
I have ranted previously about my concern that sucrose, despite its widespread use in pediatrics, is not actually a pain medication. I repeated that rant this week as part of the SMACCmini pre-conference day. However, it is always frustrating when people point out problems without offering solutions. This blog post outlines essential pediatric analgesic strategies that all emergency clinicians should know.
Why is this important?
This section probably doesn’t need to exist. If children are in pain, it is important to treat that pain. I don’t think I need much more of an argument than that.
However, there is some weak evidence that pain control in infants is even more important than in adults. Because of a relative lack of inhibitory neurotransmitters, larger receptive fields, and an increased concentration of substance P receptors, it is theorized that infants may feel pain more severely than older people. (Matthew 2003) Furthermore, there are hints that pain in infants can result in altered pain sensitivity and neuroanatomic and behavioural changes that might be long lasting. (AAP 2007; Taddio 2002; Matthew 2003) Prolonged or repeated pain can result in hyperalgesia and allodynia. (AAP 2007)
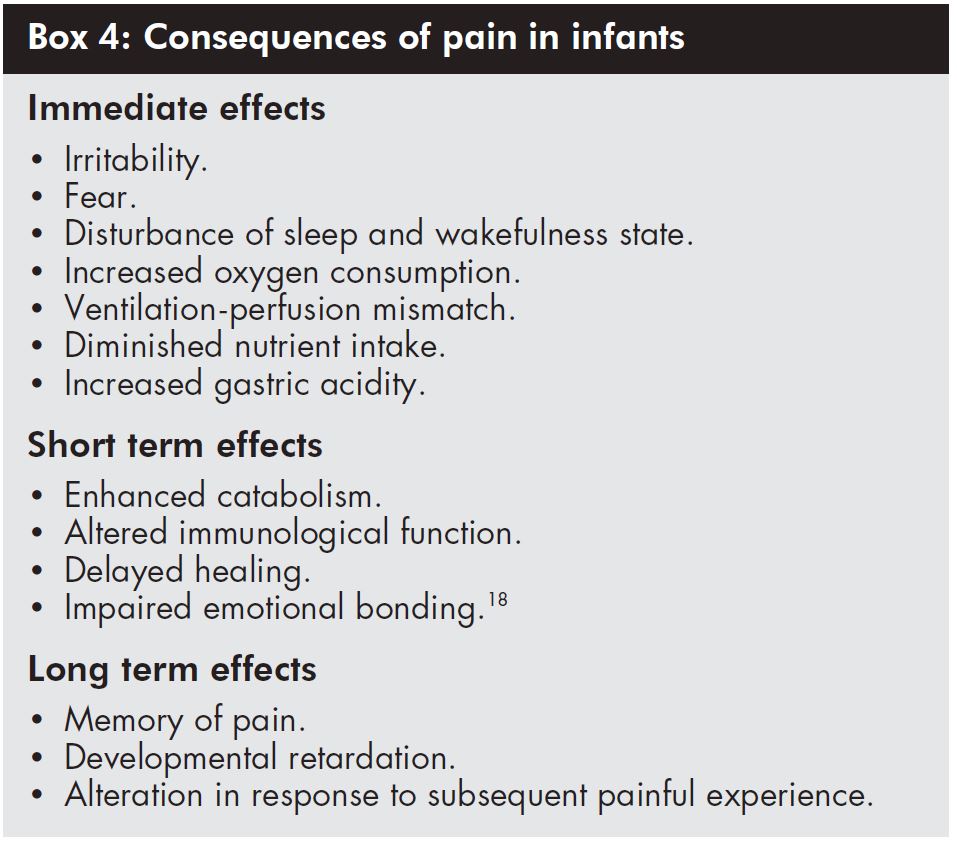
However, the science is a little complex, murky, and frequently reliant on extrapolation from animal studies. I considered doing a deep dive into the literature, but then I realized I was being ridiculous. It doesn’t really matter what the long term consequences are. We should be controlling infants’ pain because they are in pain, and we are doctors, and what else would you do? So forget about the long term consequences, and just imagine what you would want if it was your baby in pain.
Evidence of oligoanalgesia
Children need pain control, but it doesn’t seem like we are all that good at providing it. (AAP 2007) In one observational study of neonates in an NICU setting, the average neonate underwent 75 painful procedures during their NICU stay, or about 10 per day. 80% of those procedures were done without any analgesia. (Carbajal 2008) In another survey of NICU practices, only 58% of NICUs used routine analgesia for LPs, 50% for venipuncture, and 68% for chest tube insertion. (Lago 2005) Another look at NICU patients found an average of 14 painful procedures a day, but only 35% of infants were given analgesics on any given day, and 40% never received an analgesic while in the NICU. (Simons 2003)
We are just as bad in the emergency department. In a chart review of patients with long bone fractures, although 73% of adults received analgesia in the ED, only 53% of children did. (Petrack 1997) In another chart review looking at children diagnosed with appendicitis, 40% received no analgesic at all in the emergency department. (Robb 2017) This pattern of undertreatment in our youngest patients is reported widely in the literature. (Eg. Dohrenwend 2007; Alexander 2003; Friedland 1997)
Pain versus distress
Before I get too far into our analgesic options, it is important to note that pain is a relatively complex phenomenon, modulated by many factors. Pain generally starts with tissue damage with subsequent activation of neural pathways, but that biology doesn’t explain the experience of pain. The experience of pain depends a lot on your interpretation. Elite athletes often describe the lactic acid burn after a workout as pleasurable, because they anticipate its benefits. On the other hand, if you forced me to run around the block, I would perceive the exact same sensations, but experience them as pure torture. Ultimately it is distress, or the subjectively negative experience of pain that we want to treat.
Unfortunately, young children are unable to describe their sensations. We have to guess when they are in pain, and we are probably not great at it. (Singer 2002) Children who can communicate often rate their distress as higher than their pain. (Johnston 2005) In younger children, the inability to communicate means that we are forced to make assumptions, and I think that creates an ethical responsibility. Much like we would prefer to let a guilty person go free than imprison someone who is innocent, I think it is much worse to ignore pain in a vulnerable population, than to occasionally provide unnecessary treatment.
Furthermore, unlike adults, children cannot rationalise pain. I am able to put up with a needle for a blood test (OK, I whine a little bit), because I know it is for a good cause. I am able to limit my distress through rationalization. Children cannot, so again, extra caution is required.
Finally, a child’s negative experience in the emergency department will not just be due to pain. Although this post focuses on pain and analgesia specifically, we have to remember that distress has other contributors that we should address. The emergency department is a place that naturally provokes fear and anxiety, and we should do everything in our power to limit that distress, not just for children, but for all our patients.
Assessing pain
In general, we are not great at estimating a child’s pain by simple observation. (Singer 2002; Kelly 2002; Shavit 2008) Doctors and nurses might agree with each other, but if you actually ask the child, we are wrong a lot. (James 2017) If a child can talk, self-report is considered the best approach to assessing their pain. (Drendl 2017) For nonverbal children, there are a number of validated pain scores, but they all have one fatal weakness: they are validated using a guess about the child’s pain. They are based on observation, but observation doesn’t work in older children, so we probably have to assume it doesn’t work in younger children either. We will never know, as these children can’t report their pain. So although I think it is OK to consider these scores, it is important to recognize that they are imperfect.
In this vulnerable population we need to err on the side of caution. If a procedure or condition is painful in adults, you just have to assume its painful in children. Of course, there is a huge range of pain tolerance in adults. A procedure that can be done under local anesthetic for some patients may require procedural sedation for others. When a patient can communicate, the choice is simply a matter of asking about pain. For nonverbal children, I think the safest approach is to assume the highest estimate of pain. If some adults would want sedation for a procedure, I think sedation should be the standard for those who cannot participate in the conversation.
Pediatric pain management strategies
That was a fairly lengthy introduction. Let’s get into the important stuff: things we can do to prevent, limit, or treat childrens’ pain in the emergency department.
Limit painful procedures
Perhaps the best strategy to reduce pain is simply to avoid causing pain in the first place. (Witt 2016; AAP 2007) Before doing any invasive procedure, always consider if the procedure is required. Evidence based medicine has an incredible role to play in reducing investigations and therefore pain. For example, understanding that UTI is almost never a serious bacterial illness in a well appearing infant limits the need for invasive procedures to collect urine.
I find it helpful to speak to the pediatrician before drawing blood work “I know they are going to want”. Sometimes the bloodwork isn’t needed at all. More often, they might want to add some esoteric test, and speaking with them first can prevent the need for multiple blood draws. Bunching tests or treatments together often makes sense.
On the other hand, although it makes sense to group painful procedures together, other times it is better to just get things done. We sometimes delay procedures because we worry that the child will be difficult or require a sedation. As a result, they sit longer with their abscess, or foreign body, or burn, prolonging pain. When a procedure is necessary, just get it done.
Furthermore, the emergency department is often the best place for procedures. Procedural sedation is not available in other areas of the hospital. If a child with a borderline fracture is seen in an ortho clinic, it will often be “gently” adjusted without the benefit of sedation. The same goes for the debridement of burns in plastic surgery clinics and foreign body removal in ENT clinics. We are sedation experts, and it is often better for our patients if we use that expertise. However, not everything should be done in the chaos of the emergency department, and using our anesthetic colleagues and the controlled setting of the OR is also occasionally a great idea. The best option will depend on your hospital set up.
A few specific considerations
Heel sticks: Heel sticks are routinely used in pediatrics, but there is evidence that venipuncture is less painful and so probably should be prefered. (Logan 1999; Ogawa 2005) The preference for venipuncture is probably strengthened by the fact that EMLA can be used, while it is ineffective for heel sticks. (Lago 2009) If a heel stick is used, the heel should not be squeezed as it significantly increases pain without improving the efficacy of the procedure. (Lago 2009)
Intraosseous lines: Although it doesn’t sound like it, an intraosseous line can actually be an analgesic procedure. I’ve watched a neonate have multiple IV attempts by 6 or 7 different providers. That unnecessary pain is entirely my fault. The pain would have been far less, and the resuscitation far better, if I had stuck to my rule of 2 IV attempts then IO.
IM injections: I often see medications given intramuscularly or subcutaneously, because we are afraid to start an IV. However, IM medications hurt more than an IV start, and do not provide the option for subsequent doses. If the patient might need more than one parenteral dose, I start an IV. (On the other hand, the oral route is equally effective for almost every analgesic, so if the child is tolerating PO, forget needles all together and given the medication orally).
Let nurses treat pain
As great as my profession is, one thing about doctors is that we aren’t very good at routine tasks or following protocols. If you want to see consistent and prompt management of children’s pain, create protocols and put nurses in charge. (Yanuka 2008; Corwin 2012; Sampson 2014)
Topical anesthetics (eg. EMLA)
There is plenty of evidence that ELMA reduces pain from needle insertion. (Lander 2006; Baxter 2013; Young 1996; Lim 2017) It has also been shown to reduce pain from and is recommended for circumcision. (Witt 2016; Taddio 200) Unlike sucrose, children’s self reported pain is reduced by EMLA. (Lander 2006) EMLA may also increases the rate of successful venipuncture in the emergency department (Baxter 2013) and is associated with improved success in pediatric lumbar punctures. (Baxter 2006; Nigrovic 2007)
One recent meta-analysis showed no difference between EMLA and placebo in infants less than 3 months of age. (Shahid 2018) However, the numbers were small, and the point estimates do make EMLA look better, just marginally so. The authors were concerned about methemoglobinemia in this age group, but there were no reported bad outcomes among the 412 infants included.
There are a large number of studies of EMLA, and it appears to have a very good safety profile. The biggest concern would be methemoglobinemia, especially in children with concomitant G6PD deficiency. (Witt 2016)
- The recommended maximum doses for EMLA are:
- Less than 3 months: 1 gram on 10cm2 (1 finger tip unit, or a line of cream from the DIP to the finger tip, is approximately 0.5 grams of topical medication)
- 3-12 months: 2 grams on 20cm2
- 1-6 years: 10 grams on 100cm2
Studies demonstrating effectiveness generally left EMLA for at least 1 hour. It doesn’t look effective after shorter durations, so patience is essential, and it may not be appropriate for all emergency department patients. (Yamamoto 1998)
There are a large number of alternative topical anesthetics (tetracaine 2% cream, liposomal lidocaine 4%, liposomal lidocaine 5%, lidocaine 7%/tetracaine 7%), however most have not specifically been evaluated in children. (Witt 2016) Amethocaine may provide superior pain relief to EMLA. (Lawson 1995; Lander 2006) Liposomal lidocaine has the advantage of a faster onset time (30 minutes) and it doesn’t require an occlusive dressing (Lago 2009; Drendl 2017).
LET (a combination of lidocaine, epinephrine, and tetracaine) is another excellent option that can be used on open wounds for laceration repair.
Local anesthetics
Local infiltration of lidocaine is suggested to reduce pain from procedures such as PICC line insertion, arterial line, central line placement, lumbar puncture, and circumcision. (Witt 2016)
Sources recommend against using lidocaine with epinephrine in the neonate population, for fear of tissue necrosis, but no citations are provided, and that sounds a lot like the myth of not using epinephrine in fingers and toes to me. (Witt 206) I do use epinephrine with most lidocaine injections, but you will have to decide for yourself.
- Maximum lidocaine dose:
- 3mg/kg
- 7mg/kg with epinephrine
- 1% lidocaine is 10mg/ml. In small infants, you can reach the toxic dose very quickly, so make sure you do the math. I often dilute to 0.5% to give myself more volume to work with.
There are a number of techniques that can be used to decrease the pain on infiltration of local anesthetic, included buffering with bicarbonate, warming, using the smallest possible needle, distraction, pre-application of EMLA, using the smallest volume possible, and infiltrating slowly. (Scarfone 1998; Quaba 2005)
Nerve blocks
An entire post could be dedicated to nerve blocks. They are a great option both for procedures and managing painful conditions, such as fractures.
Simple analgesics
Acetaminophen is widely recommended for mild to moderate pain from procedures, including heelsticks, dressing changes, circumcision, and venipuncture. (Witt 2016; Shah 1998)
- Maximum total daily acetaminophen dose: (Witt 2016)
- Less than 1 month: 60mg/kg
- 1-3 months: 75mg/kg
Ibuprofen is contraindicated before 6 months of age, but is an excellent analgesic in older infants. (Witt 2016)
Opioid analgesia
Opioids are excellent pain medications with a good margin of safety. They are recommended for more painful procedures, such as debridement, incision and drainage, lumbar puncture, tracheal intubation, chest tube insertion and central line placement. (Witt 2016)
There is an entire blog post in the works about codeine, but I see no role for its use in any age group. In infants in particular, there have been adverse events because of rapid metabolizers. Numerous organizations, including the American Academy of Pediatrics, the Canadian Pediatrics Society, the FDA, and Health Canada have warned against using codeine in children younger than 12 years of age.
Fentanyl is a great option, but it might have altered pharmacokinetics in neonates, with a half life up to 10 hours. (AAP 2007)
In general, neonates (less than one month) will require lower, titrated doses, whereas toddlers (because of higher metabolisms) require somewhat larger doses.
Low dose ketamine
Low dose ketamine is being used more often for pain control in adults. I am not aware of any literature looking at ketamine for pain control in infants, but it’s safety profile makes this an attractive option for many procedures.
Intranasal anxiolysis and pain control
Many of the medications we use for analgesia and anxiolysis can be administered intranasally, eliminating the need for needles (although intranasal sprays are not entirely pain free). I routinely use IN ketamine, midazolam, and fentanyl in the care of children. The biggest limitation is volume in older children, as you are limited to a maximum of about 1 mL per nostril, but ideally should use smaller volumes than that. In smaller doses, remember that the atomizer will typically have 0.1 mL of dead space that has to be accounted for when drawing up the medication. (Drendl 2017)
Nitrous oxide
Nitrous oxide is rarely available in Canada, so I have had limited experience with it until my recent move to New Zealand. (Now that I have it, I love it.) It acts as a weak dissociative agent, with action both at opioid and NMDA receptors. It has reasonably good evidence. (Reinoso-Barbero 2011, Lee 2012) The onset is within 5 minutes and recovery time 3-5 minutes after discontinuation, with a very low rate of serious adverse events, although vomiting is relatively common. (Tsze 2016; Drendl 2017)
Procedural sedation
Although it takes time, there are a number of procedures where sedation is the best option. This is a difficult assessment in infants. There is a huge variance in pain tolerance among individuals. In adults, we know that the same sized abscess in the same location can be drained with a field block in some individuals, but will require deep sedation in others. In adults the decision is easy – I just ask. Often we will make an attempt using local, but the patient can tell me to stop if it isn’t tolerated, and we can transition to sedation. Unfortunately, we can’t ask infants, and they are unable to tell us to stop if we are causing them pain. Therefore, I think that we have to be extra cautious in this population. If sedation would be requested by a significant proportion of adult patients, it is probably best to use it routinely in infants.
Address the underlying issue
Don’t forget to address the underlying condition. This is especially true for orthopedics, where splinting is incredibly important in reducing pain. If a fracture seems likely, it makes sense to splint prior to x ray.
Other non-pharmacologic interventions
There are are a variety of non-pharmacologic interventions described in children. Much like sucrose, there is limited evidence that any of these interventions provides analgesia. I think they are more likely to be calming than truly analgesic. However, they are probably comforting, limiting overall distress, and so are valuable as adjuncts. (Matthew 2003)
- Breast feeding: A Cochrane review concluded that breast feeding decreases pain from procedures, and is equally effective to sucrose. (Shah 2012) The quality of the studies isn’t great. I think “reduces pain” is the wrong conclusion. Just like the sucrose, what is observed is decreased crying and grimacing (in various scores), which doesn’t necessarily mean decreased pain.
- Non-nutritive sucking: A Cochrane review concludes that it reduces crying and behavioural scores. (Johnston 2017) Again, not necessarily pain. Physiologic parameters mixed. Lack of blinding makes all studies high risk for bias.
- Swaddling, facilitated tucking, rocking, holding: Another Cochrane review concludes these interventions decrease crying and behavioural pain scores. Again, pain not evaluable. High risk of bias, primarily because of lack of blinding. (Pillai 2015)
- Other options that are described include skin to skin care, vocal soothing, and tactile stimulation of alternate nerve fibres.
- Olfactory stimulation (vanillin aroma) has also been described. (Goubet 2003)
- Sensorial saturation: Essentially involved combining everything above, so that visual, auditory, tactile, and gustatory sensation is all engaged to distract the infant, or decrease pain signals. (Lim 2017; Locatelli 2018)
- If possible, don’t wake a child up just to do a painful procedure. (Lago 2009) How would you like to be woken in the middle of the night an immediately jabbed with a needle? Waiting until the child is awake makes sense.
- As children get older, explanations, pep talks, music, distractions, and child life specialists are invaluable, but the focus of this post is really preverbal infants. For good advice in the older child group, see the FOAMed suggestions at the end of this post. Don’t underestimate the value of technology. The trance induced by a cell phone screen may drive parents nuts when there are chores to be done, but can be invaluable in the emergency department. Of course, as my FOAMed friends would emphasize, don’t forget the bubbles.
It must be re-emphasised that non-pharmacological interventions practised in isolation are unlikely to relieve pain. They are more useful as complementary strategies to pharmacological methods of relieving acute pain.”
(Matthew 2003)
Use multiple options
There is no one size fits all option. Different scenarios will require different analgesic and anxiolytic techniques. Most scenarios call for more than one, such as the combination of EMLA, extra local anesthetic, an anxiolytic, and nonpharmacologic techniques in a child who requires a lumbar puncture.
Conclusion
Children, especially those who cannot speak, are a vulnerable population whose pain is consistently undertreated. This is unacceptable, especially when considering the wide variety of treatment modalities available. All emergency physicians should be comfortable controlling pain in a pediatric population.
Assessment of pain is particularly difficult when children cannot speak. An infant’s pain is fundamentally unknowable, so we have to guess. There are numerous validated pediatric pain scales, but all are subject to the same fundamental flaw in that they measure observed behaviours not pain. Rather than (or in addition to) using these scales, I would suggest drawing on our experience with older patients, who can describe their pain. If a procedure or medical condition hurts in verbal patients, we have to assume it also hurts in infants. If most (or even some) older patients would want treatment for their pain, we have to assume that infants would also want treatment. It is better to err on the side of overtreatment than subjecting this vulnerable population to needless pain.
Other FOAMed
Paediatric Pain and Sedation – Tips to Change Your Practice from #EuSEM15 by Natalie May; Natalie May also covered pain scales in this post
PEM Playbook by Tim Horeczko has an excellent resource on pediatric pain control.
Emergency Medicine Cases: Pediatric Pain Management and Pediatric Procedural Sedation
SGEM 78: Pediatric pain control
Pediatric Pain Management Pearls with Sebrina Perkins on REBELEM
A Rational Approach to Managing Acute Pain in Children on Science Based Medicine
Topical Anesthetic Creams on Don’t Forget the Bubbles
References
AAP. Prevention and management of pain in the neonate. An update. Advances in neonatal care : official journal of the National Association of Neonatal Nurses. 2007; 7(3):151-60. [pubmed]
Alexander J, Manno M. Underuse of analgesia in very young pediatric patients with isolated painful injuries. Annals of emergency medicine. 2003; 41(5):617-22. [pubmed]
Baxter AL, Fisher RG, Burke BL, Goldblatt SS, Isaacman DJ, Lawson ML. Local anesthetic and stylet styles: factors associated with resident lumbar puncture success. Pediatrics. 2006; 117(3):876-81. [pubmed]
Baxter AL, Ewing PH, Young GB, Ware A, Evans N, Manworren RC. EMLA application exceeding two hours improves pediatric emergency department venipuncture success. Advanced emergency nursing journal. 2013; 35(1):67-75. [pubmed]
Carbajal R, Rousset A, Danan C, et al. Epidemiology and treatment of painful procedures in neonates in intensive care units. JAMA. 2008; 300(1):60-70. [pubmed]
Corwin DJ, Kessler DO, Auerbach M, Liang A, Kristinsson G. An intervention to improve pain management in the pediatric emergency department. Pediatric emergency care. 2012; 28(6):524-8. [pubmed]
Dohrenwend PB, Fiesseler FW, Cochrane DG, Allegra JR. Very young and elderly patients are less likely to receive narcotic prescriptions for clavicle fractures. The American journal of emergency medicine. 2007; 25(6):651-3. [pubmed]
Drendel AL, Ali S. Ten Practical Ways to Make Your ED Practice Less Painful and More Child-Friendly Clinical Pediatric Emergency Medicine. 2017; 18(4):242-255.
Friedland LR, Pancioli AM, Duncan KM. Pediatric emergency department analgesic practice. Pediatric emergency care. 1997; 13(2):103-6. [pubmed]
James F, Edwards R, James N, Dyer R, Goodwin V. The Royal College of Emergency Medicine composite pain scale for children: level of inter-rater agreement. Emergency medicine journal : EMJ. 2017; 34(6):360-363. [pubmed]
Johnston CC, Bournaki MC, Gagnon AJ, Pepler CJ, Bourgault P. Self-reported pain intensity and associated distress in children aged 4-18 years on admission, discharge, and one-week follow up to emergency department. Pediatric emergency care. 2005; 21(5):342-6. [pubmed]
Johnston C, Campbell-Yeo M, Disher T, et al. Skin-to-skin care for procedural pain in neonates. The Cochrane database of systematic reviews. 2017; 2:CD008435. [pubmed]
Kelly AM, Powell CV, Williams A. Parent visual analogue scale ratings of children’s pain do not reliably reflect pain reported by child. Pediatric emergency care. 2002; 18(3):159-62. [pubmed]
Lago P, Garetti E, Merazzi D, et al. Guidelines for procedural pain in the newborn. Acta paediatrica. 2009; 98(6):932-9. [pubmed]
Lander JA, Weltman BJ, So SS. EMLA and Amethocaine for reduction of children’s pain associated with needle insertion. Cochrane Database of Systematic Reviews 2006, Issue 3. Art. No.: CD004236. DOI: 10.1002/14651858.CD004236.pub2
Lago P, Guadagni A, Merazzi D, et al. Pain management in the neonatal intensive care unit: a national survey in Italy. Paediatric anaesthesia. 2005; 15(11):925-31. [pubmed]
Lawson RA, Smart NG, Gudgeon AC, Morton NS. Evaluation of an amethocaine gel preparation for percutaneous analgesia before venous cannulation in children. British journal of anaesthesia. 1995; 75(3):282-5. [pubmed]
Lee JH et al. A Randomized Comparison of Nitrous Oxide Versus Intravenous Ketamine for Laceration Repair in Children. Pediatr Emerg Care 2012. PMID: 23187987
Lim Y, Godambe S. Prevention and management of procedural pain in the neonate: an update, American Academy of Pediatrics, 2016. Archives of disease in childhood. Education and practice edition. 2017; 102(5):254-256. [pubmed]
Locatelli C, Bellieni CV. Sensorial saturation and neonatal pain: a review. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. 2018; 31(23):3209-3213. [pubmed]
Logan PW. Venepuncture versus heel prick for the collection of the Newborn Screening Test. The Australian journal of advanced nursing : a quarterly publication of the Royal Australian Nursing Federation. ; 17(1):30-6. [pubmed]
Mathew PJ, Mathew JL. Assessment and management of pain in infants. Postgraduate medical journal. 2003; 79(934):438-43. [pubmed]
Nigrovic LE, Kuppermann N, Neuman MI. Risk factors for traumatic or unsuccessful lumbar punctures in children. Annals of emergency medicine. 2007; 49(6):762-71. [pubmed]
Ogawa S. Venepuncture is preferable to heel lance for blood sampling in term neonates Archives of Disease in Childhood – Fetal and Neonatal Edition. 2005; 90(5):F432-F436.
Petrack EM, Christopher NC, Kriwinsky J. Pain management in the emergency department: patterns of analgesic utilization. Pediatrics. 1997; 99(5):711-4. [pubmed]
Pillai Riddell RR, Racine NM, Gennis HG, et al. Non-pharmacological management of infant and young child procedural pain. The Cochrane database of systematic reviews. 2015; [pubmed]
Quaba O. A users guide for reducing the pain of local anaesthetic administration Emergency Medicine Journal. 2005; 22(3):188-189.
Reinoso-Barbero F et al. Equimolar Nitrous Oxide/Oxygen vs Placebo for Procedural Pain in Children: A Randomized Trial. Pediatrics 2011. PMID: 21606149
Robb AL, Ali S, Poonai N, Thompson GC, . Pain management of acute appendicitis in Canadian pediatric emergency departments. CJEM. 2017; 19(6):417-423. [pubmed]
Scarfone RJ, Jasani M, Gracely EJ. Pain of local anesthetics: rate of administration and buffering. Annals of emergency medicine. 1998; 31(1):36-40. [pubmed]
Sampson FC, Goodacre SW, O’Cathain A. Interventions to improve the management of pain in emergency departments: systematic review and narrative synthesis. Emergency medicine journal : EMJ. 2014; 31(e1):e9-e18. [pubmed]
Shah V, Taddio A, Ohlsson A. Randomised controlled trial of paracetamol for heel prick pain in neonates. Archives of disease in childhood. Fetal and neonatal edition. 1998; 79(3):F209-11. [pubmed]
Shah PS, Herbozo C, Aliwalas LL, Shah VS. Breastfeeding or breast milk for procedural pain in neonates. The Cochrane database of systematic reviews. 2012; 12:CD004950. [pubmed]
Shahid S, Florez ID, Mbuagbaw L. Efficacy and Safety of EMLA Cream for Pain Control Due to Venipuncture in Infants: A Meta-analysis. Pediatrics. 2018; [pubmed]
Shavit I, Kofman M, Leder M, Hod T, Kozer E. Observational pain assessment versus self-report in paediatric triage. Emergency medicine journal : EMJ. 2008; 25(9):552-5. [pubmed]
Simons SH, van Dijk M, Anand KS, Roofthooft D, van Lingen RA, Tibboel D. Do we still hurt newborn babies? A prospective study of procedural pain and analgesia in neonates. Archives of pediatrics & adolescent medicine. 2003; 157(11):1058-64. [pubmed]
Singer AJ, Gulla J, Thode HC. Parents and practitioners are poor judges of young children’s pain severity. Academic emergency medicine. 2002; 9(6):609-12. [pubmed]
Taddio A, Shah V, Gilbert-MacLeod C, Katz J. Conditioning and hyperalgesia in newborns exposed to repeated heel lances. JAMA. 2002; 288(7):857-61. [pubmed]
Taddio A, Ohlsson K, Ohlsson A. Lidocaine-prilocaine cream for analgesia during circumcision in newborn boys. Cochrane Database Syst Rev. 2000;2:CD000496
Tsze DS, Mallory MD, Cravero JP. Practice Patterns and Adverse Events of Nitrous Oxide Sedation and Analgesia: A Report from the Pediatric Sedation Research Consortium. The Journal of pediatrics. 2016; 169:260-5.e2. [pubmed]
Witt N, Coynor S, Edwards C, Bradshaw H. A Guide to Pain Assessment and Management in the Neonate Curr Emerg Hosp Med Rep. 2016; 4(1):1-10.
Yamamoto LG, Boychuk RB. A blinded, randomized, paired, placebo-controlled trial of 20-minute EMLA cream to reduce the pain of peripheral i.v. cannulation in the ED. The American journal of emergency medicine. 1998; 16(7):634-6. [pubmed]
Yanuka M, Soffer D, Halpern P. An interventional study to improve the quality of analgesia in the emergency department. CJEM. 2008; 10(5):435-9. [pubmed]
Young SS, Schwartz R, Sheridan MJ. EMLA cream as a topical anesthetic before office phlebotomy in children. Southern medical journal. 1996; 89(12):1184-7. [pubmed]
Morgenstern, J. Pediatric Pain Management, First10EM, March 25, 2019. Available at:
https://doi.org/10.51684/FIRS.8176


One thought on “Pediatric Pain Management”