
Morgenstern, J. Remdesivir: the evidence, First10EM, January 25, 2022. Available at:
https://doi.org/10.51684/FIRS.124935
This is part of the ongoing series of articles updating the evidence on current COVID-19 therapies. The rest of the series can be found here, and there is more to come. This article will cover the evidence for remdesivir in COVID-19.
Remdesivir (GS-5734) is an antiviral drug that was originally tested (unsuccessfully) in the treatment of Ebola. It is a prodrug that is metabolised in cells into an adenosine nucleotide analog that inhibits viral RNA polymerases, preventing replication. (Barlow 2020) There are laboratory and animal studies that demonstrate that remdesivir may have some inherent anti-viral properties against SARS-CoV-2 and other coronaviruses. (Wang 2020, Le Bras 2020) However, the evidence of clinical benefit is somewhat underwhelming.
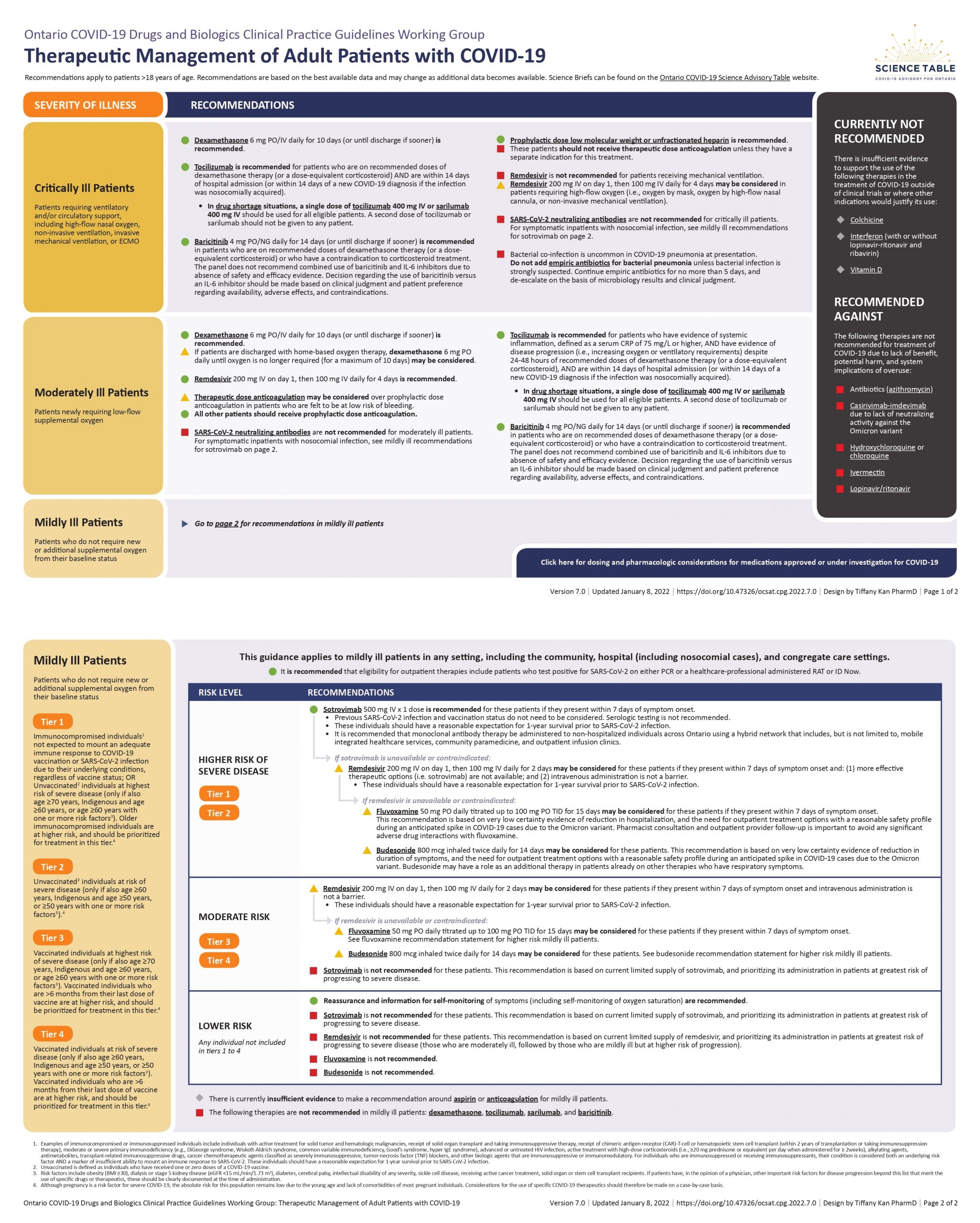
The Ontario Science Table recommendation
- Remdesivir is not recommended for patients receiving mechanical ventilation.
- A 5 day course of remdesivir may be considered for patients on high flow oxygen.
- A 5 day course of remdesivir is recommended for moderately ill patients.
- Remdesivir is not recommended in mildly ill patients (but the recommendation is based on drug shortages, not efficacy).
(Full recommendations available here.)
As a comparison, the World Health Organisation recommends against the use of remdesivir in all patients.
The remdesivir evidence
The first RCT was conducted at 10 hospitals in Hubei, China. (Wang 2020b) 237 patients hospitalized with severe COVID-19 (oxygen saturations less than 94%) and less than 12 days of symptoms were eligible to participate. The treatment group received 200mg of remdesivir on day 1 followed by 100mg daily on days 2-10, and that was compared to placebo. The primary endpoint was time to clinical improvement within 28 days of randomization. There was not a statistically significant difference in clinical improvement. Patients who received remdesivir had a median time to clinical improvement of 21 days as compared to 23 days with placebo. Mortality was not significantly different between the two groups (14% with remdesivir and 13% with placebo). Adverse events were found in 66% of the patients in the remdesivir group and 64% in the placebo group. More participants discontinued remdesivir because of adverse or serious adverse events than in the placebo group (12% vs 4%). This trial was stopped early, because the COVID-19 epidemic in Hubei was brought under control, which leaves it potentially under-powered to detect small differences between the groups.
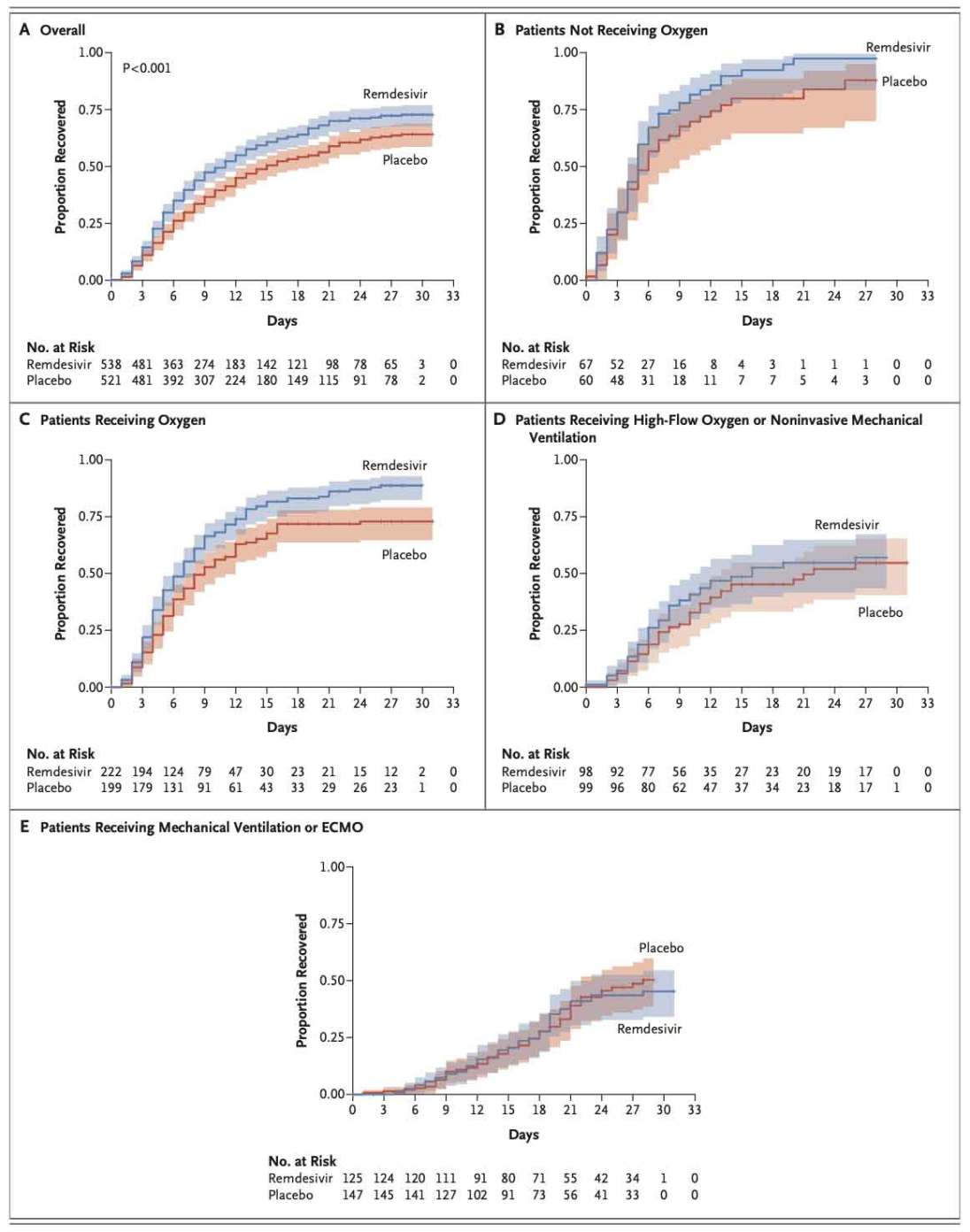
The ACCT-1 trial is a large multinational RCT that compared a 10-day course of remdesivir with placebo. (Beigel 2020) However, they couldn’t get placebo in Europe, so a portion of this trial was unblinded. In total, 1063 hospitalized patients were enrolled, with the vast majority required supplemental oxygen. The primary outcome measure, adjusted part way through the trial, was the time to recovery based on an 8-point ordinal scale. Participants in the remdesivir group had a shorter time to recovery (median 10 days) than patients in the placebo group (median 15 days), with a rate ratio for recovery of 1.29 (95% CI 1.12 to 1.49). The study’s original primary outcome, odds of improvement at 15 days, was also better with remdesivir (odds ratio 1.5; 95% CI 1.2-1.9). Mortality was not statistically different between the 2 groups at 29 days after randomization (11.4% in the remdesivir group versus 15.2% in the placebo group, hazard ratio 0.73, 95% CI 0.52 to 1.03). Serious adverse events were reported in 21.1% of the patients in the remdesivir group and in 27% of the patients in the placebo group. Most of the subgroup analyses represented similar benefits across all subgroups, but there was no benefit seen in patients who required mechanical ventilation, ECMO, noninvasive ventilation, or high flow oxygen at the time of enrollment. This makes sense, as remdesivir is an antiviral, and the critically ill are into an ARDS stage of their disease where viral load is less likely to be relevant. There are a number of potential sources of bias in the ACCT-1 trial, the biggest of which is that the trial was only partially blinded. That being said, it still represents the best trial of remdesivir that we have. There is a full blog post on this trial here.
There are two studies conducted by the manufacturer of Remdesivir. The first is an open-label RCT that compares a 5 day course of remdesivir to a 10 day course in patients 12 years and older hospitalized with COVID-19, an oxygen saturation less than 94%, but not requiring mechanical ventilation.(Goldman 2020) Because the trial does not contain a placebo or standard care control group, it does not help answer the question of whether remdesivir is effective. For what it’s worth, patients who received a 5-day course of remdesivir had a similar clinical status at day 14 to that of patients who received a 10-day course of remdesivir (p=0.14). Among all participants, 21% of patients in the 5-day group and 35% in the 10-day group experienced serious adverse events.
The fourth trial was another manufacturer conducted, open-label, multicenter, RCT which tested remdesivir in 596 hospitalized patients with confirmed SARS-CoV-2 infection. (Spinner 2020) Patients were less sick than in the other trials, as an oxygen saturation greater than 94% on room air was part of the inclusion criteria. Patients were randomized to receive a 5-day course of remdesivir, a 10-day course of remdesivir, or usual care. The primary outcome was the assessment of patients’ clinical status on day 11, defined by a 7-point scale with ordered categories (from death to not hospitalized). I find the choice of 11 days as a primary outcome very bizarre. Most trials would choose 10 or 14 days. The choice of 11 days seems like a post-hoc data-dredged type of outcome, rather than a prospectively chosen outcome. They changed to this outcome more than ½ way through the trial. After 11 days, the group of patients randomized to the 5 day remdesivir treatment had a higher odds of an improved clinical status when compared to patients receiving standard care (odds ratio 1.65; 95% CI 1.09-2.48). However, there was not a statistical benefit seen in the 10 day treatment group. There was no difference in mortality (1% in the 5 day group, 2% in the 10 day group, and 2% in the standard care group). There were no statistical differences in length of oxygen therapy or hospitalization. Adverse events occurred in 51% of the 5 day group, 59% of the 10 day group, and 47% of the standard care group, with the difference between the 10 day group and standard care being statistically significant.
Both of the manufacturer conducted trials have significant limitations. They were both open label trials, which significantly increases the risk of bias. They employ an ordinal scale, which makes the absolute benefit difficult to assess. Furthermore, not all levels of the scale are equally important, so a similar numeric improvement on the scale could represent very different clinical improvements. In the second trial, patients in the 10 day group only received a median of 6 doses, with only 38% of the patients receiving the full 10 day treatment, limiting the trial’s ability to distinguish between 5 and 10 days of treatment.
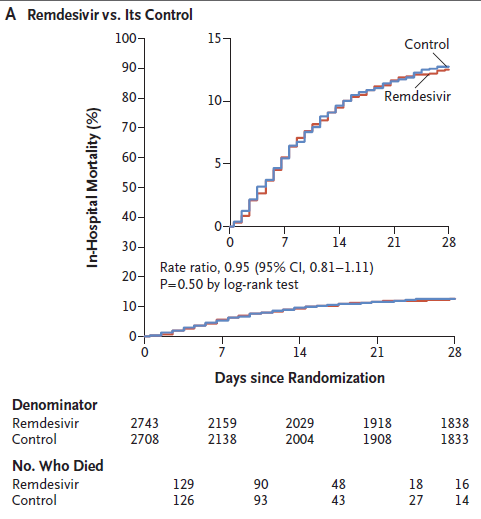
The fifth trial is SOLIDARITY, a large multinational open-label adaptive design RCT that is looking at a number of agents in hospitalized COVID-19 patients. (WHO 2021) The publication we have is only an interim release. The final data is not available anywhere. In the Remdesivir arm, 2743 patients received a 10 day course of remdesivir and 2708 received standard care. There was no statistical effect on mortality, with a rate ratio of 0.95 (95% confidence intervals 0.81 to 1.11). There was also no effect on mechanical ventilation. Hospital length of stay was longer in the remdesivir group than the control group (at 7 days 69% of the remdesivir group was still in hospital as compared to 59% of the control group), but that outcome is likely to be biased by the open-label trial design, and the fact that remdesivir needs to be given by an intravenous infusion. At this time, these results are only available as a preprint of an interim analysis.
CATCO is another open-label pragmatic RCT that was performed in conjunction with the SOLIDARITY trial. (Ali 2022) In admitted patients with confirmed COVID-19, they compared remdesivir to standard care. Some of these patients are included in the above SOLIDARITY trial, but the Canadian arm continued randomizing for a few extra months, so some are not. (You really shouldn’t count the same data twice. It is a type of publication bias. Of the 1282 patients in this study, 951 were included in the SOLIDARITY trial, so this is mostly duplicate data.) There was no change in the primary outcome of in-hospital mortality (18.7% vs 22.6%, RR 0.83, 95%CI 0.67-1.03). There was a difference in need for mechanical ventilation (8% vs 15%, RR.053, 95% CI 0.38-0.75). There was no difference in hospital length of stay or need for oxygen therapy. Although it is presented as its own publication, this really really just a subgroup analysis of the SOLIDARITY trial, and should be interpreted as such. The overall data suggest no change in need for mechanical ventilation, but the ‘treated in Canada’ subgroup is statistically significant. Not only that, the primary outcome in this subgroup was negative. So this is a secondary outcome in a subgroup analysis. If that was published in the same paper, we would know to dismiss it out of hand. (This is very similar to how in ISIS 2 it looks like thrombolytics for MI don’t work if you were a gemini, or if you were from 2 specific countries. We ignore these subgroups, because we know they are mathematical falsities.) (Sleight 2000) Furthermore, this publication has the same limitations as SOLIDARITY as a whole: it is unblinded. The fact that there was a change in need for mechanical ventilation, but no change in the need for oxygen, seems to suggest the outcomes are biassed.
The DisCoVeRy trial was an open-label, adaptive, multiple centred RCT of hospitalised patients requiring oxygen with confirmed COVID-19. (Ader 2021) There were multiple arms, but 1 was a 10 day course of remdesivir, and that was compared to standard care. 857 patients with randomised to either remdesivir or standard care. In terms of their primary outcome (clinical status on day 15), there was no difference between the two groups. There were also no significant results for any of the many secondary outcomes they looked at. Again, all these patients required oxygen at the time of enrollment, so it may simply have been too late to benefit from an antiviral. (This trial was also performed in conjunction with SOLIDARITY, but unlike CATCO less than 10% of the patients included here were included in SOLIDARITY, so there is a lot less overlap.)
There is another very small (70 patient) open label RCT out of India that is not really contributory to the discussion, but was a negative trial. (Mahajan 2021)
The PINETREE trial is a double-blind, placebo controlled RCT in outpatients 12 years and older with less than 7 days of symptoms and at least 1 risk factor for disease progression. (Gotlieb 2021) 562 patients were randomised to a 3 day course of remdesivir or placebo. Unfortunately, this is another trial that uses the incredibly biassed “COVID-19 related hospitalisation” as part of their composite primary outcome (with death). (They also changed their primary outcome from their original protocol, away from the actually important all-cause hospitalisation.) There was a statistically significant improvement in this primary outcome (5.3% vs 0.7%, p=0.008). There were no deaths at all, so their entire primary outcome was this biassed statistical fabrication. Luckily, unlike some of the other studies, they actually report all cause hospitalisation, and it was improved as well (1.8% vs 6.4%). Alleviation of symptoms by day 14 was also better with remdesivir, although it was pretty bad in both groups (35% vs 25%).
Systematic reviews
I think systematic reviews and meta-analyses have been badly misused throughout the COVID pandemic. A meta-analysis provides us with a very precise appearing numerical conclusion, and so people have tended to make strong recommendations based on systematic reviews. However, that single numerical summary masks the many sources of bias and uncertainty in the individual trials.
However, unlike some of our other options (such paxlovid where not even a single study has been published), there have been enough publications on remdesivir that a meta-analysis may help us summarize the current results (as long as we remain aware of the significant limitations of the individual trials.)
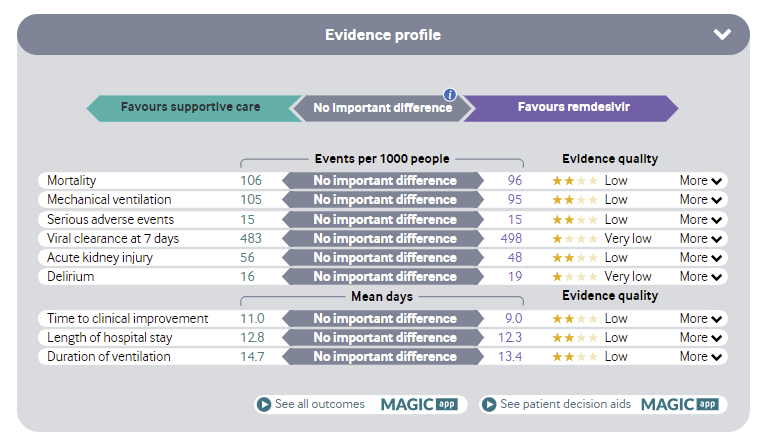
The living meta-analysis of COVID therapies in the BMJ lists remdesivir in the “not different from standard care” section. (Siemieniuk 2021) It concludes that there is no difference in mortality, adverse events, viral clearance at 7 days, duration of hospital stay, or time to symptom resolution. There is a ‘low certainty’ decrease in mechanical ventilation with borderline statistical significance (2.6% absolute decrease with 95% CI 5.1% to 0.2%). Considering the unblinded nature of these trials and that all other outcomes are negative, this needs to be taken with a grain of salt. (This is based on everything up to the SOLIDARITY interim results).
The Cochrane review concludes that “remdesivir probably makes little or no difference to all‐cause mortality”. (Ansems 2021) They were “uncertain whether remdesivir increases or decreases the chance of clinical improvement in terms of duration to liberation from supplemental oxygen” and “very uncertain whether remdesivir decreases or increases the risk of clinical worsening in terms of new need for mechanical ventilation”. However, “remdesivir probably decreases the serious adverse events rate”. (Also up to SOLIDARITY interim results.)
Other systematic reviews consistently find no mortality benefit with remdesivir. (Kaka 2021; Singh 2021) These reviews differ somewhat in their other conclusions, and suggest remdesivir may improve time to clinical improvement. However, considering the predominance of unblinded studies, any subjective outcomes are highly likely to be biassed.
Here is the WHO summary of the evidence:
However, there is one systematic review that stands out in contrast, because it has been widely cited (at least on twitter) as demonstrating a mortality benefit from remdesivir. (Lee 2022) (It is only currently available as a preprint, and so hadn’t been peer reviewed). Importantly, it doesn’t actually demonstrate a mortality benefit overall (RR 0.92, 95% CI 0.80 to 1.06). It is only when patients are broken into subgroups that the mortality benefit becomes statistically significant, and only in patients requiring oxygen but not mechanical ventilation (RR 0.83 95% CI 0.73-0.95). The RR in patients not requiring oxygen also looks good, but with massive confidence intervals. However, if you want to accept these numbers, you probably also have to accept the opposite, where it looks like remdesivir increases mortality in mechanically ventilated patients (RR 1.19 95% CI 0.96-1.44). That is really important, because one of the most common arguments for giving remdesivir despite imperfect evidence is its lack of harm. However, if remdesivir increases mortality in a subgroup of patients, it obviously is capable of significant harm. More likely, we have yet again fallen into the subgroup trap. Subgroups turn out to be wrong more often than they are right. Although this benefit has a reasonable physiologic basis, and was present in the biggest trials, it doesn’t appear consistently in the data, with 3 of the 8 trials having point estimates on the side of mortality increasing with remdesivir. This may be a real finding, and is certainly hypothesis generating, but it is still more likely that this is a statistical anomaly than a real effect. (Aside from just mathematic chance, there are a number of potential sources of bias that could explain the subgroup finding. First, it is not always clear from the data who required oxygen at what time. Some people receive oxygen but don’t actually need it. And the definitions in each study are somewhat different, so in order to perform this analysis, the authors had to make their own decisions about where patients fit. This adds a lot of subjectivity to the data.)

Comments
The WHO completely recommends against remdesivir. Many other organisations, including the Ontario Science table, take the exact opposite stance, and state that remdesivir should be used. I have a hard time supporting either of those positions.
The key take away from these trials seems to be uncertainty. We have multiple large trials with negative primary outcomes. However, the two highest quality (placebo controlled) trials were positive. There are subgroups and secondary analyses that look promising. However, we know that most subgroups and secondary analyses are wrong.
Most of the point estimates fall on the side of remdesivir providing some value. However, these trials also have some significant sources of bias that should tend to push those point estimates towards showing benefit. Furthermore, the fact that we don’t see a clear benefit with almost 10,000 patients enrolled in studies tells us that any benefit that exists will be pretty small.
Speaking of small benefits, it is important to make the same caveat I always make about extrapolation from these studies. Most patients were unvaccinated. Many were enrolled before steroids and tocilizumab were being given. Therefore, any benefit seen in these studies will be significantly smaller in real life in 2022, as outcomes are better across the board. (The relative risk reduction may stay the same, but the absolute benefit will be smaller.)
At this point, I think it would be a mistake to make definite conclusions. If remdesivir provides benefit, it is not going to be anything like the benefit we see from systemic steroids. This is clearly not a miracle cure. On the other hand, remdesivir is certainly more likely to provide a benefit than something like ivermectin. I think the best guess is very close to 50/50 whether remdesivir provides net patient oriented benefit at this point. (And that is not factoring in issues of cost or opportunity cost.)
The biggest debate is probably related to the certainty provided by subgroup analyses. It certainly makes sense that an antiviral would work better if used earlier, and it might just be too late for patients on mechanical ventilation. (In the ACCT-1 data, the benefit also disappeared for patients on high flow oxygen). However, I think we need to be really cautious about these numbers. Subgroups are just not a reliable source of evidence. (Wallach 2016; Sleight 200;Yusuf 1991) On the other hand, when subgroups demonstrate a change in a really important outcome (all cause mortality), it probably makes sense to pay some attention while waiting for more data. However, if people are going to act on these subgroups, they need to recognize both sides of the coin, and acknowledge that IF remdesivir lowers mortality in some patients it probably also increases mortality in others, and at this point we are not certain which patients are which.
In an ideal world, all patients would still be enrolled in high quality placebo controlled RCTs, and we could settle this debate quickly. I think it is reasonable to prescribe remdesivir in hospitalized patients requiring low flow oxygen, but it is also reasonable for physicians to forgo it (ie, it “may be considered”). At this point, considering the substantial investment that would be required to provide this intravenous therapy to outpatients, I think we need confirmatory data before rolling out treatment in that population.
Bottom line
The overall quality of evidence is low at this point, but we do have 2 blinded RCTs demonstrating a benefit. The best guess is that remdesivir doesn’t save lives overall, but it may shorten illness duration, and there may be a subgroup of patients (inpatients on low flow oxygen) with a larger benefit.
Other FOAMed
Other First10EM COVID therapeutics updates can be found here
Ontario Science Table Recommendations
Remdesivir for Hospitalized Patients with COVID-19
PulmCrit – Preliminary report on NIAID trial of remdesivir (ACTT-1)
COVID-19: Two More Trials Just Published on Remdesivir
PulmCrit – Eleven reasons the NEJM paper on remdesivir reveals nothing
Myths in Emergency Medicine: Remdesivir Is Not the Magic Bullet for COVID-19
IBCC: Management of COVID-19 patients admitted to stepdown or ICU
References
Ader F, Bouscambert-Duchamp M, Hites M, Peiffer-Smadja N, Poissy J, Belhadi D, Diallo A, Lê MP, Peytavin G, Staub T, Greil R, Guedj J, Paiva JA, Costagliola D, Yazdanpanah Y, Burdet C, Mentré F; DisCoVeRy Study Group. Remdesivir plus standard of care versus standard of care alone for the treatment of patients admitted to hospital with COVID-19 (DisCoVeRy): a phase 3, randomised, controlled, open-label trial. Lancet Infect Dis. 2021 Sep 14:S1473-3099(21)00485-0. doi: 10.1016/S1473-3099(21)00485-0. Epub ahead of print. PMID: 34534511
Ali K, Azher T, Baqi M, Binnie A, Borgia S, Carrier FM, Cavayas YA, Chagnon N, Cheng MP, Conly J, Costiniuk C, Daley P, Daneman N, Douglas J, Downey C, Duan E, Duceppe E, Durand M, English S, Farjou G, Fera E, Fontela P, Fowler R, Fralick M, Geagea A, Grant J, Harrison LB, Havey T, Hoang H, Kelly LE, Keynan Y, Khwaja K, Klein G, Klein M, Kolan C, Kronfli N, Lamontagne F, Lau R, Fralick M, Lee TC, Lee N, Lim R, Longo S, Lostun A, MacIntyre E, Malhamé I, Mangof K, McGuinty M, Mergler S, Munan MP, Murthy S, O’Neil C, Ovakim D, Papenburg J, Parhar K, Parvathy SN, Patel C, Perez-Patrigeon S, Pinto R, Rajakumaran S, Rishu A, Roba-Oshin M, Rushton M, Saleem M, Salvadori M, Scherr K, Schwartz K, Semret M, Silverman M, Singh A, Sligl W, Smith S, Somayaji R, Tan DHS, Tobin S, Todd M, Tran TV, Tremblay A, Tsang J, Turgeon A, Vakil E, Weatherald J, Yansouni C, Zarychanski R; Canadian Treatments for COVID-19 (CATCO); Association of Medical Microbiology and Infectious Disease Canada (AMMI) Clinical Research Network and the Canadian Critical Care Trials Group. Remdesivir for the treatment of patients in hospital with COVID-19 in Canada: a randomized controlled trial. CMAJ. 2022 Jan 19:cmaj.211698. doi: 10.1503/cmaj.211698. Epub ahead of print. PMID: 35045989
Ansems K, Grundeis F, Dahms K, Mikolajewska A, Thieme V, Piechotta V, Metzendorf M-I, Stegemann M, Benstoem C, Fichtner F. Remdesivir for the treatment of COVID‐19. Cochrane Database of Systematic Reviews 2021, Issue 8. Art. No.: CD014962. DOI: 10.1002/14651858.CD014962. Accessed 23 January 2022.
Barlow A, Landolf KM, Barlow B, et al. Review of Emerging Pharmacotherapy for the Treatment of Coronavirus Disease 2019. Pharmacotherapy. 2020;40(5):416-437. doi:10.1002/phar.2398
Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the Treatment of Covid-19 — Preliminary Report. New England Journal of Medicine. 2020;0(0):null. doi:10.1056/NEJMoa2007764
Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the Treatment of Covid-19 – Final Report. N Engl J Med. 2020 Oct 8:NEJMoa2007764. doi: 10.1056/NEJMoa2007764. Epub ahead of print. PMID: 32445440; PMCID: PMC7262788.
Goldman JD, Lye DCB, Hui DS, et al. Remdesivir for 5 or 10 Days in Patients with Severe Covid-19. New England Journal of Medicine. 2020;0(0):null. doi:10.1056/NEJMoa2015301
Gottlieb RL, Vaca CE, Paredes R, Mera J, Webb BJ, Perez G, Oguchi G, Ryan P, Nielsen BU, Brown M, Hidalgo A, Sachdeva Y, Mittal S, Osiyemi O, Skarbinski J, Juneja K, Hyland RH, Osinusi A, Chen S, Camus G, Abdelghany M, Davies S, Behenna-Renton N, Duff F, Marty FM, Katz MJ, Ginde AA, Brown SM, Schiffer JT, Hill JA; GS-US-540-9012 (PINETREE) Investigators. Early Remdesivir to Prevent Progression to Severe Covid-19 in Outpatients. N Engl J Med. 2021 Dec 22:NEJMoa2116846. doi: 10.1056/NEJMoa2116846. Epub ahead of print. PMID: 34937145
Kaka AS, MacDonald R, Greer N, Vela K, Duan-Porter W, Obley A, Wilt TJ. Major Update: Remdesivir for Adults With COVID-19 : A Living Systematic Review and Meta-analysis for the American College of Physicians Practice Points. Ann Intern Med. 2021 May;174(5):663-672. doi: 10.7326/M20-8148. Epub 2021 Feb 9. Update in: Ann Intern Med. 2021 Dec;174(12):W114-W115. Erratum in: Ann Intern Med. 2021 Mar 16;: PMID: 33560863
Le Bras A. Efficacy of remdesivir in a rhesus macaque model of MERS-CoV infection. Lab Animal. 2020;49(5):150-150. doi:10.1038/s41684-020-0537-x
Lee TC, Murthy S, Del Corpo OC, et al. Remdesivir for the Treatment of COVID-19: An Updated Systematic Review and Meta-Analysis. 2022. https://doi.org/10.1101/2022.01.22.22269545
Mahajan L, Singh AP, Gifty. Clinical outcomes of using remdesivir in patients with moderate to severe COVID-19: A prospective randomised study. Indian J Anaesth. 2021 Mar;65(Suppl 1):S41-S46. doi: 10.4103/ija.IJA_149_21. Epub 2021 Mar 20. PMID: 33814589
Pan H, Peto R, Karim QA, et al. Repurposed antiviral drugs for COVID-19; interim WHO SOLIDARITY trial results. medRxiv. Published online October 15, 2020:2020.10.15.20209817. doi:10.1101/2020.10.15.20209817
Siemieniuk RA, Bartoszko JJ, Ge L, Zeraatkar D, Izcovich A, Kum E, Pardo-Hernandez H, Qasim A, Martinez JPD, Rochwerg B, Lamontagne F, Han MA, Liu Q, Agarwal A, Agoritsas T, Chu DK, Couban R, Cusano E, Darzi A, Devji T, Fang B, Fang C, Flottorp SA, Foroutan F, Ghadimi M, Heels-Ansdell D, Honarmand K, Hou L, Hou X, Ibrahim Q, Khamis A, Lam B, Loeb M, Marcucci M, McLeod SL, Motaghi S, Murthy S, Mustafa RA, Neary JD, Rada G, Riaz IB, Sadeghirad B, Sekercioglu N, Sheng L, Sreekanta A, Switzer C, Tendal B, Thabane L, Tomlinson G, Turner T, Vandvik PO, Vernooij RW, Viteri-García A, Wang Y, Yao L, Ye Z, Guyatt GH, Brignardello-Petersen R. Drug treatments for covid-19: living systematic review and network meta-analysis. BMJ. 2020 Jul 30;370:m2980. doi: 10.1136/bmj.m2980. Update in: BMJ. 2020 Sep 11;370:m3536. Update in: BMJ. 2020 Dec 17;371:m4852. Update in: BMJ. 2021 Mar 31;372:n858. Erratum in: BMJ. 2021 Apr 13;373:n967. PMID: 32732190
Singh S, Khera D, Chugh A, Khera PS, Chugh VK. Efficacy and safety of remdesivir in COVID-19 caused by SARS-CoV-2: a systematic review and meta-analysis. BMJ Open. 2021 Jun 24;11(6):e048416. doi: 10.1136/bmjopen-2020-048416. PMID: 34168031
Sleight P. Debate: Subgroup analyses in clinical trials: fun to look at – but don’t believe them! Curr Control Trials Cardiovasc Med. 2000;1(1):25-27. doi: 10.1186/cvm-1-1-025. PMID: 11714402
Spinner CD, Gottlieb RL, Criner GJ, et al. Effect of Remdesivir vs Standard Care on Clinical Status at 11 Days in Patients With Moderate COVID-19: A Randomized Clinical Trial. JAMA. Published online August 21, 2020. doi:10.1001/jama.2020.16349
Wang M, Cao R, Zhang L, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020;30(3):269-271. doi:10.1038/s41422-020-0282-0
Wang Y, Zhang D, Du G, et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. The Lancet. Published online 2020.
Yokoyama Y, Briasoulis A, Takagi H, Kuno T. Effect of remdesivir on patients with COVID-19: A network meta-analysis of randomized control trials. Virus Res. 2020;288:198137. doi:10.1016/j.virusres.2020.198137
Wallach JD, Sullivan PG, Trepanowski JF, Sainani KL, Steyerberg EW, Ioannidis JP. Evaluation of Evidence of Statistical Support and Corroboration of Subgroup Claims in Randomized Clinical Trials. JAMA Intern Med. 2017 Apr 1;177(4):554-560. doi: 10.1001/jamainternmed.2016.9125. PMID: 28192563
WHO Solidarity Trial Consortium, Pan H, Peto R, Henao-Restrepo AM, Preziosi MP, Sathiyamoorthy V, Abdool Karim Q, Alejandria MM, Hernández García C, Kieny MP, Malekzadeh R, Murthy S, Reddy KS, Roses Periago M, Abi Hanna P, Ader F, Al-Bader AM, Alhasawi A, Allum E, Alotaibi A, Alvarez-Moreno CA, Appadoo S, Asiri A, Aukrust P, Barratt-Due A, Bellani S, Branca M, Cappel-Porter HBC, Cerrato N, Chow TS, Como N, Eustace J, García PJ, Godbole S, Gotuzzo E, Griskevicius L, Hamra R, Hassan M, Hassany M, Hutton D, Irmansyah I, Jancoriene L, Kirwan J, Kumar S, Lennon P, Lopardo G, Lydon P, Magrini N, Maguire T, Manevska S, Manuel O, McGinty S, Medina MT, Mesa Rubio ML, Miranda-Montoya MC, Nel J, Nunes EP, Perola M, Portolés A, Rasmin MR, Raza A, Rees H, Reges PPS, Rogers CA, Salami K, Salvadori MI, Sinani N, Sterne JAC, Stevanovikj M, Tacconelli E, Tikkinen KAO, Trelle S, Zaid H, Røttingen JA, Swaminathan S. Repurposed Antiviral Drugs for Covid-19 – Interim WHO Solidarity Trial Results. N Engl J Med. 2021 Feb 11;384(6):497-511. doi: 10.1056/NEJMoa2023184. Epub 2020 Dec 2. PMID: 33264556
Yusuf S, Wittes J, Probstfield J, Tyroler HA. Analysis and interpretation of treatment effects in subgroups of patients in randomized clinical trials. JAMA. 1991 Jul 3;266(1):93-8. PMID: 2046134
Photo by Annie Spratt on Unsplash

{kind=link}
4 thoughts on “Remdesivir: the evidence”
1. Justin, thankfully, acknowledges the Ebola/remdesivir study and calls it “unsuccessful”. He just didn’t elaborate on the mortality rate from it. To elaborate further, the mortality figures: “ (remdesivir) had the highest mortality of any of the treatment modalities with 53.1 percent of the Ebola patients who were administered Veklury® (remdesivir) dying within 28 days.“
https://www.nejm.org/doi/10.1056/NEJMoa1910993?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
2. I would be curious on his thoughts on how, “Remdesivir can also induce significant cytotoxic effects in cardiomyocytes that is considerably worse than chloroquine cardiotoxic effects. “. https://pubmed.ncbi.nlm.nih.gov/34643857/ Especially since Fauci determined that hydroxy/chloroquine were off the table because of the very same issue. ?Double standard favoring patented drugs?
3. Dr Bryan Ardis has done a deep dive as he believes his father in law went into kidney failure and died after given remdesjvir in hospital. He hasn’t stopped talking since. An excellent breakdown of the studies: https://principia-scientific.com/doctor-reveals-remdesivir-is-real-cause-of-covid-19-maladies/