
Since my rather lengthy write up of the stroke literature, there have been new RCTs published looking at thrombolytics for acute ischemic stroke. No, we haven’t got the replication of NINDS that we so desperately need. However, the new trials do represent a step forward in our thinking about stroke: they use imaging to select a group of patients that might be more likely to benefit. When using thrombolytics for MI, we select the subgroup most likely to benefit by looking for ST elevation on the ECG. We don’t just give thrombolytics to everyone with chest pain, but that is basically our current approach to stroke. We throw lytics at anyone presenting with acute neurologic symptoms, and in that context, I don’t think it is surprising that our efforts thus far have been ineffectual. Although there are other differences between stroke and MI, I have always felt we were going to need to find a “STEMI equivalent” in stroke patients if thrombolytics were going to have any chance of success.
Yesterday, I reviewed the results of the WAKE-UP trial, which used an MRI pattern that suggests that the onset of stroke was less than 4.5 hours before the scan. (Thomella 2018) Although it uses advanced imaging, the WAKE-UP approach is really just a minor tweak of our current time-based paradigm.
Another candidate for a STEMI equivalent is the use of either CT perfusion or perfusion-diffusion MRI to try to identify patients who have evidence of ischemia, but salvageable brain tissue. There have been a few promising studies using this technique to guide thrombectomy out to 24 hours after symptom onset (which may need to be the focus of a future blog post). (Nogueira 2018, Albers 2018) There have also been a couple of negative trials looking at this imaging technique with thrombolytics.
The EPITHET trial was a phase 2 placebo-controlled RCT that screened patients who were 3-6 hours after the stroke symptom onset using perfusion-diffusion MRI and then randomized them to alteplase or placebo. They screened 3908 patients to find 101 eligible candidates. There was no difference in their primary outcome, which was a disease oriented imaging outcome. There was no statistical difference in mortality (26% with alteplase vs 12% with placebo in patients with perfusion mismatch; p=0.10). There was also no difference in good functional outcomes (45% vs 40% in the patients with mismatch, p=0.38). There was the expected increase in symptomatic ICH (7.7% vs 0%, stats not reported). Overall, the study was negative, but was clearly underpowered, and quite concerning for the large increase in mortality seen. (Davis 2008) In fact, it is a little surprising that phase 3 trials occurred after a phase 2 trial with a 14% increase in mortality.
The ECASS4-EXTEND trial was a multicentre, placebo controlled, double-blind RCT that also looked at a perfusion-diffusion MRI guided approach, enrolled patients who were 4.5 to 9 hours after symptom onset, and randomized them to alteplase of placebo. They were supposed to enroll 264 patients. After screening 232 patients, they managed to enroll 120, but then the trial was stopped early. They couldn’t recruit enough patients, because everyone was going for endovascular therapy. There were no statistically significant differences in anything in this trial, but once again it was under-powered. The neurologic outcomes were better in the tPa group (mRS 0-1 35% with tPa vs 26% with placebo, p=0.45), but a p value of 0.45 could be consistent with just about anything. Once again, mortality looks worse (11.5% vs 6.8%, p=0.53), but the confidence intervals are huge. (Ringleb 2019)
That brings us to the main topic of this blog post, the largest of these trials, the EXTEND trial…
The paper
The EXTEND Trial: Ma H, Campbell BCV, Parsons MW, et al. Thrombolysis Guided by Perfusion Imaging up to 9 Hours after Onset of Stroke. The New England journal of medicine. 2019; 380(19):1795-1803. PMID: 31067369 [full text] Clinicaltrials.gov: NCT00887328 and NCT01580839
The Methods
This is a multicentre, randomized, placebo controlled trial of perfusion imaging (either CT or MRI) to guide tPa in late ischemic strokes or patients with wake-up strokes.
Patients
Adult patients with excellent functional status at baseline (a modified Rankin score less than 2) who either presented 4.5 to 9 hours after the onset of their symptoms or had their stroke symptoms upon waking up. Patients had to have an NIHSS of 4-26 and hypoperfused but salvageable brain tissue detected on either CT or MRI perfusion imaging.
- Patients were excluded if the physician was considering endovascular thrombectomy and if they had any of the standard exclusions for thrombolytics.
Intervention
tPa (alteplase) 0.9 mg/kg, 10% as a bolus and the rest over 1 hour.
Comparison
Placebo.
Outcome
The primary outcome was a modified Rankin score (mRs) of 0 to 1 at 90 days.
Safety outcomes included death and symptomatic intracranial hemorrhage.
The Results
They planned to enroll 400 patients and later adjusted that down to 310. The trial was stopped early after 225 patients were enrolled because they thought the results of the WAKE-UP trial invalidated the equipoise of this trial. (Thomella 2018) The median NIHSS was 12 (more sick than WAKE-UP). 25% of the patients were enrolled between 6 and 9 hours, 10% between 4.5 and 6 hours, and 65% were enrolled because of a wake up stroke.
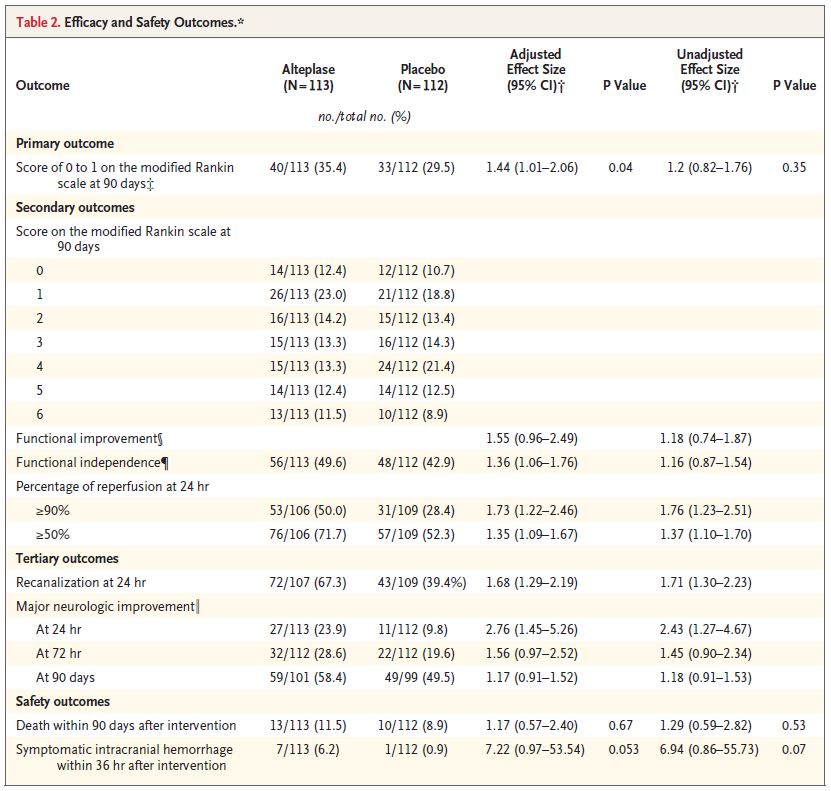
More people had a good neurologic outcome in the tPa group. Whether or not this was a statistically significant difference is unclear. The primary outcome of a mRs 0-1 occurred in 35.4% of the tPa group and 29.5% of the placebo group (adjusted OR 1.44; 95%CI 1.01 – 2.06, p=0.04). If instead of the adjusted analysis, you just do the stats on the raw numbers, the trial is not statistically significant (OR 1.2, 95% CI 0.82 – 1.76, p =0.35).
Unlike NINDS, there was actually an improvement in neurologic function at 24 hours in this trial. As defined by a drop of 8 or more on the NIHSS, 24% of the tPa group and 10% of the placebo group saw improvement (OR 2.43; 95%CI 1.27-4.67). Other secondary outcomes can be seen in the table below.
More people died in the tPa group, but it wasn’t statistically significant (11.5% vs 8.9%; adjusted OR 1.17, 95% CI 0.57-2.4; p=0.67).
There was predictably more symptomatic intracranial hemorrhage in the tPa group (6.2% vs 0.9%).
My thoughts
This is the second trial in a row demonstrating a potential benefit of using advanced imaging to guide the use of thrombolytics in ischemic stroke. I think this approach is promising, but unfortunately there are numerous problems with this trial that will hinder practice going forward.
Yesterday’s comments about stopping trials early apply to this trial as well and complicate the interpretation of the results. They stopped this trial because they claim that the results of WAKE-UP resulted in a loss of equipoise. That indicates that they believe that the WAKE-UP trial gives us a definitive scientific answer. I will let you read the WAKE-UP review again and decide for yourself, but I think there are many issues with WAKE-UP, including the fact that they never actually finished the trial, that mean we clearly needed more research. Stopping this trial early just robs us (and more importantly our patients) of some really important answers..
Furthermore, the imaging technique used in WAKE-UP was completely different from the one used in EXTEND, which makes any arguments about losing equipoise sort of silly. (The editorialist for this paper seems to agree with me.) (Marshall 2019) A p-value of 0.04, that only exists on an adjusted analysis, is always very suspicious for p-hacking. Furthermore, there is a small but potentially important increase in mortality, that we also saw in both of the other trials looking at this technique, that was guaranteed not to be statistically significant by ensuring the trial was under-powered for that outcome. Stopping trials early introduces significant bias, especially in a context where the author conflict of interest list is long.
Once again, this is a very select group of patients. They managed to enroll 225 patients from 27 hospitals over 8 years. That is only 1 patient a year at each hospital! Unlike the WAKE-UP trial, they don’t provide us with a proper flow diagram, nor do they tell us how many patients they screened to find those 225 patients. The results are almost certainly shaped by selection bias, and the tiny number of eligible patients limits the importance of these results. (If we are only going to be treating 1 patient a year, it doesn’t seem to make sense to invest in these advanced imaging techniques and the 24/7 neuroradiologists that will be required.)
The applicability of these trial results is further hindered by the massive change in stroke systems over the decade since this trial was designed. 80% of the patients in this trial had large vessel occlusions. In most centers, those patients will be managed with thrombectomy, meaning that these results apply to even fewer patients in 2020.
Depending on the column you read, this trial was both statistically significant (p 0.04) and not (p 0.35). Which number should you believe? There is a big statistical debate about whether RCT results should be adjusted or not. Randomization is supposed to balance the groups, so why would you subsequently adjust the results? On the other hand, you have lots of information about the baseline characteristics of the patients, so why wouldn’t you take that data into account? My problem with adjustments is that there are so many ways you can adjust data, you can make trials say almost anything you want. It gives researchers too much freedom (they can just keep trying different adjustments until they see a p value they like).
I think it is OK to do adjusted statistics if you are explicit about exactly how you are going to do the adjustment when the trial is registered so that the freedom to tinker is eliminated. The clinicaltrials.gov entry for this trial says nothing about adjustment. Their original protocol calls for a standard regression analysis, rather than the Poisson analysis they performed. They hide the results in the supplementary appendix, but much like the unadjusted numbers, the originally planned adjustment was not statistically significant (with a p value of 0.06). Therefore, I think you have to ignore the adjusted analysis, and look at the p value of 0.35 that comes with the raw numbers, or at the very least the p value of 0.06 that comes with their originally planned adjustments. This was a negative trial.
Looking through the secondary outcomes, we see the same trend. Many were statistically significant after being adjusted, but not so if you use the raw numbers. However, the general trend was that all of these numbers were better in the tPa group. Also, unlike all prior studies, they actually saw an improvement at 24 hours with tPa. I think that is important moving forward, because it was always somewhat biologically implausible that tPa could have no effect at 24 hours but somehow magically improve outcomes at 90 days (which is what NINDS seems to tell us).
Although I think the use of advanced imaging to guide thrombolysis in ischemic stroke is promising, there are important harms to be considered. Perhaps the biggest is time. The average door to needle time in this trial was 2 hours, which is much slower than guideline recommended care. These advanced studies take time to perform and read, so we need to be sure they are helping our patients before they are widely deployed. This is why a 3 pronged replication of NINDS, which compares both time based and imaging based strategies to placebo, would be ideal.
These studies should move us further away from the “time is brain” conceptualization of stroke management. The concept of a 3 hour or 4.5 hour cutoff for treatment was probably always based on a retrospective Texas sharpshooter interpretation of the literature. The Cochrane review concludes that the available data does not support a difference between the 0-3 hour and 3-6 hour groups. (Wardlaw 2009) There is a glaring contradiction in the current stroke world. On the one hand, people are still arguing that time is incredibly important, which is why we need to ignore every trial except NINDS and ECASS3. On the other hand, the EXTEND and WAKE-UP trials, as well as the numerous endovascular trials that have included patients far beyond the traditional stroke time windows, indicating that time is not the true arbiter of treatment success.
Our approach to ischemic stroke thus far has been a lot like giving every chest pain patient thrombolytics. Physiologically, it makes sense that lytics could help in ischemic stroke, but we need to find the right subset of patients; we need to find our STEMI equivalent.
The debate about thrombolytics in stroke has spent far too long stuck in a dichotomous “they work” versus “they don’t work” argument. It is almost certainly more complicated than that. The literature makes it clear that tPA causes significant harm when given to patients with ischemic stroke. Bleeding increases, and mortality probably does as well. However, there are also hints in the data that thrombolytics might improve neurologic outcomes. The damage from this debate over the past 30 years is that, in polarizing the two sides, it has prevented the necessary follow up research that might identify appropriate subgroups who actually benefit from thrombolytics.
Bottom line
In this small trial that was stopped early, the small improvement in neurologic outcomes seen with tPa was probably not statistically significant, and only applies to a very small number of patients. This approach probably also increases mortality. I think the use of advanced imaging to guide tPa is promising (especially among patients presenting in the first 3 hours), but we clearly need more research.
Other FOAMed
Thrombolytics for stroke: The evidence
REBEL EM – Extending the tPA Window to 4.5 – 9 Hours in Acute Ischemic Stroke (AIS)?
EM NERD – The Case of the Magician’s Sleight
EM Lit of Note – EXTEND Alteplase Shenanigans!
References
Albers GW, Marks MP, Kemp S, et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. The New England journal of medicine. 2018; 378(8):708-718. [pubmed]
Davis SM, Donnan GA, Parsons MW, et al. Effects of alteplase beyond 3 h after stroke in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET): a placebo-controlled randomised trial. The Lancet. Neurology. 2008; 7(4):299-309. [pubmed]
Ma H, Campbell BCV, Parsons MW, et al. Thrombolysis Guided by Perfusion Imaging up to 9 Hours after Onset of Stroke. The New England journal of medicine. 2019; 380(19):1795-1803. PMID: 31067369
Marshall RS. Image-Guided Intravenous Alteplase for Stroke – Shattering a Time Window. The New England journal of medicine. 2019; 380(19):1865-1866. [pubmed]
Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. The New England journal of medicine. 2018; 378(1):11-21. [pubmed]
Ringleb P, Bendszus M, Bluhmki E, et al. Extending the time window for intravenous thrombolysis in acute ischemic stroke using magnetic resonance imaging-based patient selection. International journal of stroke : official journal of the International Stroke Society. 2019; 14(5):483-490. [pubmed]
Thomalla G, Simonsen CZ, Boutitie F, et al. MRI-Guided Thrombolysis for Stroke with Unknown Time of Onset. The New England journal of medicine. 2018; 379(7):611-622. PMID: 29766770
Wardlaw JM, Murray V, Berge E, del Zoppo GJ. Thrombolysis for acute ischaemic stroke. Cochrane Database of Systematic Reviews 2009, Issue 4. Art. No.: CD000213. DOI: 10.1002/14651858.CD000213.pub2.
Morgenstern, J. Stroke thrombolytics update 2: The EXTEND trial, First10EM, January 28, 2020. Available at:
https://doi.org/10.51684/FIRS.10784



4 thoughts on “Stroke thrombolytics update 2: The EXTEND trial”
Thrombolytics may work in selected patients but we don’t really have a good way of selecting patients. We don’t know the physiologic mechanism behind this possible improvement (why is there no change at 24 hours?). Very few patients will ever get selected.
If they work they don’t work very well. Analyzed in terms of QALYs or DALYs (the only valid measures) thrombolytics are essentially irrelevant compared to boring things like swallow studies and rehab. It’s just a rabbit hole.
I don’t think the analogy of giving lytics to every chest pain is like how we treat stroke…for chest pain we use ST changes to guide therapy as you say and for stroke we use the NIHSS/clinical exam. The exam allows us to localize the brain vascular lesion just like ST changes in contiguous leads allows you to localize the cardiac vascular lesion. If a patient has RUE weakness with LLE weakness that does not correlate with any vascular territory so that patient does not get shot gun TPA w a negative CT just like a patient w ST changes in non contiguous leads would not immediately activate a cath lab…
The problem with that argument is that NIHSS / clinical exam have not been shown to correlate with benefit from treatment like ST elevation has. We do the same kind of assessment you are talking about with chest pain. We use clinical exam and history to distinguish chest pain that sounds like PE and chest pain that sounds like ACS. The current approach to stroke is very much like giving thrombolytics to every patient that sounds like they have ACS based on the clinical exam, which would be disastrous.