Time for another rapid recap of some important, inane, or interesting emergency medicine literature. Not a single paper about coronavirus though – you will have to stick to CNN for that. As always, the podcast version will be on the BroomeDocs podcast.
Hold up – you want to shove that giant plastic tube into my chest?!?! But doctor – I feel fine! Can I at least get a second opinion?
The PSP trial: Brown SGA, Ball EL, Perrin K, et al. Conservative versus Interventional Treatment for Spontaneous Pneumothorax. The New England journal of medicine. 2020; 382(5):405-415. PMID: 31995686 [full text]
I think this will be a practice changing article for a lot of people. They took people with a large primary spontaneous pneumothorax, and randomized them to either a chest tube or nothing (conservative therapy). There are some problems with the trial. It is not blinded. They use a disease oriented outcome. Their choice of non-inferiority margin is somewhat large. Patients were lost to follow-up and others crossed over between the two groups. Despite all that, I think the conclusions are correct. Conservative therapy was non-inferior to invasive therapy. In fact, I think the data says it was better, with less time off work, less time in hospital, and fewer serious adverse events. I have already been offering conservative therapy to my patients for years based on observational data, so it’s really nice to see an RCT that supports that practice.
Bottom line: Not every patient with a pneumothorax needs plastic in their pleural space. Shared decision making is the key.
Everyone loves topical TXA – but does it work in upper GI bleed?
Karadaş A, Doğan NÖ, Pinar SG, et al. A randomized controlled trial of the effects of local tranexamic acid on mortality, rebleeding, and recurrent endoscopy need in patients with upper gastrointestinal hemorrhage. European journal of gastroenterology & hepatology. 2020; 32(1):26-31. PMID: 31567714
This is a single-centre, placebo controlled, double-blind RCT that compared topical TXA (2 grams via an NG tube) to placebo in 162 adult emergency department patients with objective evidence of upper GI bleed. They excluded 5 patients after randomization because they had variceal bleeds, but this is a methodologic faux-pas. We would obviously have to treat these patients in the ED, as we don’t know the source of bleeding, so their outcomes need to be considered as well. The primary outcome is a pretty bad composite that includes things that really matter (mortality) with relatively irrelevant outcomes (ED revist). There was no statistically significant difference in this primary outcome, although the TXA group actually did worse (32.1% vs 29.1%, p=0.69). There were no statistically significant differences in anything. In terms of the most important outcome, mortality was 10.3% with TXA and 12.7% with placebo (p=0.64). This could represent a clinically important difference that the trial was simply not powered to detect. The Cochrange review on TXA for GI bleeds indicates a possible mortality benefit, but the underlying data is significantly flawed. (Bennett 2014) There is a large RCT currently underway from the same group that has given us CRASH 2, CRASH 3, and WOMAN, called the HALT-IT trial, that is designed to determine if TXA decreases all cause mortality in GI bleed. (Roberts 2014) Personally, I am not sure why I would choose to use TXA through an NG when the IV route is available.
Bottom line: This study does not support the use of topical TXA for upper GI bleeds. It is unknown whether IV TXA might help these patients.
Your results may vary: the imprecision of medical measurements
McCormack JP, Holmes DT. Your results may vary: the imprecision of medical measurements. BMJ (Clinical research ed.). 2020; 368:m149. PMID: pubmed
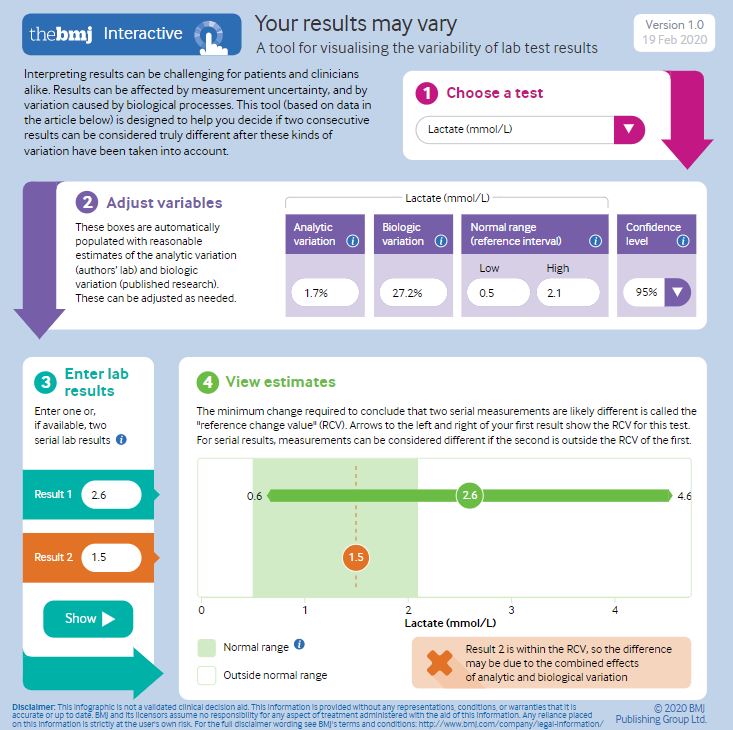
The bottom line suggestion from this paper is that our lab results should really come with error bars. They discuss three sources of imprecision in our lab results: preanalytical error (differences in the way specimens are collected, handled, stored, or shipped), analytical error (the imprecision of the test itself), and biologic variation. They suggest that biologic variation, the extent to which human physiology naturally varies over time, is probably the most important source of error, and it certainly affects our ability to monitor patients over time. They give some excellent examples focused on primary care that highlight the potential problems of trying to track cholesterol, bone density, and hemoglobin A1c over time. Although the focus is primary care, this issue is also essential in emergency medicine. I love their clinical summary: “much of the uncertainty in clinical measurements is not a fixable problem but only a knowable problem.”
They published a great interactive tool with this paper that you might want to play around with. For example, as you can see in the image below, if you get a lactate value of 2.6 (ie a high lactate) and then repeat the test and get a value of 1.5 (ie normal), the tool tells you that the second result is within the error bars for the first result, so a change between the two may not represent a true biological change. (I never covered the ANDROMEDA-SHOCK study here, but this imprecision in the lactate value goes a long way towards explaining those results, although there are also other reasons that following lactate in sepsis may not make sense.) You can find the BMJ interactive tool here.
Bottom line: You must consider the imprecision of the tests you order when interpreting the results. Ideally, this information would be incorporated into laboratory reporting.
Despite the conclusions here, Tamiful probably doesn’t work
Butler CC, van der Velden AW, Bongard E, et al. Oseltamivir plus usual care versus usual care for influenza-like illness in primary care: an open-label, pragmatic, randomised controlled trial. Lancet. 2020; 395(10217):42-52. PMID: 31839279
This trial tries to convince us that oseltamivir helps, but I am not convinced. It is an RCT of primary care patients over 1 year of age with an influenza like illness who were randomized to oseltamivir or no treatment (there was no placebo, and that is the reason the whole trial fails). They report that Tamiflu decreases symptoms by 1 day, but the outcome was based on the patient’s symptom journal and the trial was not blinded. There was no difference in any of the objective outcomes, including hospitalizations, repeat healthcare visits, or use of over the counter medications. The authors present us with proof that we are just seeing the placebo effect in an unblinded trial: the symptom reduction was identical whether the patient tested positive for influenza or not. Oseltamivir only works against influenza, so the fact that patients with other viral illnesses also got better clearly demonstrates that the entire benefit was from the placebo effect.

Bottom line: Despite the headlines, there is still no role for oseltamivir in outpatients with influenza (and also no good evidence that it helps inpatients).
Cranial burr holes in the emergency department: to drill or not to drill?
Howard A, Krishnan V, Lane G, Caird J. Cranial burr holes in the emergency department: to drill or not to drill? Emergency medicine journal : EMJ. 2019; PMID: 31888954
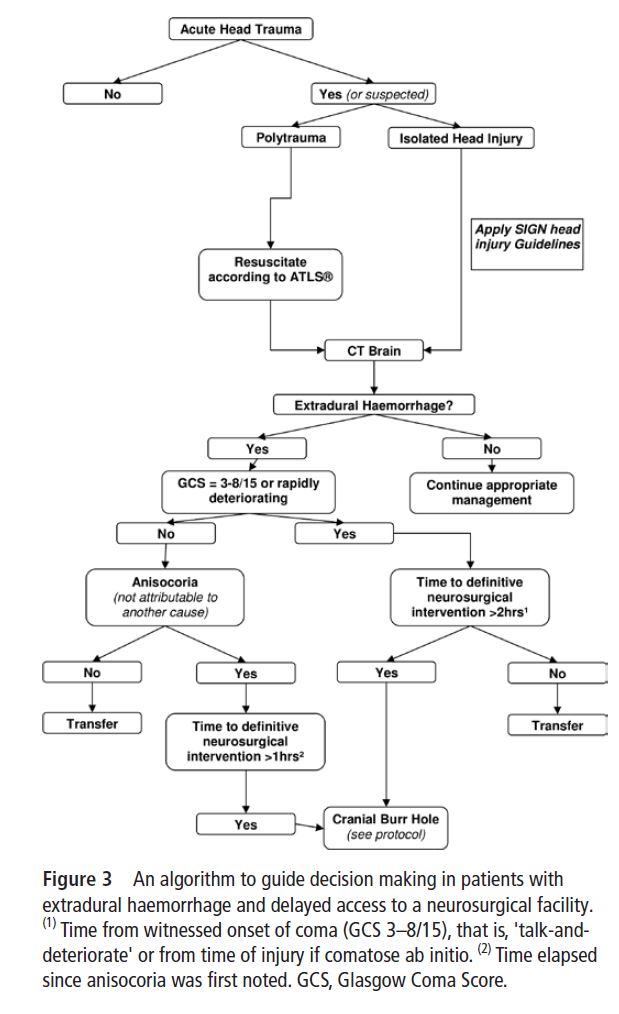
This is an interesting discussion – based around 2 cases in which burr holes were drilled by emergency doctors in the emergency department – about when we might want to consider performing burr holes ourselves rather than waiting for the neurosurgeon. They discuss some past data, but honestly the evidence is very weak. In one case series of patients with extra-axial hemorrhage and bilateral fixed dilated pupils, and impressive 2/3 of patients survived and half of them had favourable neurologic outcomes. Based on that, they argue we should consider the burr hole a life saving invasive procedure akin to decompression of the chest, and that in the right context it is a procedure that emergency doctors should be performing. I tend to agree, but it will depend a lot on how far you are from neurosurgery and the clinical details of the patient in front of you. As an interesting side note, both the the patients they describe required repeated irrigation and suction of the hematoma during the 2.5 hour transfer to neurosurgery, and most of what was evacuated was clot. They therefore make the argument that you really need a proper drill rather than the makeshift IO needle, which gas been reported, and we discussed in the research roundup previously. There is a good letter to the editor by Mike Abernathy discussing this paper, and seconding the argument that this is a procedure we should be able to do in emergency departments. (Abernathy 2020)
Bottom line: In Markham, it should take us less than 2 hours to get patients to a neurosurgeon, so their algorithm indicates a burr hole is probably unnecessary. However, for those working elsewhere, this may be an important discussion to have with your local group.
Are there no bounds to my medical ignorance?
Mendonça CN, Silva PM, Avelleira JC, Nishimori FS, Cassia Fde F. Shiitake dermatitis. Anais brasileiros de dermatologia. ; 90(2):276-8. PMID: 25831007 [free full text]
I had definitely never heard of this before: flagellate or Shiitake dermatitis. It is caused by a toxic reaction to lentinan, a component of shiitake mushrooms. It is heat labile, so destroyed as long as the mushrooms are cooked. There also seems to be an individual component, as not all people exposed to lentinan develop the syndrome. You develop pruritic linearly arranged erythematous papules 2-3 days after eating raw or undercooked shiitake mushrooms. The lesions are self-limited, and there are no other symptoms, so you don’t need to do much. The pruritis can be intense, so antihistamines and steroids may be required.
The quest for a STEMI equivalent in stroke
The WAKE UP Trial: Thomalla G, Simonsen CZ, Boutitie F, et al. MRI-Guided Thrombolysis for Stroke with Unknown Time of Onset. The New England journal of medicine. 2018; 379(7):611-622. PMID: 29766770 [free full text]
My feelings about thrombolytics for ischemic stroke are pretty well known. Our current approach doesn’t work, but I have long wondered about finding a “ST elevation” equivalent in stroke that would help us identify the subset of patients that actually benefit. This trial pushes us in that direction, using advanced imaging to select patients for lytics, although unfortunately they are trying to use the advanced imaging to give lytics to more patients rather than less. This is a multicentre RCT that selected patients who were more than 4.5 hours from the onset of their stroke symptoms (or woke up with stroke symptoms) using MRI imaging, and randomized them to tPa or placebo. There was a benefit in terms of neurologic outcomes (53% vs 42%), but there were a number of problems with the trial, the biggest of which was the fact that they never actually finished it (they ran out of money). Mortality was also increased (4% vs 1%, p=0.07) and my guess is it would have been statistically significant if the trial was completed.
Bottom line: This imaging guided technique is interesting, and may result in better outcomes, but this trial is also consistent an increase in mortality (which isn’t good). We shouldn’t be treating patients with unknown time of symptom onset of wake up strokes yet.
The EXTEND Trial: Ma H, Campbell BCV, Parsons MW, et al. Thrombolysis Guided by Perfusion Imaging up to 9 Hours after Onset of Stroke. The New England journal of medicine. 2019; 380(19):1795-1803. PMID: 31067369 [full text]
This trial is similar to the last one. It is a multicentre RCT looking at advanced imaging (a different kind of imaging from the last trial) to guide thrombolytics in patients with wake up strokes or delayed presentations. Like the last trial, it was stopped early, which leaves us with more questions than answers. They claim a statistical improvement in neurologic outcomes based on a p value of 0.04, but the stats were only “significant” on an adjusted analysis, and it wasn’t the adjusted analysis they said they were going to do in their protocol. Once again, mortality looks about 3% worse in the lytics group, but not statistically so. I like the way that this research is going, but this trial looks negative and certainly shouldn’t result in changes to the way we manage stroke.
Bottom line: I imagine we will see more of these advanced imaging studies in the future, but we shouldn’t change practice at this point.
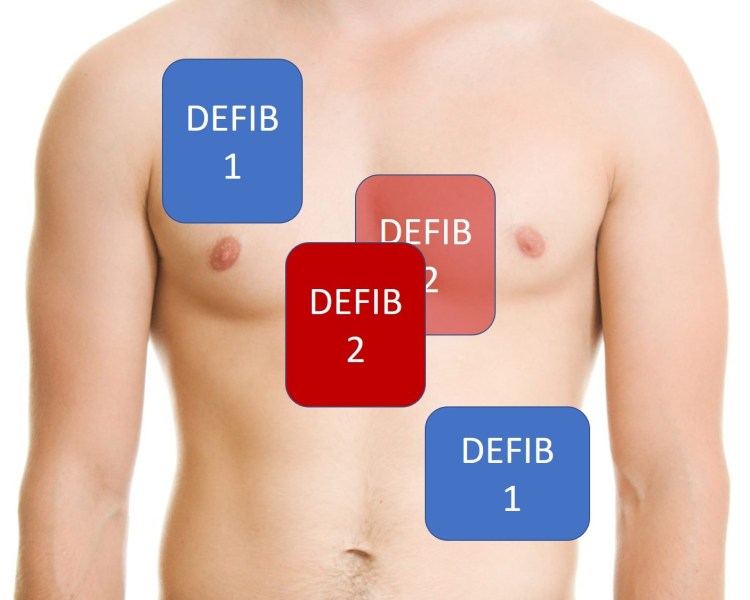
Light ‘em up: Double sequential defibrillation
Cheskes S, Dorian P, Feldman M, et al. DOuble Sequential External Defibrillation for Refractory Ventricular Fibrillation: The DOSE VF Pilot Randomized Controlled Trial. Resuscitation. 2020; PMID: 32084567
This is just a pilot study, so don’t get too excited, but it is our first randomized data on double sequential defibrillation. They randomized 152 patients with refractory ventricular fibrillation to either standard ACLS, double sequential defibrillation, or vector change defibrillation (changing the pads from anterior-lateral to anterior-posterior). Because it is just a pilot study, we can’t say too much about the outcomes. They don’t even provide confidence intervals, but ROSC was higher in the double sequential group, which counters some prior observational data that said outcomes might be worse. We still don’t know if this will translate into increased survival with good neurologic function, but while we wait for the main study, I think this is a reasonable technique to use. Importantly, they ensured that there was a slight delay between the two shocks by having the same paramedic run both machines. (Having both shocks occur simultaneously could damage the machines.)
Bottom line: It will take a while for the real study to come out, but I think it is reasonable to use double sequential defibrillation while you are waiting.
OK – Guys, I was joking
Bignucolo A, Parent A, Dube M, Kusnierczyk J, Ansell D, Ohle R. Triple-sequential defibrillation for refractory ventricular fibrillation in a 24-year-old male out of hospital cardiac arrest. CJEM. 2019; 21(6):809-811.
In the main write up of the double sequential defibrillation article, I joked that I was surprised that no one had moved on to triple sequential defibrillation yet. But of course, I was wrong. Some of my fellow Canadians published a case report describing exactly that. A 24 year old had a refractory ventricular fibrillation arrest and ultimately at the 80 minute mark, they successfully defibrillated him using 3 machines simultaneously. The patient walked out of the hospital neurologically intact. Although this is a very cool case, and it is great news that this guy survived, I wonder where this train of logic ends? Keep attaching defibrillators until we can’t see any more skin?
Marshmallows for diarrhea
Clarebrough E, Guest G, Stupart D. Eating marshmallows reduces ileostomy output: a randomized crossover trial. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland. 2015; 17(12):1100-3. PMID: 25951410
This is a randomized cross-over trial looking at the effects of marshmallows on ileostomy output. Subjects acted as their own controls. For 5 days they ate 3 marshmallows (4.8 grams each) 3 times a day, and for another 5 day period they refrained from eating marshmallows. They then monitored their own ileostomy output. (An unblinded trial that relies on patients measuring their own output is somewhat problematic.) They were told not to otherwise alter their diet, but I imagine that after eating 9 marshmallows a day, people might not have been as hungry, which itself could have led to decreased ostomy output. They did find that the total ostomy output was decreased (average difference 75 mL per day). 71% of patients had less output, but 21% reported an increase in output while on marshmallows. Is this paper somehow relevant to emergency medicine? I do occasionally see patients with high ostomy output as a chief complaint, so I guess this could be a therapeutic option. Of course, 9 marshmallows a day for the rest of your life is not exactly an ideal diet. However, it has been suggested that this effect might extrapolate to patients with acute infectious diarrhea. For an acute bout of diarrhea the extra calories may actually be a plus. If nothing else, this might provide you with a tasty placebo for a condition we otherwise treat with time. The next question is: how many marshmallows is ideal? If 9 a day is good, are 18 better?
Bottom line: Like honey for cough, marshmallows might be a tasty placebo for high output ostomies or maybe diarrhea in general?
Cheesy Joke of the Month

Other References
Abernethy M. Cranial burr holes in the emergency department: to drill or not to drill? Emergency medicine journal : EMJ. 2020; [pubmed]
Bennett C, Klingenberg SL, Langholz E, Gluud LL. Tranexamic acid for upper gastrointestinal bleeding. The Cochrane database of systematic reviews. 2014; [pubmed]
Chan CC, Chan YY, Tanweer F. Systematic review and meta-analysis of the use of tranexamic acid in tonsillectomy. European archives of oto-rhino-laryngology. 2013; 270(2):735-48. [pubmed]
Morgenstern, J. Research Roundup (March 2020), First10EM, March 16, 2020. Available at:
https://doi.org/10.51684/FIRS.12427