
Morgenstern, J. The CLOVERS trial: Does nothing matter in sepsis?, First10EM, January 24, 2023. Available at:
https://doi.org/10.51684/FIRS.129271
Most septic patients don’t have a salt water deficit. Some people are (incorrectly) convinced that normal saline is a murder weapon. Should salt water remain the first line therapy for sepsis induced hypotension? The CLOVERS trial was just published, and it turns out that perhaps nothing you do matters.
The paper
The CLOVERS trial: National Heart, Lung, and Blood Institute Prevention and Early Treatment of Acute Lung Injury Clinical Trials Network; Shapiro NI, Douglas IS, Brower RG, et al. Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension. N Engl J Med. 2023 Jan 21. doi: 10.1056/NEJMoa2212663. Epub ahead of print. PMID: 36688507 NCT03434028
The Methods
The CLOVERS trial is a multicenter, open-label, randomized, superiority trial.
Patients
This is a convenience sample of adult patients with suspected or confirmed infection (defined as having received antibiotics) and sepsis induced hypotension (systolic blood pressure less than 100 mmHg after a 1 L bolus).
Exclusions: More than 4 hours since hypotension, more than 24 hours since hospital admission, more than 3 L of IV fluids before enrollment, fluid overload, volume depletion from non-sepsis source.
Intervention
Restrictive fluid strategy: “protocol prioritized vasopressors as the primary treatment for sepsis induced hypotension, with “rescue fluids” being permitted for prespecified indications that suggested severe intravascular volume depletion.”
Comparison
Liberal fluid strategy: “protocol consisted of a recommended initial 2000-ml intravenous infusion of isotonic crystalloid, followed by fluid boluses administered on the basis of clinical triggers (e.g., tachycardia) with “rescue vasopressors” permitted for prespecified indication”

Outcome
The primary outcome was all cause mortality by discharge or 90 days.
The Results
They enrolled 1563 patients from 60 hospitals in the United States. Patients appear evenly matched at baseline, with a mean age of about 60, a SOFA score of 3.4, and a mean systolic blood pressure of 93. Patients had received a median of 2 liters of IV fluids prior to randomization in both groups, and about 20% of each group was on vasopressors at the time they were enrolled.
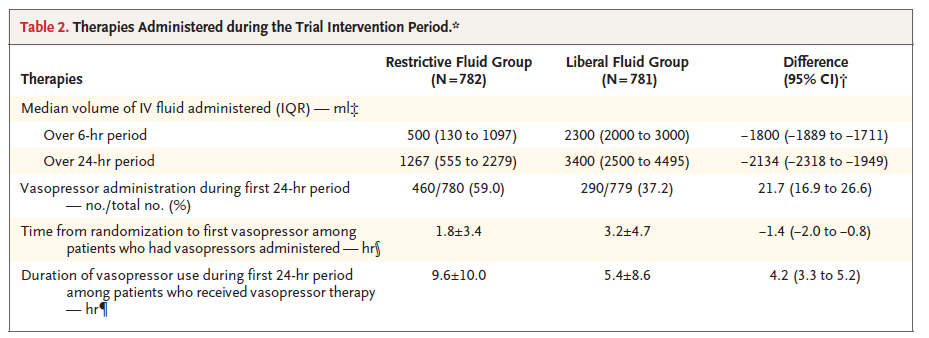
Protocol adherence was 97%, and the treatment difference between the groups appears clinically significant. Median fluids in the first 6 hours was 500 mL in the restrictive group as compared to 2300 mL in the liberal group (-1800 difference, 95% CI -1889 to -1711). Over 24 hours, the median amount of IV fluid was 1267 mL in the restive group as compared to 3400 mL in the liberal group. Vasopressor use was 59% in the restrictive group as compared to 37% in the liberal group.
There was no difference in the primary outcome of all cause mortality (14.0% vs 14.9%, ARR 0.9%, 95% CI -4.4 to 2.6%, p=0.61).
There were no statistical differences in any of the secondary outcomes (nor do there appear to be any under-powered clinically important differences), including ventilator use, renal replacement therapy, ICU length of stay, hospital length of stay, or serious adverse events. The subgroups also all look identical (although perhaps there is a hypothesis generating point estimate in the group of patients with end stage renal disease.)

My thoughts
Although these results could make you nihilistic, I don’t think there is any doubt that fluid and vasopressor support really matter for some septic patients. In my mind, what this trial really emphasizes are the limitations of our definitions in sepsis (we group together a lot of disparate conditions under a single umbrella), the limitations of our current monitoring (we don’t know if these patients had sepsis induced cardiac dysfunction), and the limitations of using blood pressure as a surrogate (when we really care about tissue perfusion). There is almost certainly a subset of patients where hemodynamic support really matters, but this trial (among many others) makes it clear that the decisions aren’t critical for the average patient. Future research really needs to delve into the heterogeneity of sepsis, rather than treating it as a homogenous state of pathology.
Although this is a large trial, it is still not large enough. The 95% confidence intervals include numbers that we would care about on both sides of the coin (from restrictive fluids decreasing mortality by 4.4% to restrictive fluids increasing mortality by 2.6%). There is no reason to think that either of those outcomes is real, but they are within the realm of statistical possibilities after this trial.
Crossover is always a problem in these kinds of trials, and can bias the results towards no effect. The restrictive group still received a fare amount of fluid, including everyone getting about 2 L IV before being enrolled. This is probably not an ideal study from the standpoint of some people in the restrictive camp, but I think it is pragmatic, as most patients will get a few boluses as we sort out what is going on in the emergency department. As compared to other trials we have seen, there is actually a pretty big gap between the groups, and I think the difference of 2 L over a 24 hours period is clinically significant and large enough that you might have expected a clinical difference in some of the outcomes (even if you don’t think 2 liters of salt water is going to change mortality).
One could imagine that the inclusion criteria for this trial were imperfect. Perhaps patients should have been selected based on some kind of volume status assessment. That being said, I don’t think that anyone has proved the clinical utility of volume assessments, so who knows if that would have made a difference.
It is also possible that the inclusion criteria encompassed too many ‘healthy’ sepsis patients. Only 20% were on vasopressors at the beginning of the trial, and only 59% of the restrictive group ended up on vasopressor at any point. The mortality was about half that seen in the early goal directed therapy trials (although mortality rates for sepsis are lower across the board as compared to 20 years ago). The inclusion of too many ‘healthy’ sepsis patients could dilute out an effect (in either direction) in the sicker subset.
Personally, I think there are some significant practical advantages of using the restrictive algorithm that wouldn’t necessarily be captured in a study. Despite decades of attention, septic patients with borderline blood pressures are still routinely admitted to ward beds with limited monitoring, and deteriorate without anyone being aware. The brief blood pressure response to a fluid bolus can be misleading, and frequently leads to patients being admitted to a floor with a lower level of care than they really require. Earlier use of vasopressors in sick patients prevents that from happening, as almost all hospitals require patients on vasopressors to be admitted to the ICU (which is where almost all of these patients deserve to be). That difference wouldn’t necessarily be identified in a trial like this, as often patients receive above average monitoring in a research context. Therefore, I personally still lean towards early vasopressors in patients I am concerned about.
I am not sure where it fits into the critical appraisal, but I really enjoyed this twitter comment, so I will include it here:
As another side note, only 27% of the restrictive group had a central line placed within the first 72 hours, despite 59% receiving vasopressors. 40% received peripheral vasopressors at some point, but it seems like almost 30% received their vasoprssors exclusively through a peripheral IV for their entire ICU stay. There were no infusion site extravasations reported in this study, and the only skin complication occurred in the liberal fluid group. In other words, as we already knew, peripheral vasopressors are safe and clearly part of the standard of care.
Bottom line
The CLOVERS trials is an open label RCT that did not demonstrate any difference (either beneficial or harmful) from using a restrictive fluid strategy over a liberal fluid strategy in sepsis induced hypotension. Do whatever you please for now, although for practical reasons I am still leaning towards earlier vasopressors in sepsis.
Other FOAMed
Peripheral vasopressors: the myth and the evidence
The BaSICS trial: Normal saline has been fine all along
References
National Heart, Lung, and Blood Institute Prevention and Early Treatment of Acute Lung Injury Clinical Trials Network; Shapiro NI, Douglas IS, Brower RG, et al. Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension. N Engl J Med. 2023 Jan 21. doi: 10.1056/NEJMoa2212663. Epub ahead of print. PMID: 36688507


6 thoughts on “The CLOVERS trial: Does nothing matter in sepsis?”
Nice