Over the last month, normal blog content has taken a back seat to the COVID pandemic. I will continue to update the COVID resources, and write about new studies as they come out, but I think it is about time that we got back to regular content. Let’s start with a post I wrote a few months ago about hypothermia for cardiac arrest. There was a big new RCT looking at hypothermia for cardiac arrest last year. However, before tackling that paper, I thought it would be worthwhile to review the 3 prior studies, and perhaps explain my skepticism about the idea that cooling brains could save lives.
The practice of hypothermia for cardiac arrest was born out of two RCTs in 2002. At that point, I hadn’t even applied for medical school yet, so I did not apply my skeptical thinking to the papers in real time. Although our thinking has been fundamentally reshaped by these two trials, I think it is worth considering the results we might have predicted in 2001. Hypothermia is supposed to decrease cerebral oxygen demands, which is supposed to help alleviate the ischemia that occurs after cardiac arrest. My guess is that most of the damage is done during the low flow state of cardiac arrest itself, in which case hypothermia could not possibly help, but there is some degree of persistent ischemia in the hours after the arrest, which is the target of hypothermia. Unfortunately, most novel medical interventions don’t work. As compared to a medication or a surgical procedure, I personally think that hypothermia is less likely to work, so my pretest probability for the 2002 trials would probably have been quite low. However, there were animal studies prior to 2002 suggesting benefit, which should probably increase our pretest probability, but not by too much, as animals studies often don’t translate into human results. (Bernard 2002) All things told, if you offered me a bet in 2001, I would have bet against these trials showing a benefit.
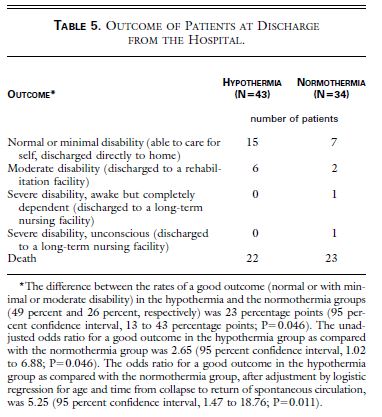
The RCT from Bernard and colleagues randomized 84 patients with an initial cardiac rhythm of ventricular fibrillation who had achieved return of spontaneous circulation (ROSC) but were persistently comatose. (Bernard 2002) 7 patients were subsequently excluded, leaving 77 to be analyzed. The trial was not truly randomized, as they assigned patients based on the day of the month, which is a major potential source of bias. (If you are a fan of hypothermia, you might exclude older patients with multiple comorbidities, or other poor prognostic factors, on the days that you know that they would be assigned to receive hypothermia. They don’t tell us how many people were screened to find those 84, so selection bias is also a significant possible problem.) The trial isn’t blinded, which makes sense considering the intervention, but also increases the chance of bias. Cooling in this study was achieved by ice packs. The target was 33 degrees Celsius, and patients were kept at 33 degrees until 12 hours after hospital arrival, at which point they were actively rewarmed using a heated-air blanket over 6 hours. The primary outcome, patients with neurologic function good enough to be sent home or to a rehab facility, occured in 49% of the hypothermia group and 26% of the normothermia group (p=0.046, although when I plug the numbers into a fragility index calculator, you get a fragility index of 0 and a p value of 0.06). Mortality was not statistically significant (51% vs 68%, p=0.16).
Bottom line: This is a small trial at high risk of bias with a borderline statistically significant result. The absolute difference is impressive and definitely warrants further research, but could easily be explained by bias in the trial design rather than a true difference.
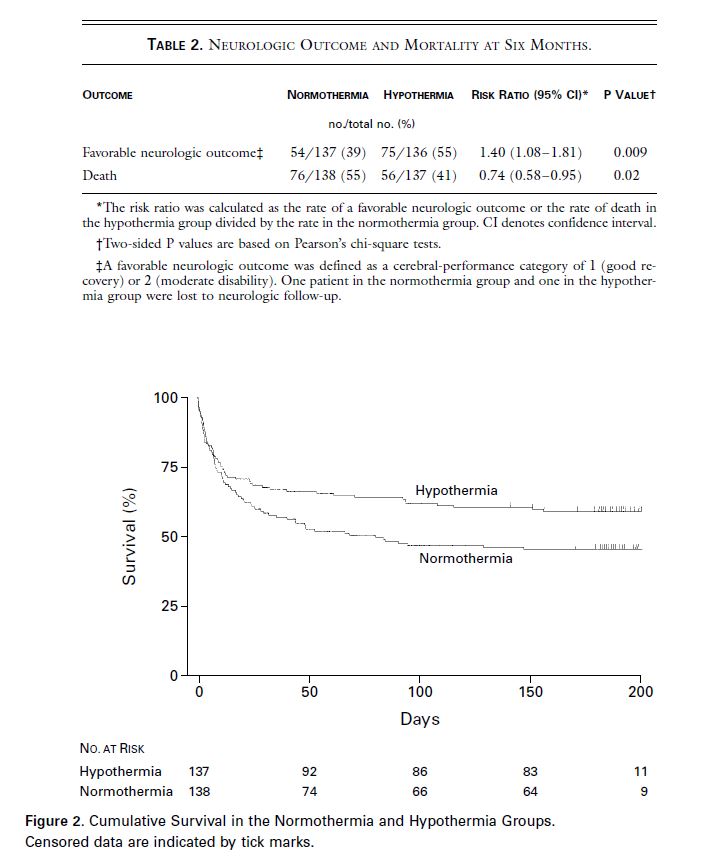
The other RCT, published in the same edition of the New England Journal of Medicine by the Hypothermia After Cardiac Arrest study group, randomized 275 comatose adult patients (out of 3551 screened) with ROSC after a witnessed cardiac arrest with a shockable rhythm, a presumed cardiac origin of arrest, and a short downtime. (HACA 2002) (They don’t actually tell us how they arrived at this sample size, but they say enrollment was slower than expected, and they ended the trial because they ran out of money rather than because they reached the expected sample size.) This trial was properly randomized. Again, doctors and patients weren’t blinded, but outcome assessors were. The hypothermia group was cooled using an external device to a target temperature between 32 and 34 degrees Celsius and maintained there for 24 hours followed by an 8 hour passive rewarming. The primary outcome was a good neurologic outcome within 6 months, based on a Pittsburgh cerebral-performance score, and occured in 55% of the hypothermia group and 39% of the normothermia group (p=0.009, RR 1.40, 95% CI 1.08-1.81). Six month mortality was also improved in the hypothermia group (41% vs 55%, p=0.02).
Bottom line: This trial is more convincing than the Bernard trial. It is still a relatively small trial, with some significant potential sources of bias, but based on these results it seems reasonable to adopt the intervention while waiting for more research.
This was the point in time that I entered medicine. Hypothermia was the rage. As a clerk, I was frequently sent rushing for ice packs. But after reading these papers, I had my doubts. The difference was big enough that I certainly went along with the guidelines, but based on these studies I felt there was still a very good chance that hypothermia was ineffective.
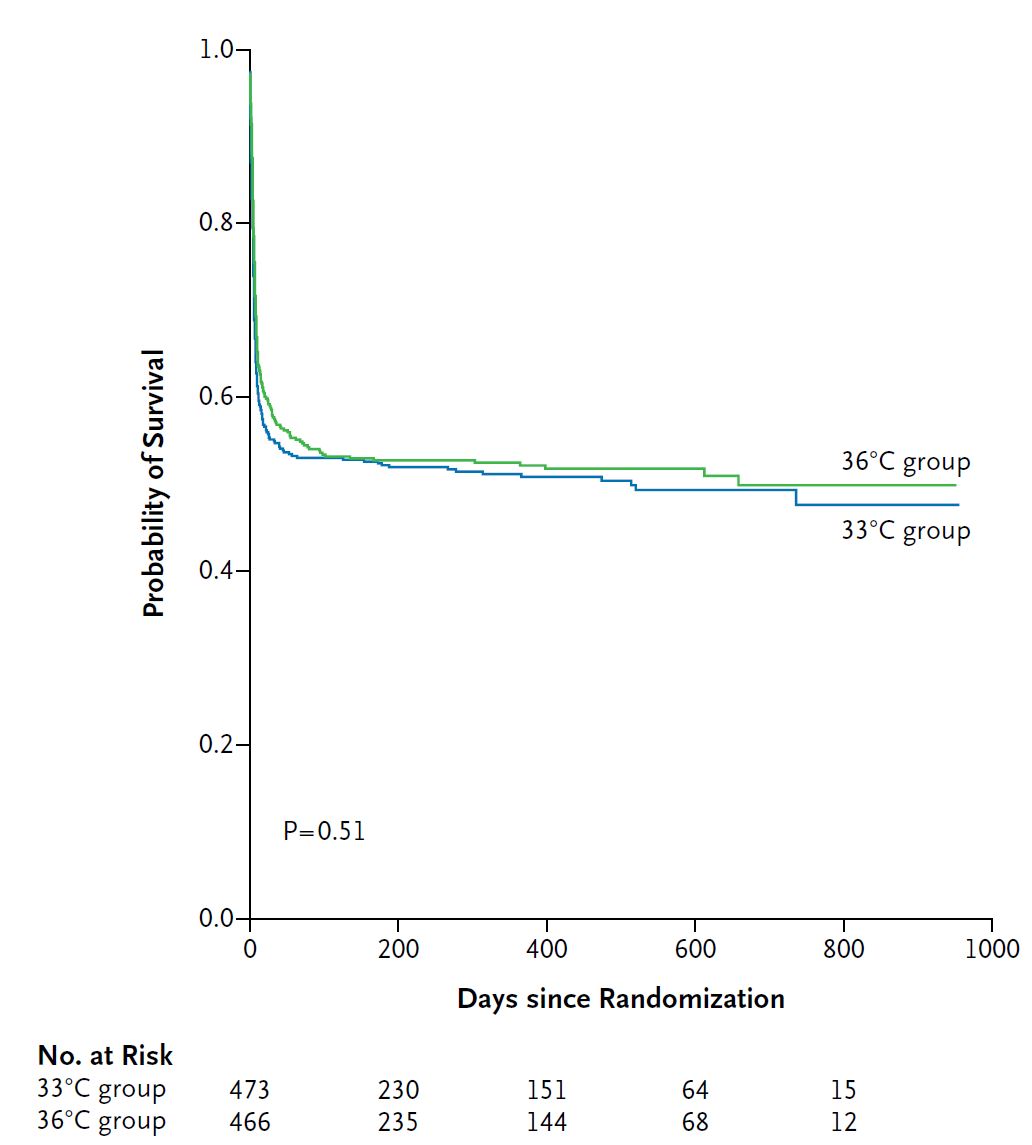
Which brings us to the TTM trial. (Nielson 2013) This is a multicentre RCT from 36 ICUs in Europe and Australia, which enrolled 950 comatose adult patients on arrival to hospital after out of hospital cardiac arrest, regardless of the presenting rhythm. The patients were randomized to a target temperature of either 33 or 36 degrees Celsius for 28 hours with mandatory sedation. The patients and treating physicians were not blinded, but the physicians performing neurologic prognostication and the outcome assessors were. This was a relatively select group of cardiac arrest patients, with 90% being bystander witnessed and 75% getting bystander CPR, which matters when trying to extrapolate the numbers to all comers. They enrolled all rhythms, but 80% of the patients enrolled had a shockable rhythm. There was no difference in the primary outcome of death at the end of the trial (50% vs 48%, p=0.51). There was also no difference in neurologic outcomes. The survivors essentially all had great neurologic outcomes in both groups, which seems different from other cardiac arrest research, such as PARAMEDIC 2.
Bottom line: In the largest, highest quality RCT to date, there was no difference between the hypothermia and normothermia (or very mild hypothermia) groups.
So what exactly does the TTM trial mean? There are a few possible interpretations. Perhaps my doubts were correct: the results of the earlier studies were born in bias or fluke, and hypothermia never worked at all. Obviously, I was biased towards that interpretation, but there are a few other possible interpretations of this data. The first 2 trials only included patients with shockable rhythms, so maybe the inclusion of all comers was the problem with TTM. (This seems unlikely, as 80% of the patients still had shockable rhythms.) The more popular interpretation seems to be the avoidance of fever theory. Both groups in the TTM trial had their temperatures tightly regulated. Unlike the first 2 trials, the normothermia group was not allowed to become febrile. There has always been a lot of observational data suggesting fever is bad in critically ill patients, so perhaps the benefit seen in the earlier hypothermia trials was all the consequence of avoiding fever.. (However, association is not causation. There is not, as far as I know, any RCT data demonstrating that controlling fever actually improves outcomes. In fact, there are multiple RCTs, and treating fever in the ICU does not provide any benefit – although treating fever is somewhat different from preventing it altogether.) (Young 2019) The fever hypothesis is a reasonable theory, but it certainly isn’t proven fact.
To complete our evidence review, there are also a couple RCTs looking at prehospital hypothermia. Bernard and colleagues randomized 234 adult patients with an out of hospital VFib arrest to either have their cooling start in hospital or in the ambulance. The ambulance based cooling got patients colder faster, but had no effect on outcomes, although the trial was stopped early and may have been underpowered. (Bernard 2010) Kim and colleagues randomized 1359 adult prehospital patients with ROSC after out of hospital cardiac arrest to prehospital cooling (accomplished by infusing 2 L of 4 degree saline) or standard care. (Kim 2014) Although prehospital cooling reduced core temperature and got patients to the target termerapture faster, there was no change in mortality or neurologic outcomes. Going back to physiologic reasoning, hypothermia is supposed to help with ischemia, and you would think this period immediately after arrest would be the most important. However, it appears that starting hypothermia earlier provides no benefit. Given that fever develops later after arrest, these results could be consistent with the avoidance of fever theory, but are also consistent with the theory that hypothermia just doesn’t work.
Which brings us to the new study published in 2019:
The paper
The HYPERION Trial: Lascarrou JB, Merdji H, Le Gouge A, et al. Targeted Temperature Management for Cardiac Arrest with Nonshockable Rhythm. The New England journal of medicine. 2019; 381(24):2327-2337. PMID: 31577396 [full text] NCT01994772
The Methods
This is an open-label, pragmatic, multi-centre RCT based in 25 ICUs in France.
Patients
Adult patients with a cardiac arrest (both in and out of hospital) with a non shockable cardiac arrest from any cause who remained comatose after ROSC.
- Exclusions: More than 10 minutes without CPR (“no flow time”), more than 60 minutes of CPR (“low flow time”), major hemodynamic instability (defined as epinephrine or norepinephrine requirement of more than 1 mcg/kg/min), longer than 300 minutes from arrest to randomization, moribund condition, pregnancy, breastfeeding, lack of health insurance.
Intervention
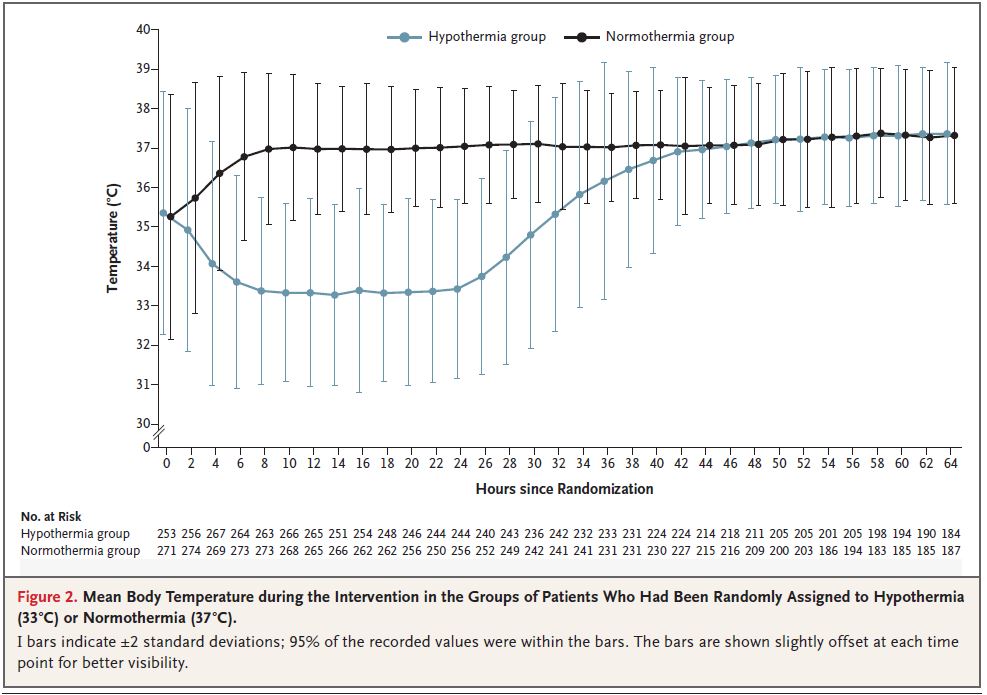
A target temperature of 33 degrees Celsius for 24 hours then slow rewarming, then a target temperature of 36.5 to 37.5 Celsius for 24 hours.
Comparison
Targeted normothermia of 36.5 to 37.5 degrees Celsius for 48 hours.
Other treatment
Although the trial is pragmatic, they did standardized treatment of several variables, including sedation and paralysis.
Outcome
The primary outcome was survival with a favourable neurologic outcome at 90 days (defined as a Cerebral Performance Category (CPC) of 1 or 2).
The Results
They enrolled 584 patients, 581 of which are included in the final analysis. They screened 2723 patients who met the inclusion criteria to find those 584.
About 75% of the arrests were out of hospital, thus the other 25% were in hospital. The cause of the arrest was noncardiac in ⅔ of patients. The most common cause of death was withdrawal of life support (62% in the hypothermia group and 65% in the normothermia group).
The cooling clearly worked, but unfortunately a large number of patients in the “normothermia” group actually developed a fever.
The primary outcome, survival with good neurologic outcome, occurred in 10.2% of the hypothermia groups and 5.7% of the normothermia group (absolute difference 4.5%, 95% CI 0.1-8.9%, p=0.047, fragility index = 1).
Mortality was not statistically different (81.3% vs 83.2%).
My thoughts
Before this trial was published, I was unsure about the utility of hypothermia. Were the previous positive results real? Is fever avoidance the only important intervention? This trial tells us that the rhythm (shockable versus non-shockable) is probably irrelevant, but still leaves us with a lot of questions.
Like many trials, they had to screen many more patients than were actually included in the trial, which results in potential selection bias. Some of the exclusion criteria, such as “moribund condition” and “for logistical reasons” are quite subjective. However, allocation concealment was appropriate in this trial, so the selection bias is more a concern for the generalizability of these results, rather than producing a systemic imbalance between the two groups. The inclusion of in-hospital cardiac arrest patients also affects generalizability to emergency department patients.
Although the results are statistically significant, they may not be replicable. The p value for the primary outcome was just barely below our standard cut off of 0.05. A single patient with a different outcome would have made the results of the trial statistically insignificant. That is especially important considering that the neurologic outcomes were based on phone interviews and the patients and their family members were not blinded to their treatment group. As was discussed in the review of thrombolytics for stroke, cerebral performance scores are not reliably reproduced when repeated by different interviewers. This introduces significant potential for bias and makes the results less reliable.
The cause of death in almost ⅔ of patients was withdrawal of life support. The decision to withdraw care can have a major impact in any cardiac arrest trial. If physicians are too pessimistic, we may withdraw care before any benefit from treatment can be seen. In the TTM trial, they blinded the doctor performing neuroprognostication, which should help. In HYPERION, the physicians making end of life decisions were not blinded to the patient’s study group, which could have biased the outcomes. For example, after noticing that they patient did not receive hypothermia, the physician might lower their prognosis, increasing the chance of withdrawal of life support. Life support withdrawal was a slightly more common cause of death in the normothermia group (65.2% vs 61.9%), which, considering the fragility index of 1, could easily have impacted the results.
So what do the results of the HYPERION trial mean? Given the limitations, it is hard to know for sure. I am slightly less skeptical of hypothermia overall than I was before the trial was published. This trial, like the 2 positive trials before it, certainly doesn’t provide definitive evidence that hypothermia helps. It still isn’t clear whether you actually need to be mildly hypothermic, or simply avoid fever. I will continue to follow my institution’s hypothermia protocol, and maybe the addition of one more ‘positive trial’ will make me feel marginally more optimistic about this management strategy.
Bottom line
The HYPERION trial adds to the evidence that strict temperature control (and possibly mild hyperthermia) results in better outcomes for comatose cardiac arrest patients. It is the first trial to focus specifically on patients with non-shockable rhythms. It doesn’t provide us with definitive evidence, but until we see more data, it seems like all comatose cardiac arrest patients with ROSC should have their temperature controlled, and that the target should be between 33 and 36 degrees Celsius, not 37.
Other FOAMed
EMCrit: The Targeted Temperature Trial Changes Everything and Five Minutes with Jon Rittenberger on the TTM Trial
The SGEM: Baby It’s Cold Outside (Pre-hospital Therapeutic Hypothermia In Out Of Hospital Cardiac Arrest) and Ice, Ice, Baby (Hypothermia Post Cardiac Arrest)
St. Emlyn’s: What’s the target temperature for OOHCA cooling?
REBEL EM: HYPERION: Targeted Temperature Management in Cardiac Arrest Patients with Non-Shockable Rhythms and Does Targeted Temperature Management Actually Work?
PulmCrit: Hypothermia for non-shockable arrest: let’s not get hot-headed about this and Top 10 reasons to stop cooling to 33C
A massive thank you to our supporters for helping to keep First10EM running. Maria Vanessa Serrano Borraz, Andrew Bonnell, André Johansson, Christy McKenzie, David Zira, Michael Hall, Michael Obiako, Peter Tagmose Thomsen, Sarra Keene, Tim LaBelle, Zachary Aust, Carla Sterling, Conal Roche, Craig McLean, Juri Katchanov, Kasemsuk Yothasamutr, Mark Hauswald, Pietro Pettenella, Rebekah, Salil Elias, Simon Olewicz, Thomas Arnold Wade, Tim Kleffner – you are all amazing! Thank you!
References
Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. The New England journal of medicine. 2002; 346(8):557-63. [pubmed]
Bernard SA, Smith K, Cameron P, et al. Induction of therapeutic hypothermia by paramedics after resuscitation from out-of-hospital ventricular fibrillation cardiac arrest: a randomized controlled trial. Circulation. 2010; 122(7):737-42. [pubmed]
HACA – Hypothermia After Cardiac Arrest study group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. The New England journal of medicine. 2002; 346(8):549-56. [pubmed]
Kim F, Nichol G, Maynard C, et al. Effect of prehospital induction of mild hypothermia on survival and neurological status among adults with cardiac arrest: a randomized clinical trial. JAMA. 2014; 311(1):45-52. [pubmed]
Lascarrou JB, Merdji H, Le Gouge A, et al. Targeted Temperature Management for Cardiac Arrest with Nonshockable Rhythm. The New England journal of medicine. 2019; 381(24):2327-2337. [pubmed]
Nielsen N, Wetterslev J, Cronberg T, et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. The New England journal of medicine. 2013; 369(23):2197-206. [pubmed]
Young PJ, Bellomo R, Bernard GR, et al. Fever control in critically ill adults. An individual patient data meta-analysis of randomised controlled trials. Intensive care medicine. 2019; 45(4):468-476. PMID: 30741326
Morgenstern, J. Hypothermia for cardiac arrest, First10EM, April 20, 2020. Available at:
https://doi.org/10.51684/FIRS.12583



3 thoughts on “Hypothermia for cardiac arrest”