
Morgenstern, J. Research Roundup (April 2023), First10EM, April 10, 2023. Available at:
https://doi.org/10.51684/FIRS.129664
Before jumping into this edition, I need to address the maternal kisses study discussed last time. Obviously the study was satire, and did an excellent job in making us laugh, but most satire studies (like those in the Christmas edition of the BMJ) are real studies. Apparently this paper was entirely fictional (or perhaps the word is fraudulent?) It was just made up, but there isn’t a note anywhere in the manuscript or on the webpage to say that is the case. I think that is very dangerous. Science is based on trust, and we expect scientific journals to publish fact not fiction. With absolutely no label to indicate the publication was fictional, there is nothing to stop people from citing this data or even including it in meta-analyses in the future. (Yes, the size of the study might have been an indication it wasn’t real, but I just assumed it was a subpart of a real study for which the parents and children were already present. If you think the subject matter alone was enough to indicate it was fiction, you clearly haven’t spent as much time reading bizarre scientific publications as I have.) Although the study was clearly satire, it is possible to mix real data with satire, being both informative and entertaining. That is the nature of science satire. Every other satire paper I have ever covered was a real study (I think). To publish a scientific manuscript in a normal format with apparently real data, but which is entirely fake, seems like scientific misconduct by the Journal of Evaluation in Clinical Practice. We joked about the ethical conduct of the researchers when we originally discussed this paper, but apparently it was the journal with questionable ethical practices. But the point is that in both blog and podcast formats last time, I discussed a fake paper as if it were real, so the egg is on my face.
Does nothing matter in sepsis?
The CLOVERS trial: National Heart, Lung, and Blood Institute Prevention and Early Treatment of Acute Lung Injury Clinical Trials Network; Shapiro NI, Douglas IS, Brower RG, et al. Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension. N Engl J Med. 2023 Jan 21. doi: 10.1056/NEJMoa2212663. Epub ahead of print. PMID: 36688507
There has been a move away from salt water in the management of sepsis, with suggestions that early vasopressors might make more sense. The CLOVERS trial was an open-label multicentre RCT that compared ‘liberal’ and ‘restrictive’ fluid strategies in adult septic patients with a blood pressure less than 100 systolic after a 1 L bolus. In the first 24 hours, there was about a 2 L difference in fluids given to the two groups, which seems reasonable to me. (Everyone had already received about 2 L before being enrolled.) There was no difference in the primary outcome of mortality, nor in any of the secondary outcomes or subgroup analyses. You can read my full thoughts on the paper here, but I think the big caveat to consider is how diverse this group of patients is. This study did not attempt to stratify by patients who might require more or less fluids (or who might be ‘fluid responsive’.) It is possible that you will fare better making this decision based on clinical judgment. However, there is one major advantage to early vasopressors not captured here: the guaranteed ICU bed. This is still a sick group of patients, but we are often tempted to send them to the floor if their blood pressure (temporarily) improves with a bolus. Using vasopressors over fluid boluses saves us from that mistake.
Bottom line: Unsurprisingly, a couple liters of IV fluids didn’t have a mortality benefit in hypotensive sepsis patients. It remains on you to decide the best time to transition from boluses to norepinephrine for the patient in front of you.
Diagnosis with a twist: It’s impossible to be perfect
Lukosiute-Urboniene A, Nekrosius D, Dekeryte I, Kilda A, Malcius D. Clinical risk factors for testicular torsion and a warning against falsely reassuring ultrasound scans: a 10-year single-centre experience. Emerg Med J. 2022 Dec 16:emermed-2021-211946. doi: 10.1136/emermed-2021-211946. Epub ahead of print. PMID: 36526335
This is a single center chart review looking at all pediatric patients admitted to the urology ward with a diagnosis with testicular torsion, orchitis, and epididymitis over a 10 years period. As far as chart review methodology goes, I would give this paper a medium grade. They discuss their methodology, including the use of a standardized abstraction form and a plan for how to deal with missing data, which is a huge step up from most chart reviews which say nothing at all. However, their plan to deal with missing data was just to eliminate the patient, which is a huge potential source of bias (perhaps people only document a finding like cremasteric reflex when it is abnormal.) Furthermore, they specifically decided not to test inter-rater reliability, and they did not blind the abstractors to their thesis, nor the patient’s final diagnosis, so there are massive sources of bias to consider. Also, I imagine a large number of patients don’t receive a formal diagnosis, and are not admitted to the surgery department, so this paper is likely to miss the majority of low risk cases. (I would expect this to result in an overestimate of positive likelihood ratios and an underestimate of negative likelihood ratios). Overall, they include 555 patients, of whom 35% had testicular torsion (which seems high, probably confirming my concern about selection bias). The main takeaway is that there are no individual features that can stand alone to either rule in or rule out the diagnosis. The presence of vomiting was the closest to a rule in, with a positive likelihood ratio of 32. Age over 13, vomiting, abdominal or groin pain, hard testis, and scrotal edema were also statistically associated with torsion. Perhaps the most important finding/reminder from this paper is that ultrasound is nowhere close to perfect for diagnosing torsion. Absent blood flow is pretty good at ruling in (positive likelihood ratio 32), but a full 42% of kids with confirmed torsion had normal blood flow on their ultrasound, for a sensitivity of only 58%. There are numerous other ultrasound findings, and unfortunately they don’t report the test characteristics of a perfectly normal ultrasound, which might be good to know.
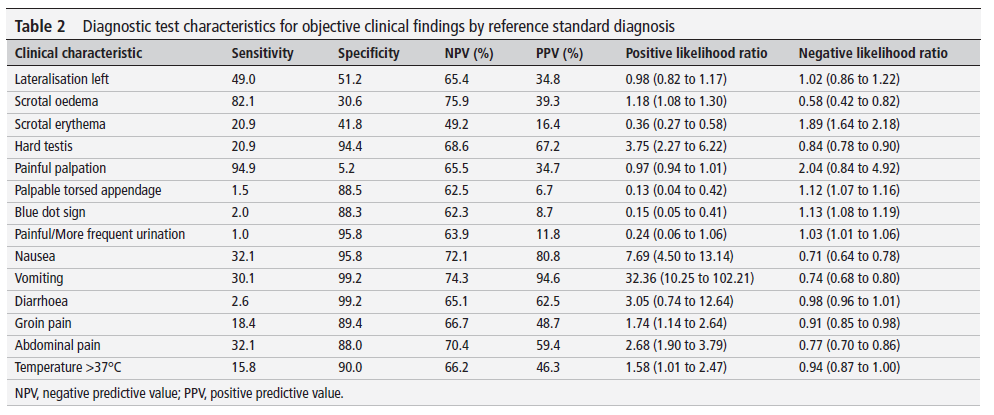
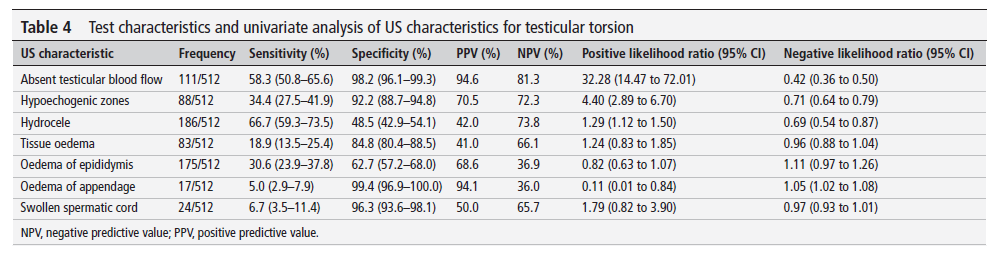
Bottom line: You can’t just rely on ultrasound when making the diagnosis of testicular torsion, which is not something our urologists always want to hear at 3am.
One is better than two?
Yarter JT, Racht J, Michels KS. Retrobulbar hemorrhage decompression with paracanthal “one-snip” method: Time to retire lateral canthotomy? Am J Emerg Med. 2023 Feb;64:206.e1-206.e3. doi: 10.1016/j.ajem.2022.11.027. Epub 2022 Nov 21. PMID: 36564334
The lateral canthotomy is a classic HALO (high acuity low occurrence) procedure, and as such causes a lot of stress among providers. Although actually relatively straight forward, the classic lateral canthotomy requires a few steps with 2 different cuts, and the apparent complexity might result in harmful delays. The authors describe a case with a classic orbital compartment syndrome from trauma. The patient had significant proptosis, and an intraocular pressure of 58 mmHg. (The patient was unconscious, and so there is no measure of visual acuity.) They describe a ‘one-snip’ technique where a single cut is made perpendicular to the eyelid margin, about 5 mm from the lateral canthal angle, extending approximately 15mm. (Procedure described in more detail here.) After this single cut, the IOP rapidly fell to 19. Discharge visual acuity was measured at 20/50, but they don’t compare it to the other eye, or provide any estimate of a baseline. Obviously, this one case report, which is lacking in almost all the clinical data you would want, probably doesn’t even count as evidence. However, I think the discussion of what counts as sufficient evidence is fascinating. In this case, there are almost certainly no unintended consequences of using this procedure over the more traditional alternative, and the benefit is immediately apparent. Either the IOP will drop and you are done, or it won’t, and in the worst case scenario you proceed with the more traditional approach. In that context, I think the theoretical benefit of simplicity allowing us to act quicker in a high stress time sensitive clinical scenario is enough to consider this procedure.
Bottom line: Despite being one of the lowest quality papers I have ever included in these write ups, this might actually be practice changing.
Can overwhelming evidence overcome entrenched dogma?
Ehmann MR, Mitchell J, Levin S, Smith A, Menez S, Hinson JS, Klein EY. Renal outcomes following intravenous contrast administration in patients with acute kidney injury: a multi-site retrospective propensity-adjusted analysis. Intensive Care Med. 2023 Jan 30. doi: 10.1007/s00134-022-06966-w. Epub ahead of print. PMID: 36715705
We have covered the myth of contrast nephropathy many times. There doesn’t seem to be a shred of evidence that the entity exists, but that doesn’t stop it from being a massive thorn in our sides. This paper looks to close a gap in the research by focusing specifically on emergency department patients with acute kidney injury. (They needed follow-up bloodwork, so it only looks at patients who were subsequently admitted, and therefore the sickest group and most likely to develop kidney injury.) They include 14,449 patients who had acute kidney injury from three emergency departments, and compare patients who received IV contrast to those who didn’t. We don’t need to spend a lot of time on this, because you already know the answer. Based on propensity matching, there was no difference in persistent renal injury based on exposure to contrast – with an odds ratio of exactly 1 (95% CI 0.89-1.11). Based on raw numbers, persistent kidney injury was actually more common among patients who didn’t receive contrast. So you could make a facetious argument that contrast actually protects kidneys, but it’s actually just going to be selection bias. The outcome was the same in subgroups with severe renal impairment (eGFR <30) and those patients admitted to the ICU. Dialysis within 180 days was actually much higher in this group than in other studies, occurring in 2.1% of patients who received contrast and 6.1% of those who didn’t. Propensity matching didn’t reveal any difference in dialysis rates (OR 0.9, 95% CI 0.65-1.124), but it is a good reminder to counsel patients with acute kidney injury that this is always a possible outcome, but that it is independent of the contrast, whatever other people might tell them.
Bottom line: The guidelines have caught up to this. If a patient needs contrast to make an important diagnosis, their creatinine is irrelevant. Most guidelines don’t come out and say it, but the evidence is pretty clear: contrast doesn’t actually hurt kidneys.
If you are still using plaster on buckle features, it’s time to stop
Perry DC, Achten J, Knight R, Appelbe D, Dutton SJ, Dritsaki M, Mason JM, Roland DT, Messahel S, Widnall J, Costa ML; FORCE Collaborators in collaboration with PERUKI. Immobilisation of torus fractures of the wrist in children (FORCE): a randomised controlled equivalence trial in the UK. Lancet. 2022 Jul 2;400(10345):39-47. doi: 10.1016/S0140-6736(22)01015-7. PMID: 35780790 [open access here]
The FORCE trial is a multicentre RCT that included 965 pediatric patients between the ages of 4 and 15 years with x-ray confirmed buckle fractures of the distal radius. The patients were randomized to either rigid immobilization (95% with a removable splint) or a bandage (roll of gauze). The primary outcome was pain at 3 days, and was identical in both groups (3/10). Pain scores were identical throughout the trial, from day 1 to 6 weeks. There were no differences in functional recovery, quality of life, complications, or days missed from school. 11% of patients crossed over from bandages to rigid immobilization, so don’t be too rigid in your conclusions. This trial makes it pretty clear that you don’t need to do anything at all about buckle fractures. However, I don’t think we need to go that far. Just stop using plaster and your patients will do so much better. (And we have known this for years.) Velcro removable splints, worn for as long as the child feels it is necessary, is all that is required. If your hospital isn’t stocking these, it’s time to make a push for it.
Bottom line: This is a well done RCT that demonstrated equivalence between rigid immobilization and a bandage in the management of distal radius buckle fractures.
You shouldn’t be using the Canadian CT head rule
Stiell IG, Clement CM, Grimshaw JM, Brison RJ, Rowe BH, Lee JS, Shah A, Brehaut J, Holroyd BR, Schull MJ, McKnight RD, Eisenhauer MA, Dreyer J, Letovsky E, Rutledge T, Macphail I, Ross S, Perry JJ, Ip U, Lesiuk H, Bennett C, Wells GA. A prospective cluster-randomized trial to implement the Canadian CT Head Rule in emergency departments. CMAJ. 2010 Oct 5;182(14):1527-32. doi: 10.1503/cmaj.091974. Epub 2010 Aug 23. PMID: 20732978
This is an old paper, but apparently we have been ignoring this evidence for more than a decade, and possibly causing a lot of harm to our patients as a result. Decision rules are supposed to go through a three stage research process: derivation, validation, and implementation. Of those, the final step is the most important, because it is the step that actually measures the impact that these rules have on decision making and patient care. Like any new diagnostic test, there is always a chance that decision rules make us worse at our job, so we really shouldn’t be using them until we see evidence of benefit. This is the implementation study for the Canadian CT head rule. It is a cluster-design, randomized, matched-pair controlled trial conducted in 12 emergency departments in Canada. That means they implemented the rule in 6 hospitals, using education, but also requiring the rule to be filled out at the time a CT was ordered, and then used another 6 hospitals as controls. The rule failed miserably. This is a rule design to decrease CT usage, but CT ordering went up by 13% in the implementation group. CT ordering also went up by 6% in the control groups, and the difference wasn’t statistically significant with a p value of 0.16. There were no clinically important missed brain injuries in either group throughout the study period. So this rule clearly does not help, and came close to being proven harmful. The best evidence suggests harm. And this study is the best case scenario, with close observation, and a requirement that the rule be filled out before every CT. Real life practice will be much worse. (I think we all know this. In modern medicine, everyone over the age of 65 gets a CT scan, even though almost none of them fit the inclusion criteria for this study. I think there is zero doubt that this rule has dramatically increased CT usage over the last few decades.)
Bottom line: The Canadian CT head rule has been proven not to help, and actually looks harmful. No one should be using this rule in clinical practice.
Full critical appraisal can be found here.
An important reminder not to adopt decision rules in their infancy (before adequate science)
Sutiman N, Khoo ZX, Ong GYK, Piragasam R, Chong SL. Validation and comparison of the PECARN rule, Step-by-Step approach and Lab-score for predicting serious and invasive bacterial infections in young febrile infants. Ann Acad Med Singap. 2022 Oct;51(10):595-604. doi: 10.47102/annals-acadmedsg.2022193. PMID: 36317570
I have been pretty vocal recently about the need for strong science when we implement decision rules. One point I have made repeatedly is the importance of external validation before accepting the numbers in these rules, as they often look much worse when repeated outside the original research centre. This is a small prospective study (258 febrile infants) that looked at the many rules that have been recently published (such as Step by Step and PECARN). It is a very high risk cohort, with 33% having serious bacterial illness and 3.5% having invasive bacterial illness. (There were 7 kids with bacteremia and 2 with meningitis. 1 of the children with meningitis also had bacteremia.) They had to exclude about half of all febrile infants because, despite being the protocol of the hospital to work them all up, many didn’t actually have blood work done. I don’t want to get into all the details, because I don’t think this is the study that will make or break any of these rules for you. However, because I know many people are rushing to adopt the PECARN rule, I thought it was important to emphasize that in this cohort, for the diagnosis of invasive bacterial illness, it only had a sensitivity of 89%, specificity of 29%, positive LR of 1.25 and negative LR of 0.38. (The numbers were very similar for serious bacterial illnesses). In other words, it looked really bad, which is why we really need to wait for external validations before rushing to adopt new decision rules. If you were interested, the Step by Step rule had a sensitivity of 100% (presented without confidence intervals), but an almost unusable specificity of 12%.
Bottom line: Be very cautious when adopting new decision rules. They are clinical tests which have the potential to both help, but also harm. We need to wait until the evidence is clear that they are helping our patients.
Blood pressure – near and dear to my heart
Anderson TS, Jing B, Auerbach A, Wray CM, Lee S, Boscardin WJ, Fung K, Ngo S, Silvestrini M, Steinman MA. Clinical Outcomes After Intensifying Antihypertensive Medication Regimens Among Older Adults at Hospital Discharge. JAMA Intern Med. 2019 Nov 1;179(11):1528-1536. doi: 10.1001/jamainternmed.2019.3007. PMID: 31424475
This is an interesting paper, and I think the results are likely to be true, but I will say up front that it is a chart review with absolutely no methods listed, so it is about the lowest quality data you can find. Also, it is focused on inpatients, not emergency patients, but I think there are still lessons to be learned. It is a large chart review from the VA system in the US looking at 14,915 older adults (>65 years) admitted with diagnoses that shouldn’t require blood pressure management: UTI, pneumonia, and PE. About 14% of these patients had their blood pressure treatment intensified after discharge (new antihypertensive, or a dose increase of at least 20%) for presumably incidentally found hypertension. They compare outcomes among patients with antihypertensive intensification to those without. There were no differences in cardiovascular outcomes at 1 year (although this might be too early to see a difference.) However, intensification of antihypertensives was associated with a higher rate of serious adverse events (4.5% vs 3.1%, HR 1.41, 95% CI 1.06-1.88) and a higher rate of readmission within 30 days (21.4% va 17.7%, HR 1.23 95% CI 1.07-01.42). This makes a lot of sense to me. High blood pressure is a chronic problem. Treating it as if it is acute is problematic, especially when you are simultaneously treating another health issue. Although this study didn’t focus on emergency department patients, this cohort is older and sicker than our average patient, and so therefore more likely to benefit from antihypertensives, so I think the lessons are good.
Bottom line: Blood pressure should generally be managed in the family doctor’s office, not the hospital.
Toxicologists will never be out of work
Rubin R. Warning About Xylazine, a Veterinary Sedative Found in Illicit Drugs. JAMA. 2022 Dec 20;328(23):2296. doi: 10.1001/jama.2022.20045. PMID: 36538321
With every passing year, we find more and more chemicals that we can put into our bodies. This brief report is based on a letter from the FDA warning that there have been increasing reports of xylazine – a veterinary tranquilizer – being implicated in overdoses, generally mixed with heroin or fentanyl. It is an alpha agonist, related to clonidine or dexmedetomidine, and so presents very similar to opioid overdoses, but with no response to narcan. There is no specific antidote, so the focus is on supportive care. In addition to the opioid effect, you can also see hypotension and bradycardia, which would be treated like a clonidine overdose. There also seem to be reports of significant skin issues, although it isn’t clear to me if that is a direct toxic effect or pressure sores similar to barbiturate blisters. There is pretty limited information at this point, and I haven’t seen any information from a toxicologist. (I am writing this in January 2023, so perhaps more information will be available at the time of publication.) That being said, although it is nice to be aware of the things our patients are taking, xylazine doesn’t have a specific toxidrome, specific test, or a specific management plan, so it probably won’t change your practice too much. According to the New York Times, more than 90% of tested drugs in Philadelphia contain xylazine, so it is certainly out there.
If you hear your patients talking about “tranq” or “zombie drug”, this would be the one.
Bottom line: Always be on the lookout for new drugs. They will certainly keep your practice interesting.
Finally, the cure for COVID??
Ben Abdallah S, Mhalla Y, Trabelsi I, Sekma A, Youssef R, Bel Haj Ali K, Ben Soltane H, Yacoubi H, Msolli MA, Stambouli N, Beltaief K, Grissa MH, Khrouf M, Mezgar Z, Loussaief C, Bouida W, Razgallah R, Hezbri K, Belguith A, Belkacem N, Dridi Z, Boubaker H, Boukef R, Nouira S. Twice-Daily Oral Zinc in the Treatment of Patients With Coronavirus Disease 2019: A Randomized Double-Blind Controlled Trial. Clin Infect Dis. 2023 Jan 13;76(2):185-191. doi: 10.1093/cid/ciac807. Erratum in: Clin Infect Dis. 2023 Feb 03;: PMID: 36367144
This is a multicenter, prospective, randomized, double-blind trial from 3 hospitals in Tunisia that looked at the use of ZINC for the treatment of confirmed COVID-19 in adult patients. Although there has been some excitement for this trial, based on a reported positive outcome, I find the results unconvincing. First of all, their real primary outcome (according to clinicaltrials.gov) was mortality, and was statistically unchanged (6.5% in the zinc group and 9.2% in the placebo group; OR 0.68, 95% CI 0.34-1.35). After the data was collected, they came up with a new primary outcome – the composite of mortality and ICU admission – and managed to get a positive result, but with a p value of 0.04, it smells a lot like p-hacking. Most importantly, there is something very weird about this population. The placebo group had a mortality of 9.2%! And they excluded all sick patients at the beginning of the trial. Even with low vaccination rates, that number just doesn’t make any sense. We never saw mortality rates as high as 10%. So this trial was negative for its primary outcome, and reports unbelievable numbers. That doesn’t sound like the kind of trial you should use to change practice.
Bottom line: This multicenter double blind RCT of zinc in COVID was actually negative, despite the widely circulated headlines to the contrary.
The evidence for nebulizers has always been a little foggy
Meckler GD, Alqurashi W, Eltorki M, Curtis SJ, Doyle E, Kam AJ, Lim R, MacPhee S, Schuh S, Wright B, Johnson DW. Epinephrine metered-dose inhaler for pediatric croup. Acad Emerg Med. 2023 Feb;30(2):144-146. doi: 10.1111/acem.14616. Epub 2022 Dec 7. PMID: 36307996
Practices with regard to nebulization vary dramatically worldwide. For asthma and COPD, there is plenty of evidence that metered dose inhalers (MDIs) work just as well as nebulizers, and so places like Toronto, which were hit hard by the original SARS, generally abandoned the infection control nightmare nebulizers for most conditions a long time ago. However, there was one exception: epinephrine for severe croup. We had no alternative. Or so I thought. I was incredibly surprised to find out at the outset of COVID-19 that there is an epinephrine MDI available, and apparently it is over the counter in the United States, but does it work for croup? This research letter is severely lacking in methodology description, but I believe it was a prospective observational trial from seven Canadian pediatric emergency departments, capturing 210 children with croup treated with an epinephrine MDI. They were using an agreed upon algorithm suggesting 5 puffs of the 125 ug/puff MDI. Mean Westley Croup score was 4 prior to treatment and fell to 2 60 minutes after treatment. They compare this mean improvement on the croup score to similar improvements seen in RCTs of nebulized epinephrine, but this trial had no comparison group. About 20% of the cohort required more than one treatment (which seems a lot higher than I am used to with nebulized epi, but is obviously very dependent on your threshold for treatment). There are many many limitations to uncontrolled observational data. It makes sense that this would work, and the need for nebulization is probably a historical practice bias. In that sense, this data is reassuring. However, 210 kids in an uncontrolled observational dataset certainly doesn’t prove equivalence to nebulized epinephrine, and severe pediatric airway obstruction is not something we should take lightly. There is a huge spectrum of croup. In my mind, if I am moving the child to resuscitation, I am probably sticking with a nebulizer for now (although I honestly can’t tell you whether that treatment is based on anything more than an observational trial of 200 kids). However, if the kid doesn’t need a resuscitation room, MDIs are probably less resource intensive in many departments, and may represent less of an infection control risk (although I am not sure that there is any such thing as an aerosol generating procedure), so I think this is a reasonable option.
Bottom line: In this small, uncontrolled, observational trial, epinephrine MDIs were given and kids generally got better.
Is high flow oxygen over blown?
Franklin D, Babl FE, George S, Oakley E, Borland ML, Neutze J, Acworth J, Craig S, Jones M, Gannon B, Shellshear D, McCay H, Wallace A, Hoeppner T, Wildman M, Mattes J, Pham TMT, Miller L, Williams A, O’Brien S, Lawrence S, Bonisch M, Gibbons K, Moloney S, Waugh J, Hobbins S, Grew S, Fahy R, Dalziel SR, Schibler A. Effect of Early High-Flow Nasal Oxygen vs Standard Oxygen Therapy on Length of Hospital Stay in Hospitalized Children With Acute Hypoxemic Respiratory Failure: The PARIS-2 Randomized Clinical Trial. JAMA. 2023 Jan 17;329(3):224-234. doi: 10.1001/jama.2022.21805. PMID: 36648469
The PARIS 2 trial compared high flow nasal oxygen to standard oxygen in 1567 pediatric patients aged 1-4 who were admitted to hospital with acute hypoxic respiratory failure. Their primary outcome was length of hospital stay, and it was actually longer in the high flow group (1.8 vs 1.5 days). ICU use was also higher (13% vs 7%). There are 2 major things to know about this trial. First, it was unblinded. I imagine that the HFNC group was ready to go home just as quickly as the standard group, but they looked sicker because of the device, so were weaned slower. Second, the mean oxygen saturation at trial enrollment was only 88% and these patients all went home in less than 2 days. In other words, it seems like the majority of these children didn’t need any oxygen at all, let alone high flow oxygen.
Bottom line: In a group of patients with very mild hypoxia, there is no benefit of early high flow humidified nasal oxygen. This trial should caution us about the massive indication creep we have seen with these devices over recent years.
The terminology we use about medical drugs can be misleading
Gøtzsche PC. The terminology we use about medical drugs can be misleading. BMJ. 2023 Mar 17;380:p601. doi: 10.1136/bmj.p601. PMID: 36931639 [free full text]
If you have followed along for any length of time, you will know that I believe language and word choice matter a lot (even if I am not much of a wordsmith myself). This short essay is worth reading. It discusses a couple different ways that basic, routine medical language shape our perspective of medical therapies. “Safe and effective” is said so often about medications that the phrase has lost all meaning, but critical reflection will reveal this phrase is actually an oxymoron. Effective means that a medication has biologic effects, which guarantees side effects, undermining the safety claim. Safe and effective are both relative, and shouldn’t be stated as absolutes. I have harped on the imbalance between “risks and benefits” many times before, but if you haven’t heard me rant, this phrase implies that benefits are guaranteed but there is only a chance of harm. That is scientifically inaccurate. The balance is between risk and “chance of benefit”, or just say “harms and benefits instead”. The final phrase this essay calls out is “risk benefit ratio”, which is only applicable if the harms and benefits are measured on the same scale (or are qualitatively similar) and therefore can be mathematically balanced. This is almost never the case, such as when we balance the high probability of a mild benefit like pain relief against the very rare probability of severe harm like death.
Bottom line: Word choice matters, and when discussing science and medicine, we really need to attempt to be precise with our language.
Just read the title
Haines JD Jr, Chop WM Jr, Swyden SN. Spontaneous pneumothorax, pneumomediastinum, and pneumopericardium in a 16-year-old drug-abusing motorcyclist surrounded by a pack of coyotes. Postgrad Med. 1989 Oct;86(5):79-80. doi: 10.1080/00325481.1989.11704431. PMID: 2798277
Honestly, there isn’t much reason to include this paper. The title just caught my eye when surfing PubMed (as one does). When the patient was returning from a camping trip, his motorcycle engine exploded and caught fire. He wasn’t injured, but did have mild smoke inhalation. Shortly thereafter, he found himself surrounded by a pack of 10 coyotes, and had a panic attack before warding off the coyotes by throwing rocks. He presented to the hospital with pneumothorax, pneumomediastinum, and pneumopericardium. They published this case to discuss “spontaneous pneumothorax”, but considering that the patient later admitted to extensive use of PCP and crack cocaine by inhalation, I think both the contention that this was spontaneous and the entire story probably falls below the threshold for publication in a medical journal. Perhaps standards were different in 1989?
Cheesy Joke of the Month
I recently received a patient complaint.
Apparently a patient presented to our emergency department after drinking a bottle of invisible ink, but after waiting for hours, he left without being seen.
After a critical incident review, it was suggested that in the future such patients be sent to the ICU.




One thought on “Research Roundup (April 2023)”