
It’s that time again. A roundup of the most interesting emergency medicine articles I have read in the last few months.
If epinephrine doesn’t work, what makes you think calcium would be any better?
Vallentin MF, Granfeldt A, Meilandt C, et al. Effect of Intravenous or Intraosseous Calcium vs Saline on Return of Spontaneous Circulation in Adults With Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA. 2021 Nov 30. doi: 10.1001/jama.2021.20929. PMID: 34847226
This is an RCT looking at the empiric use of calcium in out of hospital cardiac arrest. The trial was stopped early, after enrolling 383 patients, on the recommendation of the independent safety committee because it looked like calcium is actually harmful. The trial compared 5 mmol of calcium chloride given immediately after the first and second doses of epinephrine to a normal saline placebo in adult cardiac arrest patients. They excluded patients with a clinical indication for calcium, such as hyperkalemia. The primary outcome, return of spontaneous circulation, occurred in 19% of the calcium group and 27% of the placebo group (RR 0.72, 95%CI 0.49-1.03, p = .09). Survival and survival with good neurologic outcomes were also lower with calcium, but not statistically so. Although the study is imperfect, I think it is pretty clear evidence against using calcium empirically in patients without an indication for calcium. I should note that only 1 patient out of 1221 screened was excluded because the clinician thought calcium was clinically indicated, so this should not be a common excuse for prescribing calcium. (And that makes sense to me, as I almost never give calcium in my arrests, but it could vary depending on your patient population.)
Bottom line: We should not be using calcium empirically for out of hospital cardiac arrest, but be mindful of specific indications.
2022 and we still got nose danglers
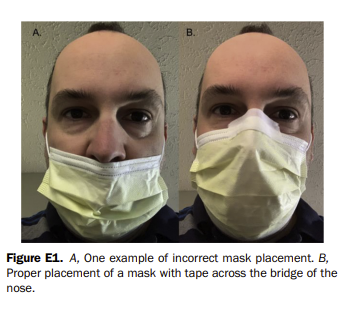
Pettit N, Zaidi A, O’Neill B, Doehring M. Use of Adhesive Tape to Facilitate Optimal Mask Positioning and Use in the Emergency Department: A Randomized Controlled Trial. Ann Emerg Med. 2021 Aug 2:S0196-0644(21)00479-0. doi: 10.1016/j.annemergmed.2021.06.004. PMID: 34353646
Masks work, but only if they are actually worn. At any given moment in the emergency department, I would be very surprised if even half of patients were wearing their masks correctly. This is an open-label RCT looking at improving compliance with proper masking. 123 emergency department patients were randomized to either have a piece of tape placed over the bridge of their nose to the top of the mask, or to have no intervention. The patients were then checked at 1 hour by the research team, and 100% of the tape group had proper mask placement as compared to only 69% of the no intervention group (absolute risk reduction 31%, 95%CI 19-43%, NNT=3.2). Harms are not reported, but should be minimal. Although this is a small, open-label study with a convenience sample of patients, the intervention is so simple and the benefit so large that this should probably be implemented widely right now. Send this article to all your triage nurses and front of house staff.
Bottom line: A simple intervention using tape on the nose may dramatically increase proper mask use among patients.
Longer is not always better in urology
Drekonja DM, Trautner B, Amundson C, Kuskowski M, Johnson JR. Effect of 7 vs 14 Days of Antibiotic Therapy on Resolution of Symptoms Among Afebrile Men With Urinary Tract Infection: A Randomized Clinical Trial. JAMA. 2021 Jul 27;326(4):324-331. doi: 10.1001/jama.2021.9899. PMID: 34313686
When it comes to evidence based medicine and antibiotics, it seems like less is always more. However, when it comes to males and urinary tract infections, guidelines always seem to suggest more and more and more. This is a double blind non-inferiority RCT that looked at 272 men with afebrile UTIs, and randomized them to receive antibiotics (ciprofloxacin or trimethoprim/sulfamethoxazole) for either 7 or 14 days. I think the non-inferiority margin of 10% is way too wide (and will write more in the future about why we really need to stop using so many non-inferiority trials), but it doesn’t seem to have mattered. In the per-protocol group, 93% of the 7 day group and 90% of the 14 day group had symptom resolution. (It was 92% vs 91% in the ITT analysis). There was no difference in recurrence, which if anything looked to be a little less in the 7 day group (10% vs 13%). Adverse events were also not different, but also a little lower in the 7 day group. They don’t specifically discuss prostatitis, but did include patients with pyelonephritis symptoms. It is worth noting that this is a group of patients with relatively complex sounding UTIs. 60% had some sort of urinary co-morbidity, including prostate cancer, prior UTIs, incontinence, and even prior prostatitis in 12%. A urologist once taught me that all men with UTIs actually have prostatitis. I am not sure that is correct, and this is one of the only conditions that I find a rectal exam adds some value. I will decrease my routine antibiotic prescription in males with UTIs, but if I officially make the diagnosis of prostatitis, I will probably still be tempted to go with a longer course.
Bottom line: This non-inferiority RCT demonstrates that a 7 day course of antibiotics is probably just as good as a 14 day course in afebrile male patients with UTIs.
We are probably not using enough buprenorphine
Herring AA, Vosooghi AA, Luftig J, Anderson ES, Zhao X, Dziura J, Hawk KF, McCormack RP, Saxon A, D’Onofrio G. High-Dose Buprenorphine Induction in the Emergency Department for Treatment of Opioid Use Disorder. JAMA Netw Open. 2021 Jul 1;4(7):e2117128. doi: 10.1001/jamanetworkopen.2021.17128. PMID: 34264326
At this point, there is no doubt that the initiation of buprenorphine is a core emergency medicine skill. (If this is something you are still uncomfortable with, or are still faced with red tape, now is the time to get that fixed.) Instead of whether we should start this life saving therapy, the question is now: what is the best approach? The low dose initiation protocols that many EDs have adopted were actually developed in office-based settings, and therefore may not be appropriate for our patient population. Many patients with opioid use disorder require much higher buprenorphine doses than the typical 8-12mg limit used in these protocols. Therefore, many emergency departments are trying higher dose (>12mg) buprenorphine inductions. This is a chart review from a single institution looking at the safety and tolerability of their high dose buprenorphine strategy, which includes a dose option of up to 32mg. The dosing of buprenorphine could be done in increments of 4 to 8 mg or with the full 24 mg at once, depending on the patient’s level of withdrawal. (The protocol is below.) Specialty consultation was suggested for recent methadone use, anticipated surgery, receipt of long-term opioid therapy for pain, intoxication with alcohol, benzodiazepines, or other sedatives, post-overdose reversal with naloxone, chronic pulmonary disease, or serious acute illness and/or organ failure. Unfortunately, I imagine many of us will not have this specialty expertise available, and will have to act as our own experts. Over a 1 year period, this department provided buprenorphine to 391 patients with 579 ED visits. They used the high dose protocol 63% of the time, including 138 doses greater than or equal to 28mg. There were no differences in vital signs, adverse events, or vomiting based on dose. 5 patients (0.8%) had precipitated withdrawal. 4 of the 5 had withdrawal after the initial dose, and so it was unrelated to the high dose regimen, and the withdrawal was simply treated with more buprenorphine. Return visits, hospitalizations, and length of stay all appear to be unrelated to buprenorphine dose. We should obviously be cautious about the results of any chart review, and these numbers seem to indicate that this hospital has a lot more expertise in managing opioid use disorder than many of us. Furthermore, these results can’t actually demonstrate a benefit of the higher dose, but the assumption is that many of the patients needing higher doses would have been inadequately treated in other EDs.
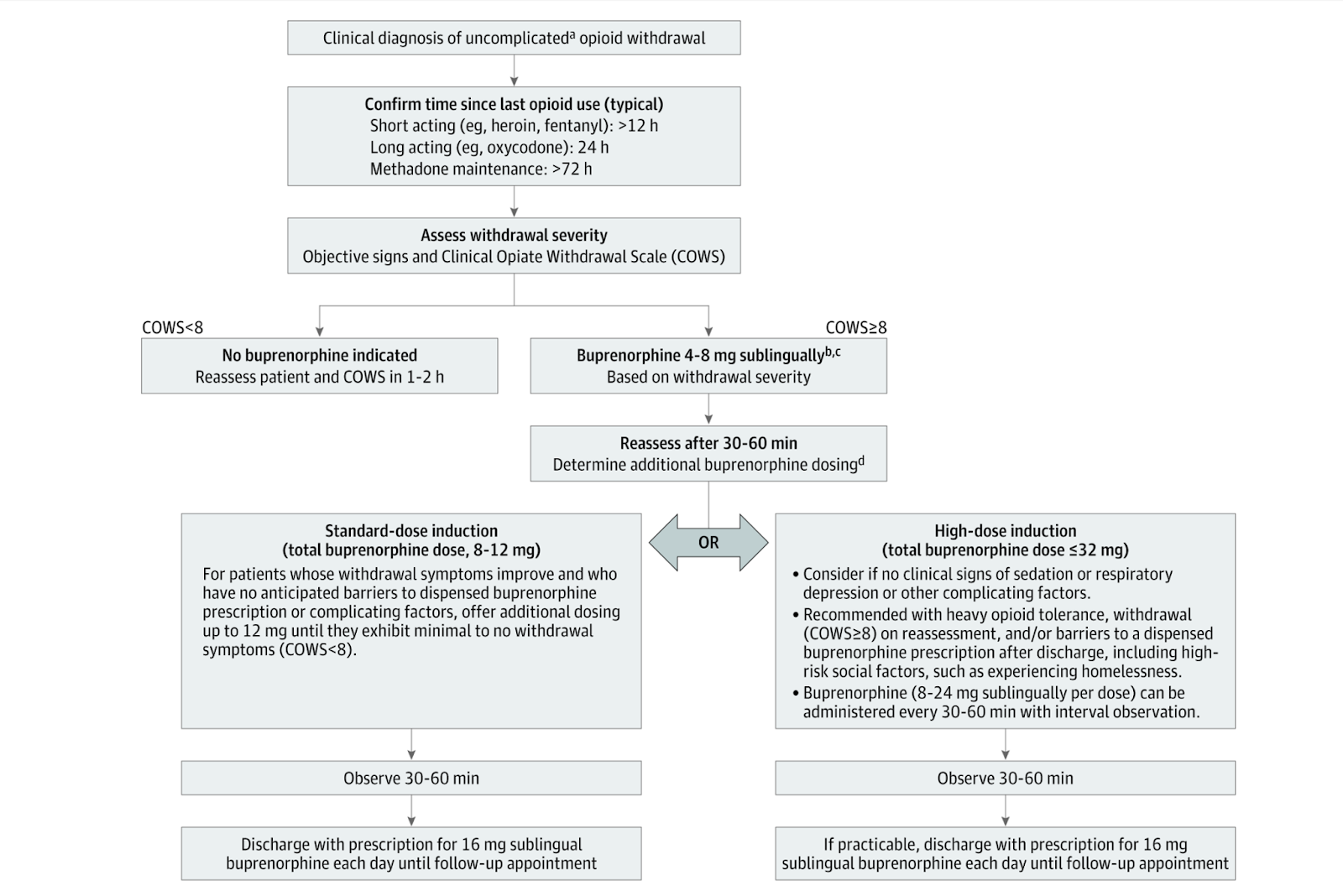
Bottom line: It appears to be safe to use higher doses of buprenorphine in the emergency department when managing opioid use disorder.
CBT for IBS
Buffone A, Goldman RD. Cognitive-behavioural therapy for children with irritable bowel syndrome. Can Fam Physician. 2021 Dec;67(12):905-907. doi: 10.46747/cfp.6712905. PMID: 34906937 [free full text]
The chronic management of children with irritable bowel syndrome may not be within the stated purview of emergency medicine, but children with chronic abdominal pain certainly spend a lot of time in the emergency department. When managing symptoms of IBS, I imagine most emergency doctors resort to something they can write on a prescription pad, but this paper reminds us that cognitive behavioural therapy should probably be a cornerstone of treatment. A Cochrane review found an 87% reduction in abdominal pain with 1 month of CBT (from 15 episodes of pain monthly down to 2), as compared to only a 33% reduction in the control group. Even if these small studies exacerage the benefits by a factor of 3, the effect is still large. The big problem I will face in Ontario is finding CBT for children, especially those who can’t afford to pay for it privately. Virtual care might alleviate some of these issues, and this paper specifically notes that internet based CBT is effective in children with IBS.
Bottom line: Consider a referral for CBT in children meeting the diagnostic criteria for IBS.
I love my Raptors (do you think I can get a sponsorship deal with the company?)
Walter J, DeBoer M, Koops J, Hamel LL, Rupp PE, Westgard BC. Quick cuts: A comparative study of two tools for ring tourniquet removal. Am J Emerg Med. 2021 Aug;46:238-240. doi: 10.1016/j.ajem.2020.07.039. Epub 2020 Jul 25. PMID: 33046320
This paper was talked about in a recent EMA episode, and I was surprised to hear that there are still people out there who don’t know about the Raptor trauma shears. I am highly biased, as I have now purchased 3 pairs of these shears myself, so I obviously love them. This is a small study in which 30 ED providers used both the Raptor shears and a motorized disc ring cutter to remove a ring from the finger of a volunteer. (This is an artificial scenario, and it is much harder to remove a ring from an incredibly swollen finger). The Raptors were quicker (8 seconds versus 67 seconds). Satisfaction was much higher (9.7/10 versus 3.8/10). Participant discomfort was also lower (0/10 versus 2/10). I have to say, when I initially bought the shears, I was highly skeptical that the ring cutter would ever be used. They just don’t look like they will work and I have had a lot of success removing rings non-destructively with the string wrapping technique. However, I have now cut through dozens of rings with 100% success. (I frequently get calls from our ICU to help them out with rings on very edematous patients). The tool is surprisingly effective, considering what it looks like, and definitely better than the alternatives I have seen. That being said, this small unblinded study proves nothing aside from the fact that at least a few other ED providers like these shears as much as I do.
Bottom line: I don’t know whether the price will be worth it to you, but I believe that the Leatherman Raptor trauma shears make a pretty good ring cutter.

Elevated blood pressure: NOT an abnormal vital sign
McAlister FA, Youngson E, Rowe BH. Elevated Blood Pressures Are Common in the Emergency Department but Are They Important? A Retrospective Cohort Study of 30,278 Adults. Ann Emerg Med. 2021 Apr;77(4):425-432. doi: 10.1016/j.annemergmed.2020.11.005. Epub 2021 Feb 10. PMID: 33579586
Asymptomatic hypertension is not an emergency. I don’t think that will be news to any of my readers, but I still get multiple referrals a week to the emergency department solely for a high blood pressure reading, so obviously this message is not getting through to some people. This is a retrospective cohort study looking at 30,278 emergency department visits in the province of Alberta over a 2 year period. 14,717 (48.6%) had an elevated blood pressure reading, of whom 10,732 (73%) had no prior diagnosis of hypertension. Clearfly, high blood pressure is not an abnormal vital sign. You cannot call something abnormal when it occurs in half of all patients. Despite 70% of patients receiving follow-up care within 1 month, only 33% of patients were started on antihypertensives, which is a strong indication that these patients didn’t actually have hypertension. (I think we all know that just being in the ED triage line raises the blood pressure of most normal individuals.) Most importantly, after adjusting for age, sex, diabetes, atrial fibrillation, and prior cardiovascular disease, having an elevated blood pressure in the ED was not associated with any bad outcomes over the next 2 years (stroke, transient ischemic attack, acute coronary syndrome, heart failure, or death). In fact, the results were almost statistically significant for an association showing that a high blood pressure was protective (HR 0.84, 95%CI 0.71-1.0). Even if you just look at the raw numbers, the risk of one of these outcomes was only 3.3% in the high blood pressure group and 2.5% in the normal blood pressure group.
Bottom line: High blood pressure is incredibly common in emergency department patients and not associated with adverse cardiovascular events over the next 2 years. There is no need for high blood pressure to be assessed or managed in the ED, and absolutely no role for referring patients with asymptomatic high blood pressure into the emergency department.
It is very important to be able to speak to your doctor
Portillo EN, Stack AM, Monuteaux MC, Curt A, Perron C, Lee LK. Association of limited English proficiency and increased pediatric emergency department revisits. Acad Emerg Med. 2021 Sep;28(9):1001-1011. doi: 10.1111/acem.14359. Epub 2021 Aug 25. PMID: 34431157
This is an interesting retrospective study looking at bounceback rates for pediatric emergency department visits based on English proficiency. They looked at 63,000 ED visits, 20% of which had a language other than English listed at their preference. There was a small but statistically significant (and probably clinically significant) increase in 72 hour bounceback visits among patients whose preferred language wasn’t English. The rate wasn’t increased among Spanish speaking patients, which would make sense if there were always Spanish speaking staff around in this American emergency department. However, the bounceback rate was even higher among patients who spoke other languages. Hospitalizations were the same in all groups, so this difference doesn’t seem to be the result of worse illness, but instead miscommunication. However, there is another explanation that is not discussed in the paper: it is possible that English speakers had easier access to primary care for follow-up. One major limitation of this study is that they classified anyone who listed a language other than English as their preferred language as having “limited English proficiency”. I know many people who speak English as their second language but have far better proficiency with the language than I do. However, if anything, this limitation would make the results even worse among the presumably smaller group of patients who really did have limited English proficiency. Another major limitation is that if language difficulties led to a bounceback visit, it is likely that the patient will seek care at another institution, which would not have been captured, and therefore the study might underestimate the number of bouncebacks. So this study is a long long way from perfect. However, I think it has face validity and offers an opportunity for us to reflect on our own practice when interacting with patients who speak different languages than we do.
Bottom line: This study is far from perfect, but it is likely that patients who don’t speak English are more likely to have 72 hour bounceback visits to the emergency department.
Do you bougie?
Driver BE, Semler MW, Self WH, et al. Effect of Use of a Bougie vs Endotracheal Tube With Stylet on Successful Intubation on the First Attempt Among Critically Ill Patients Undergoing Tracheal Intubation: A Randomized Clinical Trial. JAMA. 2021 Dec 8. doi: 10.1001/jama.2021.22002 PMID: 34879143
The worst thing about evidence based medicine is that it seems to be able to prove that basically everything doesn’t work. A prior single center RCT demonstrated a dramatic improvement in first pass success when a bougie was used routinely, but this follow up study seems to contradict those original findings. However, the devil is probably in the details. This is a multicenter RCT that includes 1102 adult patients being intubated in either an ED or ICU, and randomized them to a first attempt with either a bougie or an endotracheal tube with stylet. First pass success was the same in both groups, but it was pretty bad in both groups (80.4% vs 83.0%). Unlikely trials of medications, where the treatment effect is independent of the clinician, trials of procedures are complicated by the fact that clinician skill cannot be separated from the intervention. In the previous bougie RCT, first pass success was 96% with the bougie, which is a dramatic difference. I have questions about the overall quality of airway management here. For example, 33% of the patients were preoxygenated using only a nasal cannula, which I would never consider to be appropriate. I doubt that a bougie is required in every single case. Anatomy probably matters. But I tend to believe the results of the first RCT over this one, with the caveat that training matters. We all need to be masters of both airway techniques. That is just core emergency medicine.
Bottom line: This large multicentre RCT showed no benefit of routinely using a bougie for the first intubation attempts, but the result probably don’t apply to airway experts. Personally, I want to consider myself an airway expert.
Cheesy Joke of the Month
According to a recent poll, 6 out of 7 dwarves are not Happy.
Morgenstern, J. Research Roundup (January 2022), First10EM, January 24, 2022. Available at:
https://doi.org/10.51684/FIRS.124754


3 thoughts on “Research Roundup (January 2022)”
Hey Justin,
Always appreciate your work. FYI – on the macrodosing BUP article, the very large concern I have is that the data is from 4 years ago now (2018) and may not be relevant to those of us seeing/treating fentanyl/xylazine withdrawal. We are working on alterative regimens at our shop (hopefully we’ll publish some data you can share), but be aware, if your patients aren’t using heroin, there is a substantially increased risk for precipitated withdrawal than what is described here. We are investigating a microdosing strategy combined with short acting opioids; I would heavily caution those of you seeing patients utilizing fentanyl to be aware this article may no longer be clinically relevant. This lay article is the best we have so far: https://filtermag.org/fentanyl-buprenorphine-microdosing/ and this small case series: https://pubmed.ncbi.nlm.nih.gov/32572978/.
Thanks for the insight. Until recently, this was a rare prescription for me , so have stuck with mostly the standard regimen. However, have seen some failures at the normal doses.
Do you have a regimen for starting suboxone after naloxone? My understanding is that is another scenario where higher doses are needed