic experiences for workplace learning
- Promote metacognition in our learners and ourselves
A lot of these concepts are somewhat foreign in medical education. I expect there will be something new on this list for everyone. The paper is easy to read. If any of this sounds interesting to you, this paper will be a great springboard into the science of learning. (The paper was also covered on REBELEM’s podcast.)
Tylenol in pregnancy
Bauer AZ, Swan SH, Kriebel D, Liew Z, Taylor HS, Bornehag CG, Andrade AM, Olsen J, Jensen RH, Mitchell RT, Skakkebaek NE, Jégou B, Kristensen DM. Paracetamol use during pregnancy – a call for precautionary action. Nat Rev Endocrinol. 2021 Sep 23. doi: 10.1038/s41574-021-00553-7 PMID: 34556849
This paper is likely to get a lot of attention. It has already been sent to me multiple times. The attention is understandable, as the paper essentially says that we need to stop using acetaminophen (or paracetamol if you are reading in other parts of the world) in pregnant women. That is problematic, as acetaminophen is really the only analgesic we are currently comfortable using in pregnancy. I have been following this research for some time, and none of the individual studies were very convincing. (Confounders are incredibly common in this kind of research.) However, the studies have accumulated, and 26 of the 29 observational cohorts they identified found a positive correlation between acetaminophen use and neurodevelopmental issues. (The tie to urologic issues they discuss is less convincing, being found in only half of studies.) Consistency doesn’t necessarily exclude bias from these studies, though. Neurodevelopmental diagnoses (such as ADHD) are incredibly common, as is acetaminophen use, and when you add the potential for recall bias, it would not be surprising if the association was entirely fictional. Further complicating matters is the fact that we don’t really understand acetaminophen’s mechanism of action, which means that predicting fetal toxicology is very difficult. These authors admit that much more research is needed, but while awaiting that research, they suggest that all women be counselled prior to or early in pregnancy that:
- Pregnant women should forego APAP use unless medically indicated.
- Pregnant women should consult with their physician or pharmacist if they are uncertain whether use is indicated and before using on a long- term basis.
- Pregnant women should minimize risk by using the lowest effective APAP dose for the shortest possible time.
This is good guidance for any medication, but it doesn’t actually help us at all clinically. In large part, the impact and appropriateness of this guidance will hinge on how people interpret “medically indicated”. Although the issues raised are important, this document completely fails to provide any clinically usable information. If there is a true association between acetaminophen use and ADHD, what is the magnitude of the risk? Considering that the majority of pregnant women are currently using acetaminophen, the absolute risk must be relatively small. Without this information, or at least an estimation, it is essentially impossible to act on this information. Another major problem with this guidance (and it is similar to a lot of guidance in pregnancy) is that it fails to offer any alternatives. When treating a pregnant woman with significant pain, what exactly am I supposed to do? Are NSAIDs safer? Is morphine? In failing to provide any comparative data, this guidance cannot possibly improve clinical care; it can only serve to increase anxiety among pregnant women and physicians alike.
Bottom line: There is enough evidence to suggest that acetaminophen use in pregnancy may be associated with neurodevelopmental issues such as ADHD. However, we also have enough experience with the agent to know that the magnitude of the risk must be small, and acetaminophen is a valuable drug in pregnancy, especially when other analgesics are contra-indicated. A massive amount of uncertainty remains. Their recommendations make sense to me, and apply to all medications in pregnancy: make sure its use is actually warranted, and use the lowest dose for the shortest possible time. But I am not sure that helps us a lot when we are seeing pregnant women with painful conditions in the emergency department.
Another study that will chill your enthusiasm for hypothermia
Le May M, Osborne C, Russo J, et al. Effect of Moderate vs Mild Therapeutic Hypothermia on Mortality and Neurologic Outcomes in Comatose Survivors of Out-of-Hospital Cardiac Arrest: The CAPITAL CHILL Randomized Clinical Trial. JAMA. 2021 Oct 19;326(15):1494-1503. doi: 10.1001/jama.2021.15703. PMID: 34665203
This is a well done, partially blinded RCT comparing a target of 31°C to 34°C in comatose survivors of out of hospital cardiac arrest. We might have been more interested in this data a few years ago, before the publication of TTM and TTM2, when people were still pretty convinced that hypothermia worked. Now, it seems like this might be a trial that simply compares placebo to placebo, which is somewhat ridiculous. With that in mind, it is not surprising that the trial shows no benefit. The primary outcome was a combination of death and poor neurologic outcomes, and it occurred in 48.4% of the 31°C group and 45.4% of the 34°C group (absolute difference 3%, 95% CI -7.2% to 13.2%, p=0.56). All cause mortality was 43.5% vs 41.0%. The only significant difference among secondary outcomes was a longer ICU length of stay in the 31°C group (10 days versus 7 days, p=0.004). Really, the lower temperature looks worse across the board, and although not close to statistically significant, the 3% absolute difference between the groups would be clinically significant if real.
Bottom line: Colder is definitely not better, but that probably doesn’t matter as most people have shifted away from ‘therapeutic’ hypothermia altogether, in favour of controlled normothermia.
More details can be found here
COVID is depression?
Reis G, Dos Santos Moreira-Silva EA, Silva DCM, et al. Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial. Lancet Glob Health. 2021 Oct 27:S2214-109X(21)00448-4. doi: 10.1016/S2214-109X(21)00448-4. PMID: 34717820
This paper gets its own blog post, but only because a quick read of the abstract probably leaves you with a different conclusion than a thorough read of the paper. It is an RCT of 1497 adult outpatients with COVID and at least 1 high risk feature, randomized to either fluvoxamine 100 mg PO BID or placebo. Although they found a statistically significant decrease in their primary outcome, the outcome they used is incredibly flawed. They looked at hospitalization or an ED visit of 6 hours, which are clearly not the same thing. To make matters worse, they only counted visits that were ‘for COVID’ which would automatically exclude any adverse events from the SSRI, and therefore biases the study from the outset. This primary outcome was better with fluvoxamine (16% versus 11%), but hospitalization was not statistically different (10% vs 13%), and neither was mortality (2% vs 3%). Considering the number of different agents we have tested against COVID, we should expect some trials to be positive by chance alone, and this feels like that kind of trial. It is also worth noting that these were unvaccinated patients. Outcomes will be much better in a vaccinated population, and so the absolute benefit will be much smaller.
Bottom line: Although this study is reported as positive, I think it is unlikely that fluvoxamine actually helps patients. Personally, I would not prescribe it or take it unless I see a high quality follow up study looking at outcomes that actually matter.
A malaria vaccine!
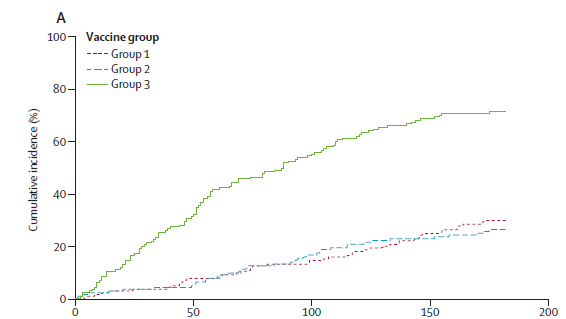
Datoo MS, Natama MH, Somé A, et al. Efficacy of a low-dose candidate malaria vaccine, R21 in adjuvant Matrix-M, with seasonal administration to children in Burkina Faso: a randomised controlled trial. Lancet. 2021 May 15;397(10287):1809-1818. doi: 10.1016/S0140-6736(21)00943-0. PMID: 33964223
Most readers don’t have to think about malaria on a day to day basis, but it remains one of the leading causes of death worldwide. My personal experience with mosquitos means that I favour efforts to completely eradicate the little bastards, but a vaccine might be a more ecologically reasonable approach. This is a double blind phase 2 RCT that included 450 pediatric patients 5-17 months old and randomized them to the R21 malaria vaccine with 1 of 2 different adjuvant doses, or to a rabies vaccine as a control group. The vaccine was tremendously effective, with an absolute risk reduction unlike anything we talk about in these research roundups. 71% of the control group was diagnosed with malaria in the 6 months after vaccination, as compared to 26% and 29% of the vaccine groups (p<0.0001). Adverse events were as you would expect: some fever, irritability, and local reactions. Obviously, this paper is not going to change practice for readers in North America, Europe, or Australia, but I find the results incredibly exciting and illuminating. I am very aware of the problem that malaria poses in the world, but I was still naively surprised by the 70% rate of infection over 6 months in the control group. (And this is despite almost 90% of households using insecticide treated mosquito nets, 15% spraying for mosquitos, and 70% receiving seasonal malaria prophylaxis.) Perhaps the biggest take home message from this paper is that those of us in high income countries need to take off our blinders as to how huge a problem malaria remains around the world.
Bottom line: There is not a licensed malaria vaccine to date, but this RCT gives us hope that that will change in the near future.
A can’t miss diagnosis: restless anal syndrome
Nakamura I, Itoi T, Inoue T. Case report of restless anal syndrome as restless legs syndrome variant after COVID-19. BMC Infect Dis. 2021 Sep 23;21(1):993. doi: 10.1186/s12879-021-06683-7. PMID: 34556029
OK, restless leg syndrome is not usually considered an essential emergency medicine diagnosis, so it may not be all that important for us to know about a variant called “restless anal syndrome”. (In fact, this article is not written well enough for me to determine whether this is a true variant, or just something they made up to get published.) However, you certainly wouldn’t want to be the only person at the dinner party who hadn’t heard of this. Basically, this is a case report of a 77 year old who recovered from mild COVID and later developed “restless, deep anal discomfort, approximately 10 cm from the perineal region”. (Don’t ask me how they determined that it was 10 cm from the perineal region, or in what direction they are referring. However, unless this patient has truly bizarre anatomy, I don’t think you could possibly still be at the anus if you were 10 cm from the perineum. Maybe they really meant restless rectal syndrome?) He had a workup that was pretty normal, and because the symptoms got better with exercise and distraction, but worse with rest, they decided this was restless anal syndrome. They treated him with daily clonazepam, which probably won’t make the geriatricians or the authors of the BEERS list too happy. Ultimately, I don’t think this article provides any value to anyone, and I am probably only including it because I giggle every time I read “restless anal syndrome”. The article mostly represents how easy it is to get anything published these days, as long as you slap the word “COVID” on it, although, considering that these symptoms developed weeks after his recovery, I am not even sure that this had anything to do with COVID.
Bottom line: I am still a school-aged boy at heart. You should have stopped reading before you got to this article.
Cheesy Joke of the Month
Someone glued my deck of cards together…
I don’t know how to deal with it



6 thoughts on “Research Roundup (November 2021)”
Here in the American south, droperidol has made a comeback in our ER. It can work like a miracle for cannabis induced hyperemesis (1.25mg IV) but I (ER nurse) have been disappointed by how quickly the unkind use of this high-risk medication has returned to practice, as if we have forgotten why it was removed from our formulary in the first place. In the past 3 weeks I had two patients who experienced adverse reactions with the inappropriate use of droperidol. One 35 y/o woman was given 1.25mg IVP for a headache and experienced significant psychological distress. The other was a 19 y/o woman being treated for viral syndrome + severe underlying anxiety who had a dystonic reaction to 2.5mg IVP that completely freaked out her mother. Droperidol is Russian roulette with two bullets in the chamber. This with safe and effective alternatives available such as ziprasidone for hyperemesis or psychosis and metoclopramide for headache.
Many years ago I had an ER physician say to me, “Whatever their complaint, droperidol stops the complaining.” This is the asshole attitude that got droperidol black-boxed in the first place. Maybe my experience is not typical but if I had my druthers we would put droperidol and prochlorperazine in a rocket and blast it into the sun.
Love this blog I never miss it! Thank-you for your efforts.
Thanks for the comment I have lots of experience with droperidol, working in both New Zealand and Australia. Can’t say I have your experience. Sure, there are the normal side effects of anti-psychotics, but no more common than with haloperidol (in fact, I think less). And the side effects are easily treatable, especially if you warn the patient in advance. Indication creep can be an issue, and mistakes among those inexperienced with it’s use will occur. However, overall I think it is a better option than what we are currently using in many clinical scenarios.
Right now I am using haloperidol in any scenario I would usually use droperidol, and I think it is clearly a worse alternative.
Right but I am not comparing droperidol to haldol. Perhaps you are constrained by cost-saving measures at your place of practice? There are new safe and effective drugs available. For acute psychosis, ziprasidone or olanzapine may take a few minutes longer to kick in than haldol but it is very effective (I compare it to rebooting a computer) and it allows for significantly faster disposition times compered to haldol (a blunt instrument by any measure). Not to mention patient experience.
Hi Justin, thanks for your excellent work. Very informative for my practice.
With regards to acetaminophen in general I wonder if you have done any deep dives into it! I know we use it everywhere but wonder if the evidence for it holds in treating many things we use it for. If you’ve already done a deep dive my apologies I’ll look again, but was wondering if you had any thoughts on the efficacy of acetaminophen/paracetamol and what you do in your practice?
https://uk.cochrane.org/news/paracetamol-widely-used-and-largely-ineffective
I haven’t done a complete review. Have covered individual papers here and there. Lots show no benefit, but outcomes often questionable (I don’t expect acetaminophen to help disability at 3 weeks, but pain in an hour is likely somewhat better).
We talk about it a bit in this EM Cases: https://emergencymedicinecases.com/drugs-that-work-analgesics/