
Morgenstern, J. The BOUGIE trial: No difference between bougie and stylet?, First10EM, December 13, 2021. Available at:
https://doi.org/10.51684/FIRS.123836
Few topics provoke as many strong opinions in emergency medicine as airway management. Each and every one of us considers ourselves airway masters (despite lots of evidence to the contrary). We know for sure that our way is the best way. These strong and divergent opinions were well illustrated by the twitter comments after the publication of the newest RCT looking at using a bougie routinely on the first intubation attempt. Let’s try to skip past some of the opinions, and see what this new BOUGIE trial (Driver 2021) really tells us.
The Paper
The BOUGIE trial: Driver BE, Semler MW, Self WH, et al. Effect of Use of a Bougie vs Endotracheal Tube With Stylet on Successful Intubation on the First Attempt Among Critically Ill Patients Undergoing Tracheal Intubation: A Randomized Clinical Trial. JAMA. 2021 Dec 8. doi: 10.1001/jama.2021.22002 PMID: 34879143 Clinicaltrials.gov: NCT03928925
The Methods
This is a multicenter, unblinded, pragmatic, randomized clinical trial performed at 15 sites (7 emergency departments and 8 ICUs) from 11 hospitals in the United States.
Patients
Adult patients undergoing an intubation with sedation and a standard geometry blade.
Exclusions: pregnancy, incarceration, need for immediate intubation without time for randomization, and provider preference (if the intubating clinician thought either technique was either required or contraindicated).
Intervention
Intubation using a bougie for the first attempt. “Operators were instructed to pass the bougie into the trachea, have an assistant load the endotracheal tube (without a stylet) onto the bougie, advance the tube over the bougie through the vocal cords to the desired depth, and withdraw the bougie and the laryngoscope.”
Comparison
Intubation using an endotracheal tube with stylet. “Operators were instructed to use an endotracheal tube with a malleable stylet for the first attempt at tracheal intubation. The trial protocol recommended shaping the stylet straight with a distal bend of 25° to 35°.”
General protocols
Both groups received an instructional video on both techniques and in person training from the site principal investigator. This was a pragmatic trial, so aside from the use of a bougie or stylet, the rest of the intubation procedure was left entirely to the operator. Outcomes were measured by a trained, independent observer not part of the clinical team.
Outcome
The primary outcome was successful intubation on the first attempt (“defined as a single insertion of a laryngoscope blade into the mouth and either a single insertion of a bougie into the mouth followed by a single insertion of an endotracheal tube into the mouth or a single insertion of an endotracheal tube with stylet into the mouth.”).
The Results
They included 1102 patients with a median age of 58 and 41% being women. About 60% of the intubations were done in emergency departments and 40% in ICUs. About 40% of the patients had 1 or more markers for anatomical airway difficulty (for what these markers are worth), most of which was obesity.
The person performing the intubation was a resident 60% of the time, a fellow 34% of the time, and an attending physician only 2% of the time. Video laryngoscopy was used 75% of the time, with direct being used in the other 25%. Sedation was administered in 98% of patients and a paralytic in 97%.
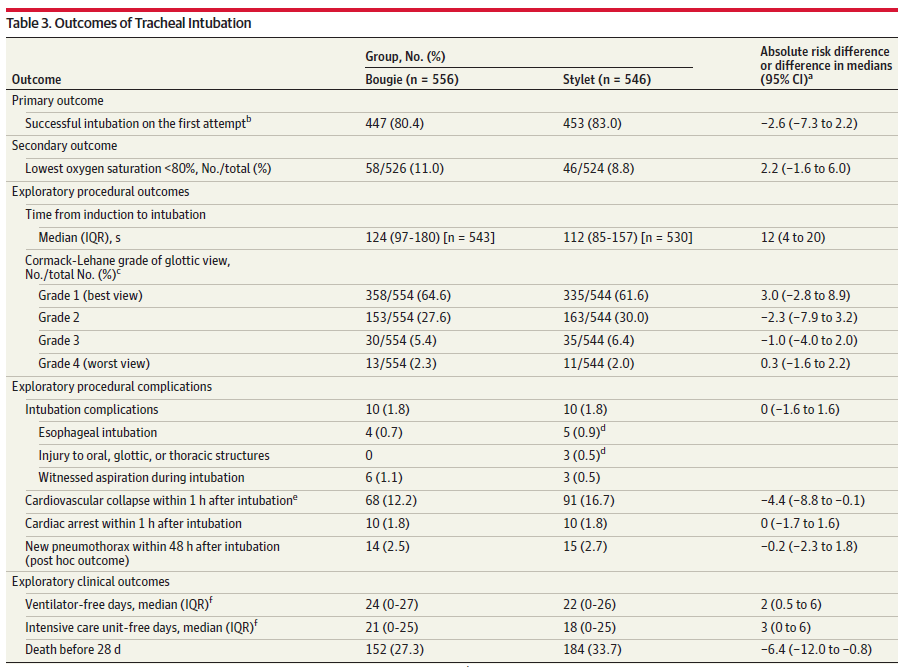
For the primary outcome, first pass success occurred in 80.4% of the bougie group and 83.0% of the stylet group (p=0.27, ARR -2.6%, 95% CI -7.3-2.2%).
Hypoxia less than 80% occurred in 11% of the bougie group and 9% of the stylet group.
Median time to intubation was 124 seconds with the bougie and 112 seconds with the stylet. Airway complications were identical at 1.8%
Mortality was 27% in the bougie group and 34% in the stylet group, which is a big difference, but given the other numbers, I don’t think it is possible this has anything to do with the stylet or bougie.
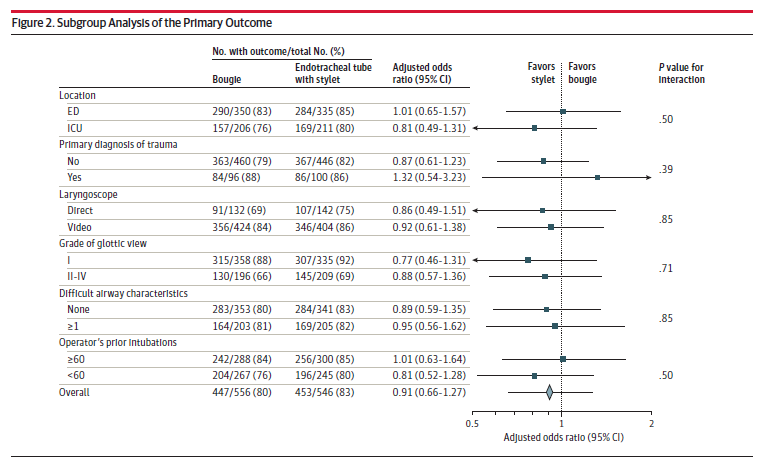
None of the subgroups were statistically significant.
My thoughts
This is a well done trial that provides us with valuable information. The authors should be commended for accomplishing a multi-center RCT for a basic airway intervention. In what seems like a rare feat to me, the final publication actually matches the registered trial protocol on clinicaltrials.gov. Even more impressive, these researchers somehow managed to continue an airway trial through the COVID-19 pandemic. Despite being an excellent trial, there are some significant limitations that we need to be aware of as we attempt to interpret and apply these results.
Open label trials are always somewhat problematic. Given the nature of the trial, there really isn’t any way to blind participants. However, you could imagine a group of residents who regularly intubate without a bougie being handed one with limited training. If they are much more comfortable with a stylet, I can imagine that they would be quicker to abandon the bougie if any difficulty was encountered. (The same bias occurs in the opposite direction, but my sense is that most training centers currently use a stylet and not a bougie for their first attempt.) Unfortunately, the manuscript does not contain any information about how much previous experience clinicians had with each technique, or whether there were preceding preferences, which could be very important in an open label trial. (Edit: In the supplement, there is an analysis that excludes attempts done by people with fewer than 5 previous intubations with a bougie. The overall first pass success rate is higher (85%), but is still the same in both groups.)
First pass success is strongly associated with clinical outcomes, which makes it one of the stronger surrogate research outcomes that we use, but we need to keep in mind that it is a surrogate outcome. This is complicated by the potential Hawthorne effect in this study. People knew they were being watched (there was an observer in the room). They knew what was being studied (they had been trained). Even if they didn’t know the primary outcome, it would have been easy to guess, as first pass success is always the primary outcome. Therefore, first pass success in this setting may not mean the same thing as first pass success in the real world. For example, clinicians may have been tempted to spend a little longer trying to pass the tube under the eyes of the observer, rather than rapidly moving on to a new technique when it was clear the first option was going to fail. However, if this were a big issue, I would have expected this trial to have a higher first pass success rate (potentially at the expense of more hypoxemia), but the first pass success was actually pretty bad in this trial.
The exclusion of all patients in whom the intubating clinician thought that there was an indication or contraindication for either a stylet or bougie limits the application of these results. Removing the obvious wins for either group (if you think they exist) biases the trial towards the null hypothesis. That being said, only 29 patients were excluded for this reason (primarily because clinicians thought that the bougie was needed), so hopefully the impact of this bias is limited.
The inclusion of trainees in airway trials is always somewhat problematic. Airway management is a complex skill that requires significant training to master. If Titleist released a new golf club with brand new technology, it is unlikely to provide any value in my hands, as I hack my way around the golf course, but could provide a significant advantage to a PGA professional. In order for any airway device to improve performance, the operator needs to be skilled with that device and the overall procedure. On the other hand, airway skills decay rapidly without practice, and residents usually have the most practice, so including staff doctors who only intubate twice a year may not be ideal. The pragmatic approach of this trial provides important information about the use of these devices for the average clinician, but may not translate well to airway experts (nor to very occasional intubators working outside of busy academic centers).
Pragmatic trials provide us very useful information about medical practice in the real world, but also have significant limitations. It is very hard to know how this data applies to my own practice, because I get the sense that many of these patients were managed in a way that I would consider substandard. For example, more than 33% of these patients were preoxygenated using only a standard nasal cannula! In my mind, that is completely unacceptable, and will not accomplish the goals of preoxygenation. I believe this is such a significant error, that it really makes me question the overall standard of airway management in this trial. (The rate of peri-intubation cardiac arrest (1.8%) and hemodynamic collapse (15%) are in keeping with previous research, but those previous studies came before an era where we emphasized resuscitation prior to intubation.) (Heffner 2013, Kim 2014, Wardi 2017)
Which brings us to the biggest issue with this trial: both groups performed relatively poorly. An 80% first pass success rate is not good enough. However, it is somewhat difficult to compare apples to apples here, because it is unclear what exactly should count as ‘an attempt’. Is your attempt over when you remove the laryngoscope from the mouth? When you remove the endotracheal tube? When the sats start to fall? This trial used a different definition than many prior studies. Using the more standard definition of removing the laryngoscope, their success rate falls in line with prior studies, at about 87%. That is better, but I personally think it still isn’t good enough.
The big difference between this trial and the original BEAM ( Driver 2018), which showed a dramatic improvement in first pass success with the bougie? The success rate was 98% when a bougie was used in the BEAM trial as compared to only 80% (or 87%) in this trial. When discussing the limitations of the BEAM trial, I discussed the limitations of extrapolating from single center trials. This single center routinely used the bougie and the intubators were highly trained. It was easy to guess that their success wouldn’t be replicated if the bougie was simply pushed into untrained hands.
This highlights the dangers of extrapolating from single center trials. There are often unique factors that limit the generalization of results. However, it is also important to consider the opposite problem: single center excellence can be washed out when averaged with multi-center mediocrity.
This concept can become very complicated. First off all, it is very easy for arrogant practitioners to overuse this excuse. “I know the studies say that cardiac stents don’t help these patients, but in my hands this is a life saving procedure.” It is too easy for this line of reasoning to completely subvert science. (I think we could solve this by making clinicians act as their own controls, to verify their claims.)
On the other hand, we shouldn’t completely write off a procedure based on studies in which practitioners were not adequately trained. The original BEAM RCT (Driver 2018) was pretty convincing, as long as you were clear about your conclusions: bougie significantly improved first pass success in this single center. Should that center look at this bigger trial and abandon the bougie? Of course not. Should we be looking at that center (Hennepin) to try to emulate their 98% success rate? Of course.
At the end of the day, you have to ask yourself which group you want to belong to: the group that used a stylet in this multicenter trial with an 87% success rate or the group that used a bougie in a single center trial with a 98% success rate. I know for certain what group I want to be in. The question is whether I am going to be able to replicate the success reported in Driver 2018. I would love to train at Hennepin. I would love it if every emergency doctor could receive the incredible training they obviously provide. I think the primary lesson from this trial is routine airway training is just not good enough. The experience described in the BEAM trial, with a 98% first pass success rate, is what we should be aiming for in emergency medicine.
Practically speaking, I think it will be very hard to show a difference between a bougie and a stylet. Prior to the publication of the Driver 2018 study, I never used the bougie for my first attempt at intubation, and my success rate with a stylet was very high. I think people who are well trained in either technique will have very high success rates. A lack of experience will lead to lower success with either technique. Whichever option you choose as your primary technique, you need to ensure you have mastered it. However, being facile with your backup option may be even more important, so I think it is critical that every emergency physician ensure that they have mastered both of these techniques.
Ultimately, airway management is not about the device, it is about the approach and the training. There is no ‘one size fits all’ piece of equipment that will get every patient intubated. I want to work in a place that develops a culture like Hennepin. If more of us did, I think we might see first pass success rates like those reported in the original BEAM study.
Bottom line
This multicenter RCT showed no difference in first pass success when comparing the use of a bougie to a stylet. We need to master both of these techniques.
Other FOAMed
Bougie is better (Driver 2018)
There are multiple great videos including the primary author and many experts at: BOUGIE trial results livestream on Critical Care Reviews
EMCrit 300 – Airway Continuous Quality Improvement and the Resus Airway Bundle
Bougie use in Emergency Airway Management (BEAM) – REBEL EM
George Kovacs on bougies:
Laryngoscopy and Bougie Pearls and Pitfalls Part 1: When and Why:
References
Driver BE, Semler MW, Self WH, et al. Effect of Use of a Bougie vs Endotracheal Tube With Stylet on Successful Intubation on the First Attempt Among Critically Ill Patients Undergoing Tracheal Intubation: A Randomized Clinical Trial. JAMA. 2021 Dec 8. doi: 10.1001/jama.2021.22002 PMID: 34879143
Driver BE, Prekker ME, Klein LR, et al. Effect of Use of a Bougie vs Endotracheal Tube and Stylet on First-Attempt Intubation Success Among Patients With Difficult Airways Undergoing Emergency Intubation: A Randomized Clinical Trial. JAMA. 2018; 319(21):2179-2189. PMID: 29800096
Heffner AC, Swords DS, Neale MN, Jones AE. Incidence and factors associated with cardiac arrest complicating emergency airway management. Resuscitation. 2013; 84(11):1500-4. PMID: 23911630
Kim WY, Kwak MK, Ko BS, Yoon JC, Sohn CH, Lim KS, Andersen LW, Donnino MW. Factors associated with the occurrence of cardiac arrest after emergency tracheal intubation in the emergency department. PLoS One. 2014 Nov 17;9(11):e112779. doi: 10.1371/journal.pone.0112779. PMID: 25402500
Wardi G, Villar J, Nguyen T, Vyas A, Pokrajac N, Minokadeh A, Lasoff D, Tainter C, Beitler JR, Sell RE. Factors and outcomes associated with inpatient cardiac arrest following emergent endotracheal intubation. Resuscitation. 2017 Dec;121:76-80. doi: 10.1016/j.resuscitation.2017.09.020. Epub 2017 Oct 12. PMID: 29032298

6 thoughts on “The BOUGIE trial: No difference between bougie and stylet?”
I tend to prefer a stylet but am unimpressed with this trial – or most of the airway trials. Under optimal conditions a bougie takes slightly longer because it basically adds one step so it is slightly more likely to cause a drop in saturation. It also doesn’t protect against aspiration as quickly. But an O2 sat < 80% is not just a surrogate endpoint it is a meaningless one. Saturations in this range are commonly experienced by mountaineers and free divers. A brief episode is completely harmless and irrelevant. So is first pass success. The risks of intubation are aspiration pneumonia (not aspiration per se), airway injury and hypoxia that causes permanent damage. A stylet is clearly faster and can be placed in the esophagus if the patient vomits during the procedure. A bougie is clearly better if the airway is hidden behind the epiglottis. I want both.
Thanks for everything you do and for your analysis here. Can you give some refs for “First pass success is strongly associated with clinical outcomes”……you mean, patient oriented outcomes? It just seems that many scenarios even in crisis situation don’t “seem” to have decompensation if one has to pull out, suction the bloody airway, buy 15 seconds where there’s no hypoxia, etc.
Cheers