A new paper was published this month that is likely to change the way that a lot of people manage spontaneous pneumothorax (although I don’t think it will significantly change my practice)…
The paper
The PSP trial: Brown SGA, Ball EL, Perrin K, et al. Conservative versus Interventional Treatment for Spontaneous Pneumothorax. The New England journal of medicine. 2020; 382(5):405-415. PMID: 31995686 [full text]
The Methods
This is a multicenter, prospective, randomized, open-label, noninferiority trial that was conducted at 39 hospitals in Australia and New Zealand.
Patients
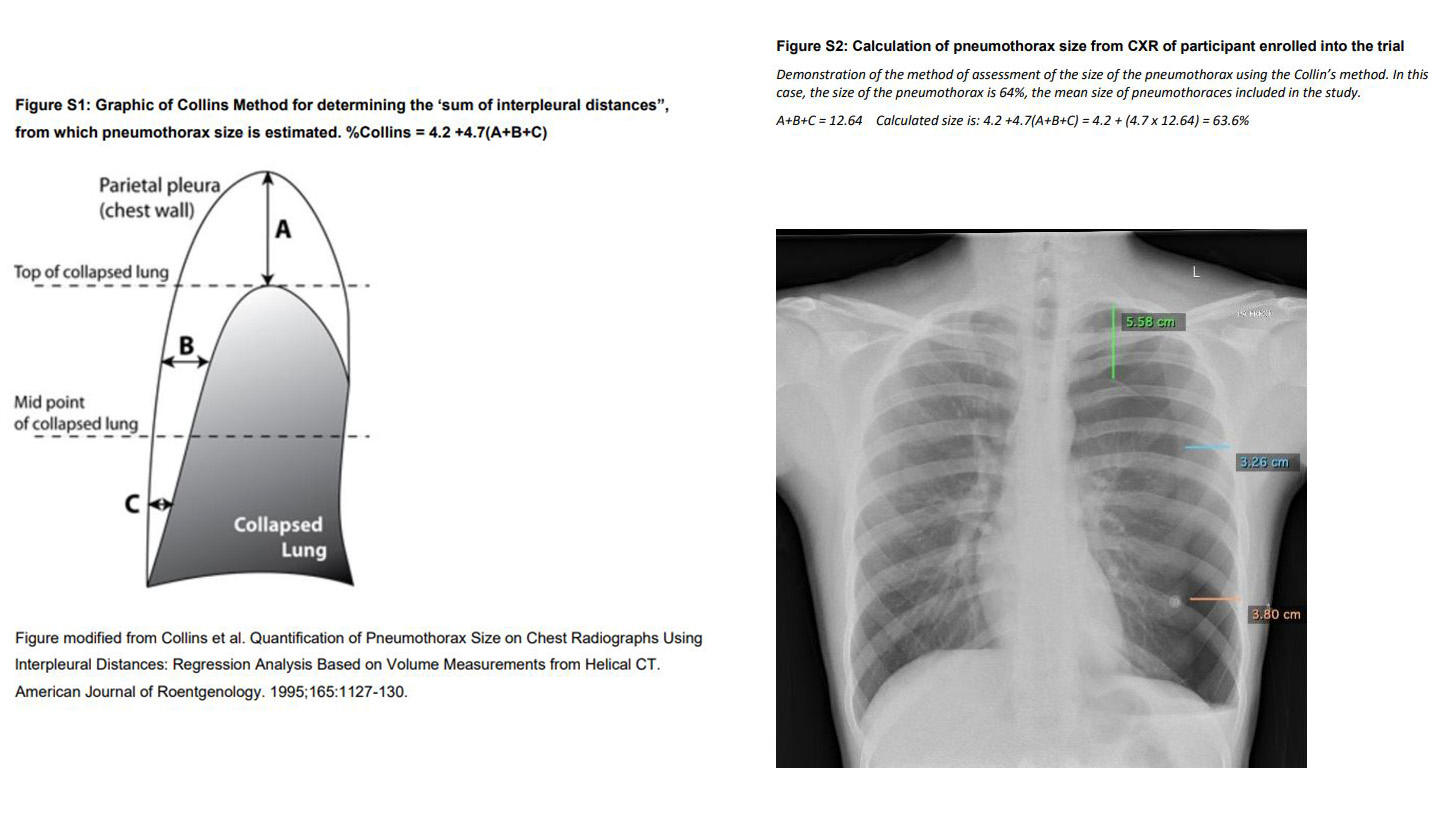
Patients aged 14 and 50 years of age were included if they had a unilateral primary spontaneous pneumothorax of 32% or more using the Collins method. (Instead of doing the math, this just means that the intrapleural distance measured at 3 spots added to more than 6cm. Just look at the images.)
Intervention
The intervention group received a chest tube. They used a small-bore (less than or equal to 12 French) tube. All tubes were attached to suction. The patient could be discharged home if the lung had re-expanded by 1 hour and remained fully expanded after the tube was clamped for a 4 hour observation period.
Comparison
The conservative management group did not receive a chest tube. They were observed in the emergency department for 4 hours (which is longer than my current practice) and a repeat chest x ray was obtained. The patients were discharged home if they were walking comfortably, were physiologically stable, and didn’t need supplemental oxygen.
Outcome
The primary outcome was complete radiologic resolution of the pneumothorax (which is obviously a surrogate outcome, and not the most clinically important outcome). They decided that a 9% absolute difference between the groups would be considered non-inferior.
The Results
After screening 2637 people over 6 years, they included a total of 316 patients. They only have outcome data at 8 weeks for 272 of those patients. The mean age was 26, 85% were males, the mean BMI was 21, and about half the patients were smokers. There was significant cross-over between the groups. 15% of the conservative management group actually ended up getting a chest tube, while 7% of the intervention group was actually treated conservatively.
For the primary outcome, radiologic resolution occurred in 98.5% of the intervention group at 8 weeks and 94.4% of the conservative management group (absolute difference 4.1%, 95% CI -8.6% to +0.5%). Because the 95% confidence interval is not larger than 9%, they conclude that conservative therapy is non-inferior to invasive therapy. The numbers are very similar in the per-protocol analysis.
Complete resolution of symptoms at 8 weeks was actually a little bit better in the conservative group (94.6% vs 93.4%).
The median time to radiologic resolution was 16 days in the invasive group and 30 days in the conservative group.
The number of patients with a procedure was 94% in the invasive group and 15% in the conservative group. The number of patients with a chest tube in longer than 72 hours was 51% in the invasive group and 9% in the conservative group.
CT usage was greater in the invasive group (19% vs 8%).
Serious adverse events were greater in the invasive group (12% vs 4%).
Pneumothorax recurrence within 12 months was greater in the invasive group (17% vs 9%). (I can’t really explain that. Does the tube interfere with healing? Or are the recurrent events caused by the removal of the tube? Would love to hear people’s thoughts.)
Hospital length of stay and hospital revisits were both greater in the invasive group.
The total number of days off work was longer in the invasive group (mean of 11 vs 6 days).

My thoughts
I love a lot of things about this trial. It should probably change practice for a large number of people in emergency medicine (although it is nowhere close to a “definitive” trial). I especially love their conclusion, which is written with greater modesty and insight than I am used to in medical research: this trial “provides modest, but statistically fragile, evidence that conservative management was noninferior to interventional management for radiographic resolution within 8 weeks, with the use of a 9-percentage-point margin…”
There are a few important limitations to this trial. It was unblinded (for obvious reasons). Significant cross-over increases the chance of seeing non-inferiority, which is why non-inferiority trials tend to focus on the per-protocol analysis. A 9% difference between the groups might be bigger than many of us would feel comfortable declaring “non-inferior”. There was significant loss to follow-up, which is probably expected with a radiologic primary outcome, because you have to convince people to come back for another x-ray at 2 months, even if they feel fine. Selection bias is also a possible problem, as more than 2600 patients were screened to find the 300 included. The choice of the primary outcome was also tricky, in that radiologic resolution is a potentially irrelevant surrogate, but at least it is objective and allowed radiologists to be blinded in this otherwise open-label study. More important outcomes, such as symptoms or return to normal activities, are all subjective and therefore problematic in an unblinded trial.
Although these issues limit the strength of the study, and we will definitely need more research in this area, I still consider this a practice changing article because we never had good evidence supporting our current invasive (and potentially harmful) practice, and because of the high probability that the conclusions of this study are correct based on what we already know about the topic.
When the study was released, my initial reaction on Twitter was “how did people not already know this?” I have been using a conservative approach to pneumothoraces for a number of years, based on what I considered to be decent evidence. However, as Dr. Andrew Petrosoniak was quick to point out, this was the first ever RCT looking at this specific issue. I think that apparent conflict provides some excellent insight into the nature of evidence based decision making.
The approach to pneumothorax that I was taught in residency was consistent with the guidelines of the American College of Chest Physicians, and involved putting a chest tube in any patient whose pneumothorax measured more than 3 cm from the apex to the cupola. (Baumann 2001) However, I spent a lot of my time in residency listening to old episodes of Emergency Medical Abstracts with Rick Bukata and Jerry Hoffman, and over the years I listened to them discuss a large number of studies that suggested using a more conservative approach.
It is true that, prior to this study, there was not a single strong RCT to guide our practice. However, a lack of RCTs is not the same as a lack of evidence.
There is an observational study from 1966 looking at all pneumothorax patients presenting to a thoracic surgery clinic. Of the 111 patients included, 75% were successfully managed with no intervention at all. If you just look at patients with simple pneumothoraces the rate was more than 80%. (Stradling 1966) In another series of 226 patients with spontaneous pneumothorax, 76% were managed successfully as outpatients. This included 49 patients managed conservatively, only 1 of whom went on to have a surgical procedure. (Mercier 1976) A chart review identified 203 episodes of spontaneous pneumothorax, of which 45 were treated with observation alone. Observation was successful in 79% of cases. It isn’t clear why an intervention was felt to be necessary in the other 21% of patients, but none of the interventions were done emergently. (Kelly 2008) Another chart review identified 234 adult patients with spontaneous pneumothorax. 63% of the small and 10% of the large pneumothoraces were managed conservatively, without significant adverse events. (Kelly 2008) One review suggests that 90% of small pneumothoraces managed conservatively will completely resorb. (Kelly 2007)
There have also been a number of studies looking at observation of pneumothoraces in trauma. Johnson looked retrospectively at 29 trauma patients with x-ray proven pneumothoraces who were treated conservatively, and only 2 failed, in that their pneumothorax got bigger on radiology, but they were still asymptomatic. (Johnson 1996) Moore and colleagues looked at 588 patients with pneumothorax visible on CT but not x-ray, 79% of which were treated conservatively, and only 6% failed conservative management. (Moore 2011) Another observational study looked at 602 patients in a registry coded as having either pneumothorax or hemothorax. The patients were relatively sick (ISS 26). 42% of the patients did not have a chest drain placed at the time of diagnosis, and 90% of those patients had their chest injury managed entirely conservatively (including patients on positive pressure ventilation). (Walker 2018)
A lot of the data on a more conservative approach to pneumothorax comes from literature looking at aspiration. An observational study of 114 adults with 131 simple pneumothoraces demonstrated a 75% success rate with iatrogenic pneumothorax and a 53% success rate with spontaneous pneumothorax. (Delius 1989) There is a 2008 systematic review that found 3 RCTs showing no difference between aspiration and chest tube in terms of failure, complications, or recurrence, but chest tubes result in significantly longer hospital stays. (Zehtabchi 2008) One small RCT from 2012 showed that aspiration had the same success rate (100% at 2 weeks), same 1 year recurrence, and shorter hospital stays when compared to chest tubes. (Parlak 2012) Another RCT (previously covered here) compared aspiration to chest tube in 127 adult patients with spontaneous pneumothorax. Aspiration worked in 75% of patients, resulted in shorter hospital stays, and appeared to have fewer complications. (Thelle 2017) Although aspiration and conservative management are clearly different, the safety profiles should be pretty similar, as neither approach leaves a chest tube in place to allow for the possibility of an expanding pneumothorax. Thus, although we cannot extrapolate to the speed of recovery, the safety of aspiration should be similar to the safety of conservative management.
The bigger question is which approach should be considered the standard of care. Conservative therapy was the standard of care until the 1940s, when intercostal catheters were adopted based only on expert opinion. (Kelly 2007) Although there has never been an RCT to prove that convservative therapy is as good as a chest tube (until now), that also means that there has never been an RCT that demonstrates that chest tubes are better than conservative care. However, there is lots of data that demonstrates that most patients will do fine without a chest tube. Like most medical practices, chest tubes are not parachutes. They clearly don’t result in massive absolute changes in mortality. They are, however, associated with multiple significant side effects. We shouldn’t just assume that they help, despite the historical tradition leading to their widespread use. Considering the available observational evidence that many patients do fine without chest tubes, and the invasive nature of the procedure, we really need an RCT proving that chest tubes actually help patients. It might make more sense to consider conservative therapy the standard of care, and think about the (lack of) evidence supporting invasive management.
Based on the observational evidence, I have always gravitated towards guidelines that suggest a more conservative approach. The British Thoracic Society guidelines allow for a little more observation than the American guidelines. (MacDuff 2010) However, I have preferred the Belgian Society on Pneumology guidelines, that define a pneumothorax as small as long as there is not dehiscence along the whole length of the lateral chest wall. In these patients, observation with outpatient follow-up is recommended. For large pneumothoraces, they recommend an aspiration first approach. (Leyn 2016) The European Respiratory Society guidelines suggest that measuring the pneumothorax is irrelevant. Instead, they suggest focusing on the patient’s symptoms, and “in selected patients with minimal or no symptoms and good access to medical care in case of deterioration, observation alone may be appropriate”. (Tscopp 2015) Therefore, conservative management is already part of guideline recommended care, and this study further supports that position.
You probably noticed that I listed a lot more secondary outcomes than I usually do. Although it is important to be cautious in interpreting secondary outcomes, I think they are important in this trial, as they suggest a trade off in benefits and harms between the conservative and aggressive management of spontaneous primary pneumothorax. On the one hand, the conservative group could have as much as a 8.6% lower chance of radiologic cure by 8 weeks. On average, the conservative group took about 2 weeks longer to be radiologically cured. Although that is a disease oriented outcome, it might matter if your pneumothorax occurred while travelling and you are trying to fly home. On the other hand, conservative management was at least as good in terms of symptoms (although the lack of blinding might affect subjective outcomes), had fewer adverse events, resulted in shorter hospital stays, and quicker returns to work. I think that is valuable information that can help make a shared decision.
As I said, I have long been comfortable with conservative management for these patients. I have been offering it as part of a shared decision making process for years (and patients almost always prefer the conservative approach). However, I have always been somewhat nervous about large pneumothoraces. In that respect, this study is incredibly helpful. It would have been much easier for these authors to focus on small pneumothoraces. It would have been easier to recruit patients to such a study, and including only small pneumothoraces would have guaranteed the non-inferior result. Instead, they took on the more difficult challenge and focused only on large pneumothoraces (32% or larger), providing us with the study we really needed. I was already comfortable doing nothing with small pneumothoraces. These aren’t definitive conclusions, but they represent the best current evidence to help guide shared decision making.
Of note, the protocol here is very different from what we do in Canada. If a patient needs a chest tube in Canada, the tube is placed, but they are almost always discharged home with the tube left in situ using a Heimlich valve. It is incredibly rare for these patients to get admitted to hospital, so the resource allocation calculation changes significantly. However, I have seen many patients over the years with numerous return ED visits because it is very painful to have a plastic tube wedged in your pleural space. I have also seen numerous complications (including empyema and significant subcutaneous emphysema) from these tubes. Those complications, rather than the inconvenience of a hospital admission, are the primary drivers in my decision making process.
Finally, we must ask what this trial says about the safety of a conservative approach. This trial is too small to make conclusions about rare adverse events, such as cardiovascular collapse from a tension pneumothorax. However, there is a fair amount of observational data available that indicates a less aggressive approach to pneumothoraces is safe. (Although those trials are also relatively small). Furthermore, there are numerous significant adverse events that can occur when placing a chest tube. My guess is that if we ran a large enough trial to assess rare but severe adverse events, they would be more common in the invasive management group.
Bottom line
This open-label RCT demonstrated that a conservative approach to primary spontaneous pneumothorax was non-inferior to invasive management. There are some limitations to this study, and conservative therapy is clearly not for every patient, but when combined with all the available data, I think it is clear that conservative management should at least be offered to stable, minimally symptomatic patients as part of a shared decision making process.
Other FOAMed
St Emlyn’s JC: Conservative management of pneumothoraces.
REBEL EM: Spontaneous Pneumothorax: Stand There and Do Nothing?
References
Baumann MH, Strange C, Heffner JE, et al. Management of Spontaneous Pneumothorax Chest. 2001; 119(2):590-602.
Brown SGA, Ball EL, Perrin K, et al. Conservative versus Interventional Treatment for Spontaneous Pneumothorax. The New England journal of medicine. 2020; 382(5):405-415. PMID: 31995686 [full text]
Delius RE, Obeid FN, Horst HM, Sorensen VJ, Fath JJ, Bivins BA. Catheter aspiration for simple pneumothorax. Experience with 114 patients. Archives of surgery (Chicago, Ill. : 1960). 1989; 124(7):833-6. [pubmed]
Johnson G. Traumatic pneumothorax: is a chest drain always necessary? Journal of accident & emergency medicine. 1996; 13(3):173-4. [pubmed]
Kelly AM. Review of management of primary spontaneous pneumothorax: is the best evidence clearer 15 years on? Emergency medicine Australasia : EMA. 2007; 19(4):303-8. [pubmed]
Kelly AM, Clooney M, . Deviation from published guidelines in the management of primary spontaneous pneumothorax in Australia. Internal medicine journal. 2008; 38(1):64-7. [pubmed]
Kelly A, Kerr D, Clooney M. Outcomes of Emergency Department Patients Treated for Primary Spontaneous Pneumothorax Chest. 2008; 134(5):1033-1036.
Leyn PD, Lismonde M, Ninane V, et al. Belgian Society of Pneumology. Guidelines on the management of spontaneous pneumothorax Acta Chirurgica Belgica. 2016; 105(3):265-267.
MacDuff A, Arnold A, Harvey J. Management of spontaneous pneumothorax: British Thoracic Society pleural disease guideline 2010 Thorax. 2010; 65(Suppl 2):ii18-ii31.
Mercier C, Page A, Verdant A, Cossette R, Dontigny L, Pelletier LC. Outpatient management of intercostal tube drainage in spontaneous pneumothorax. The Annals of thoracic surgery. 1976; 22(2):163-5. [pubmed]
Moore FO, Goslar PW, Coimbra R, et al. Blunt traumatic occult pneumothorax: is observation safe?–results of a prospective, AAST multicenter study. The Journal of trauma. 2011; 70(5):1019-23; discussion 1023-5. [pubmed]
Parlak M, Uil SM, van den Berg JW. A prospective, randomised trial of pneumothorax therapy: manual aspiration versus conventional chest tube drainage. Respiratory medicine. 2012; 106(11):1600-5. [pubmed]
Stradling P, Poole G. Conservative management of spontaneous pneumothorax. Thorax. 1966; 21(2):145-9. [pubmed]
Thelle A et al. Randomised comparison of needle aspiration and chest tube drainage in spontaneous pneumothorax. The European respiratory journal. 2017; 49(4). PMID: 28404647
Tschopp J, Bintcliffe O, Astoul P, et al. ERS task force statement: diagnosis and treatment of primary spontaneous pneumothorax Eur Respir J. 2015; 46(2):321-335.
Walker SP, Barratt SL, Thompson J, Maskell NA. Conservative Management in Traumatic Pneumothoraces Chest. 2018; 153(4):946-953.
Zehtabchi S, Rios CL. Management of emergency department patients with primary spontaneous pneumothorax: needle aspiration or tube thoracostomy? Annals of emergency medicine. 2008; 51(1):91-100, 100.e1. [pubmed]
Morgenstern, J. Conservative treatment for primary spontaneous pneumothorax, First10EM, February 24, 2020. Available at:
https://doi.org/10.51684/FIRS.11293



9 thoughts on “Conservative treatment for primary spontaneous pneumothorax”
My teaching was that a pnuemo gets a drain. The end.
But then – the teaching was focused entirely through the lens of trauma, and a prevalence of open chest wounds. I can’t say that I’ve seen a spontaneous pnuemo ever.
I feel like I need to go back to the absolute basics and re-evaluate everything I think I know about pneumo’s.
I’ve been an ER doc for 14 years and I’ve seen only 5-10 spontaneous pneumos in my life. I work in a populated suburban ER in California. They are rare. It seems from the authors wording that they are much more common where he works. For instance “numerous complications” from chest tubes for spontaneous pneumo I have never seen.
Note that the researchers used the “Collins method” to measure the pneumothorax size – this was based on a article by Rhea ( Rhea JT, DeLuca SA, Greene RE. Determining the size of pneumothorax in the upright patient.Radiology 1982:144:733-736).
Both studies compare the size of the lung in relation to the size of the thorax with labels B and C referring to the interpleural distance at the mid points of the upper and lower hemithoraces respectively, not the midpoints of the collapsed lungs, as used in the Brown study.
Using their method it is likely that the size of the pneumothorax would be underestimated for patients included in the Brown study, further highlighting the role of conservative management in “moderate” spontaneous pneumothoraces.