
Morgenstern, J. Sudden hearing loss: A rapid guideline review, First10EM, July 25, 2022. Available at:
https://doi.org/10.51684/FIRS.128223
Although I have ranted about the problems with guidelines in the past, there are some that do a reasonable job discussing the evidence, and they are often helpful for rarely seen conditions. Sudden hearing loss is a problem I only see occasionally in the emergency department, and I have never felt entirely confident in my evaluation. I thought this guideline from the American Academy of Otolaryngology – Head and Neck Surgery was good, so I decided to summarize the key points.
The Paper
Chandrasekhar SS, Tsai Do BS, Schwartz SR,et al. Clinical Practice Guideline: Sudden Hearing Loss (Update). Otolaryngol Head Neck Surg. 2019 Aug;161(1_suppl):S1-S45. doi: 10.1177/0194599819859885. PMID: 31369359.
Summary
I think this is a reasonably well done guideline. I am only providing a very basic summary here. For each recommendation, this guideline provides a brief discussion under each of these headings: “quality improvement opportunity”, “aggregate evidence quality”, “level of confidence in evidence”, “benefits”, “risks, harms, costs”, “benefit-harm assessment”, “value judgements”, “intentional vagueness”, “role of patient preferences”, “exceptions”, “policy level”, and “differences of opinion”. As a result, there is an easy to read summary that gives you a good sense of not just the recommendations, but the uncertainty and debate that underlies the recommendations.
The guideline focuses on sudden sensorineural hearing loss (SSNHL), which affects between 5 and 25 per 100,000 people a year. The majority of cases are idiopathic.
Sudden hearing loss is either sensorineural, conductive, or mixed. The physical exam is the key to distinguishing between conductive and sensorineural hearing loss. The official diagnosis of SSHNL requires audiometric testing and therefore won’t be made in the emergency department.
Recommendation 1: Clinicians should distinguish SSNHL from conductive hearing loss when the patient first presents.
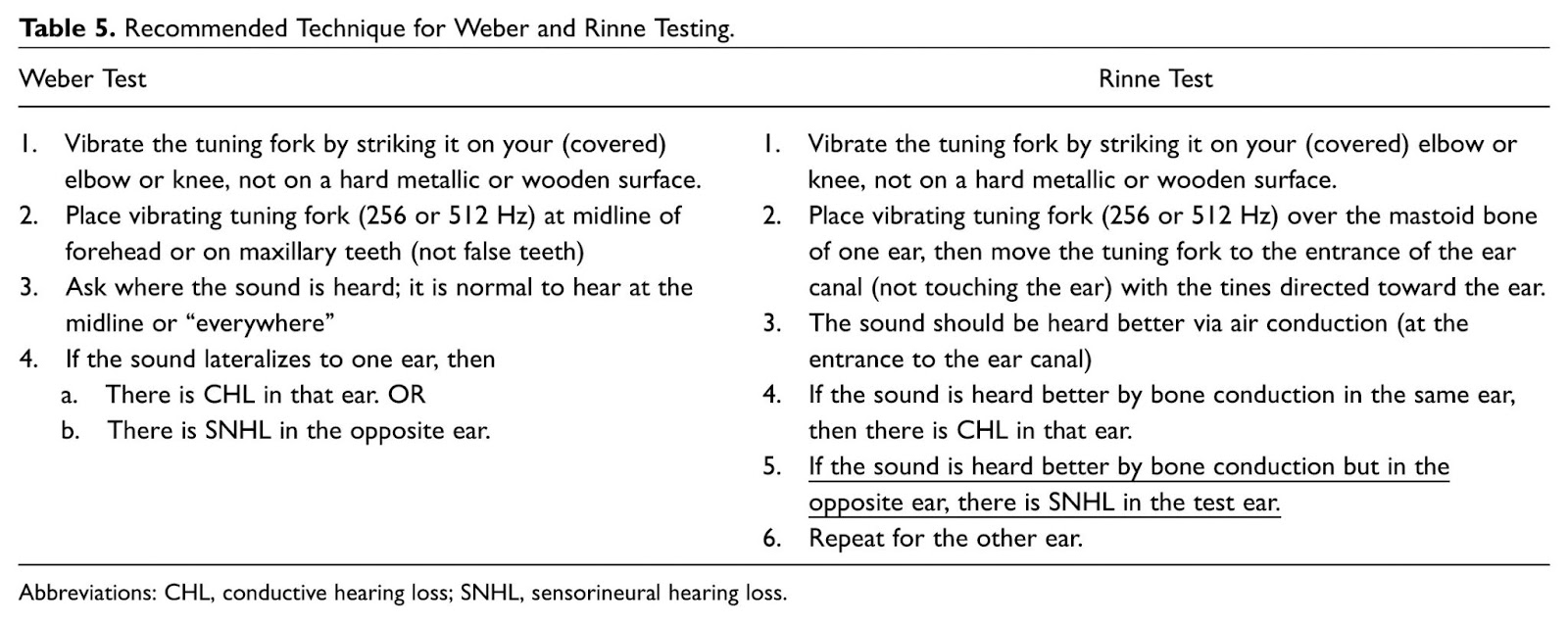
“A reasonable alternative to the Weber tuning fork test is the hum test—the patient is asked to hum and if he or she hears one’s own hum louder in the affected ear, it is likely conductive hearing loss in that ear. The sensitivity, specificity, and diagnostic accuracy of the hum test is similar to that of the Weber test.”
Recommendation 2: Clinicians should assess patients with presumptive SSNHL through history and physical examination for bilateral SHL, recurrent episodes of SHL, and/or focal neurologic findings.
Recommendation 3: Clinicians should not order routine computed tomography (CT) of the head in the initial evaluation of a patient with presumptive SSNHL. (The word routine is added here because CT will occasionally be warranted if there are focal neurologic findings on exam.)
Recommendation 4: In patients with sudden hearing loss, clinicians should obtain, or refer to a clinician who can obtain, audiometry as soon as possible (within 14 days of symptom onset) to confirm the diagnosis of SSNHL.
Recommendation 5: Clinicians should not obtain routine laboratory tests in patients with SSNHL.
The one test that may be required without other signs or symptoms is Lyme serology, as Lyme disease may provoke SSNHL. With the significant increase in Lyme distribution in recent years, this test may be more important, but there is not good data on the value of screening.
Recommendation 6: Clinicians should evaluate patients with SSNHL for retrocochlear pathology by obtaining magnetic resonance imaging (MRI) or auditory brainstem response (ABR).
“Several studies report a relatively high prevalence of cerebellopontine angle tumors in patients with SSNHL, ranging from 2.7% to 10.2% of patients who are evaluated with MRI.” Personally, I leave this to the ENT who is seeing the patient in follow-up, but in some systems the ED or primary care physician might order an MRI.
Recommendation 7: Clinicians should educate patients with SSNHL about the natural history of the condition, the benefits and risks of medical interventions, and the limitations of existing evidence regarding efficacy.
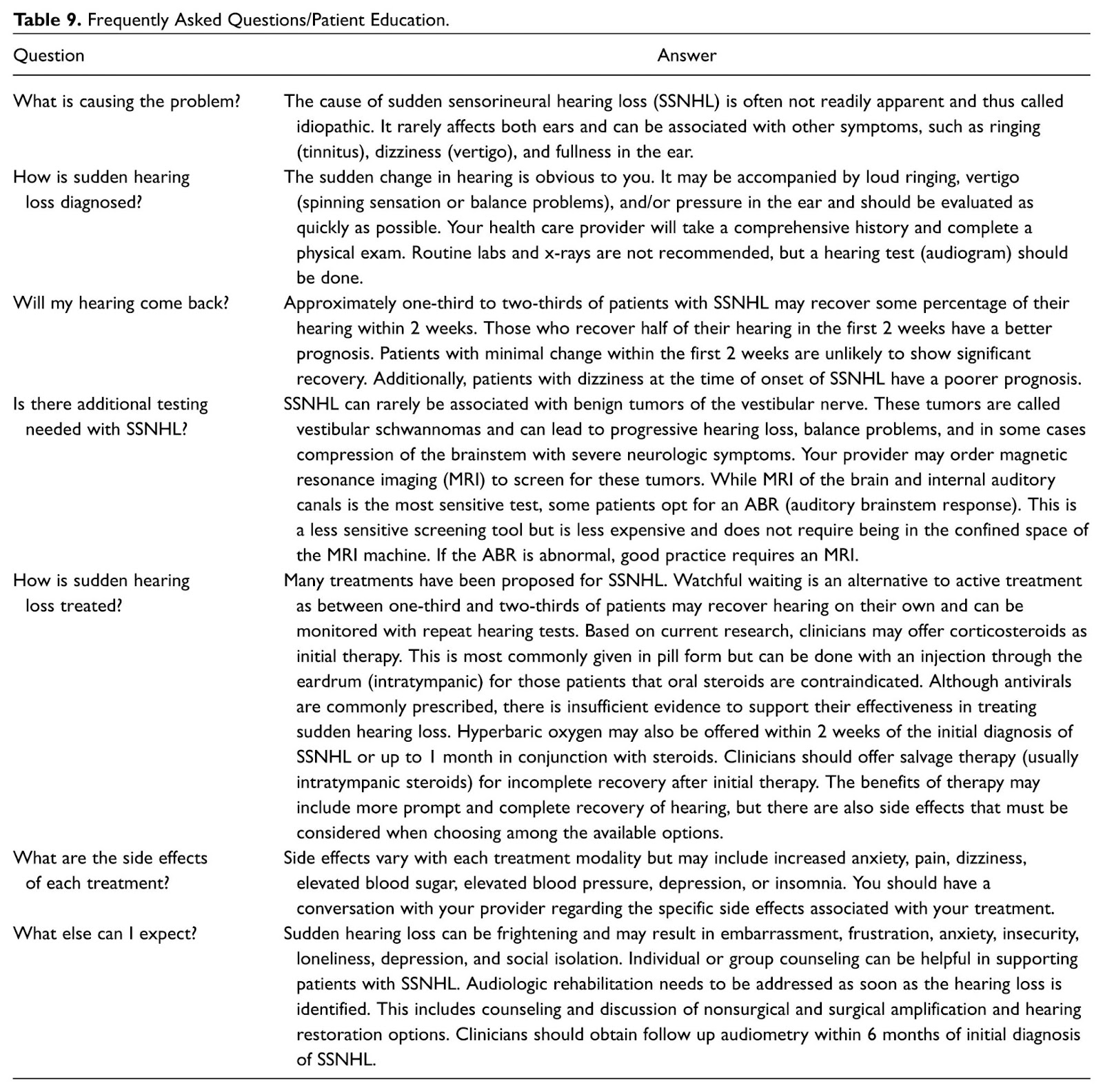
A patient handout is available here.
Recommendation 8: Clinicians may offer corticosteroids as initial therapy to patients with SSNHL within 2 weeks of symptom onset.
There are only 3 small RCTs, judged to be at high risk of bias. 2 showed no difference. 1 showed improvement in hearing in 61% of the steroid group as compared to 32% of the control group. I have not done a formal review myself, but based on that summary, it seems unlikely that steroids will help, and that harms probably outweigh the benefits.
Recommendation 9: Clinicians may offer, or refer to a clinician who can offer, hyperbaric oxygen therapy (HBOT) combined with steroid therapy within 2 weeks of onset of SSNHL. Clinicians may offer, or refer to a clinician who can offer, hyperbaric oxygen therapy (HBOT) combined with steroid therapy as salvage within 1 month of onset of SSNHL.
For acute treatment, there are 7 RCTs with a total of 392 patients, and the primary analysis of the Cochrane review showed no difference. However, an alternative analysis looking at a “25% improvement in hearing” was positive, with an NNT of only 5. This is obviously at high risk of bias, and the best we can say is, ‘we don’t know’. Personally, I wouldn’t be transferring anyone for this therapy at this time.
Recommendation 10: Clinicians should offer, or refer to a clinician who can offer, intratympanic steroid therapy when patients have incomplete recovery from SSNHL 2 to 6 weeks after onset of symptoms.
There is only a single RCT of 50 patients – but this will be the ENT’s choice either way.
Recommendation 11: Clinicians should not routinely prescribe antivirals, thrombolytics, vasodilators, or vasoactive substances to patients with SSNHL.
Recommendation 12: Clinicians should obtain follow-up audiometric evaluation for patients with SSNHL at the conclusion of treatment and within 6 months of completion of treatment.
Recommendation 13: Clinicians should counsel patients with SSNHL who have residual hearing loss and/or tinnitus about the possible benefits of audiological rehabilitation and other supportive measures.
Emergency Medicine translation
In a patient with sudden hearing loss, your job is to distinguish between conductive and sensorineural hearing loss. For sensorineural hearing loss, conduct a thorough history and physical, but barring abnormalities, you should not order lab testing or imaging. Our primary job is to counsel patients, with the understanding that almost all cases are idiopathic, and that about half resolve on their own, but that there is a risk of permanent hearing loss and tinnitus. The evidence for treatment is mixed and inconclusive. Steroids might be used, and in certain centers hyperbaric oxygen is considered. Talk with your local ENT group to determine their preference, but based on the low quality evidence discussed, I doubt that either helps.. Urgent follow-up is key, as these patients need urgent audiometry, but also may benefit from procedures such as intratympanic steroids.
Photo by Dylann Hendricks | 딜란 on Unsplash



6 thoughts on “Sudden hearing loss: A rapid guideline review”
Dear First10EM,
Just to let you know: there are two “recommendation 12” – lucky number 13 is missing ;).
Fantastic post (as always)! Big fan!
Sincerely,
Dennis De Blick (resident EM)
Thanks!
Great post Justin, really glad I am subscribing to your NL.
Interesting, I did a stint at an ear hospital ED for 3 months… the number of patientswith sudden onset of HL, turned SNHL, was frightening. The experience was practice changing for me.
Is there any mention of prednisone? Our ENTs always made a point of having us starting it in the ED.
Recommendation 8: Clinicians may offer corticosteroids as initial therapy to patients with SSNHL within 2 weeks of symptom onset.
May warrant a evidence review at some point – my guess is the evidence is very weak
I have gone through the blog post and I must admit it is very informative. I liked the writing style too. Keep up the good work and share more contents. Cheers!