
October 2020. A month that many have declared the worst of all time, but can it really be that bad if you are getting another edition of the research roundup, with all sorts of EBM goodness?
Another negative TXA trial. Life was simpler when this was a miracle drug.
Rowell SE, Meier EN, McKnight B, et al. Effect of Out-of-Hospital Tranexamic Acid vs Placebo on 6-Month Functional Neurologic Outcomes in Patients With Moderate or Severe Traumatic Brain Injury. JAMA. 2020 Sep 8;324(10):961-974. doi: 10.1001/jama.2020.8958. PMID: 32897344.
This might be one of the most controversial topics in emergency medicine right now, but there is a new study on TXA in traumatic brain injury. Everyone knows about CRASH-3 by now, even if no one agrees on what the trial actually tells us, with some people pointing out that the primary and most important outcomes were clearly negative, while others point to subgroups that might benefit. This RCT was actually done before CRASH-3, but is only getting published now, which sort of tells you the results are negative. In this trial, they randomized 1063 prehospital patients with traumatic brain injury, a GCS between 3 and 12, and at least 1 reactive pupil to placebo or 1 of 2 TXA doses. There was no difference in the primary outcome of favourable neurologic outcomes. There was no difference in mortality. This trial is much smaller than CRASH 3, and so certainly doesn’t override those results. Like CRASH-3 it is a negative trial, and so certainly doesn’t support the use of TXA. It doesn’t look at the subgroups that got everyone excited in CRASH3, so doesn’t add to that discussion, but those were just subgroups and so shouldn’t be driving our clinical practice.
Bottom line: This is another negative RCT looking at TXA in traumatic brain injury. At this time, TXA should probably not be used routinely, but more studies are indicated to follow up the subgroups identified in CRASH-3.
Lawati, K.A., Sharif, S., Maqbali, S.A. et al. Efficacy and safety of tranexamic acid in acute traumatic brain injury: a systematic review and meta-analysis of randomized-controlled trials. Intensive Care Med (2020). https://doi.org/10.1007/s00134-020-06279-w [free full text]
I will briefly add this systematic review on the topic. I won’t do much critical appraisal, as I was lucky enough to be invited to be an author on the paper. This meta-analysis combines all the RCTs looking at TXA for TBI. The key findings were that TXA likely had no effect on mortality (RR 0.95; 95% CI 0.88–1.02; risk difference (RD) 1.0% reduction; 95% CI 2.5% reduction to 0.4% increase; moderate certainty) or disability. Unfortunately, not enough trials reported on subgroups to allow an analysis, so that will remain an open debate, but these results look pretty negative to me. Personally, I am not prescribing TXA in these patients.

Pediatric Inflammatory Multisystem Syndrome
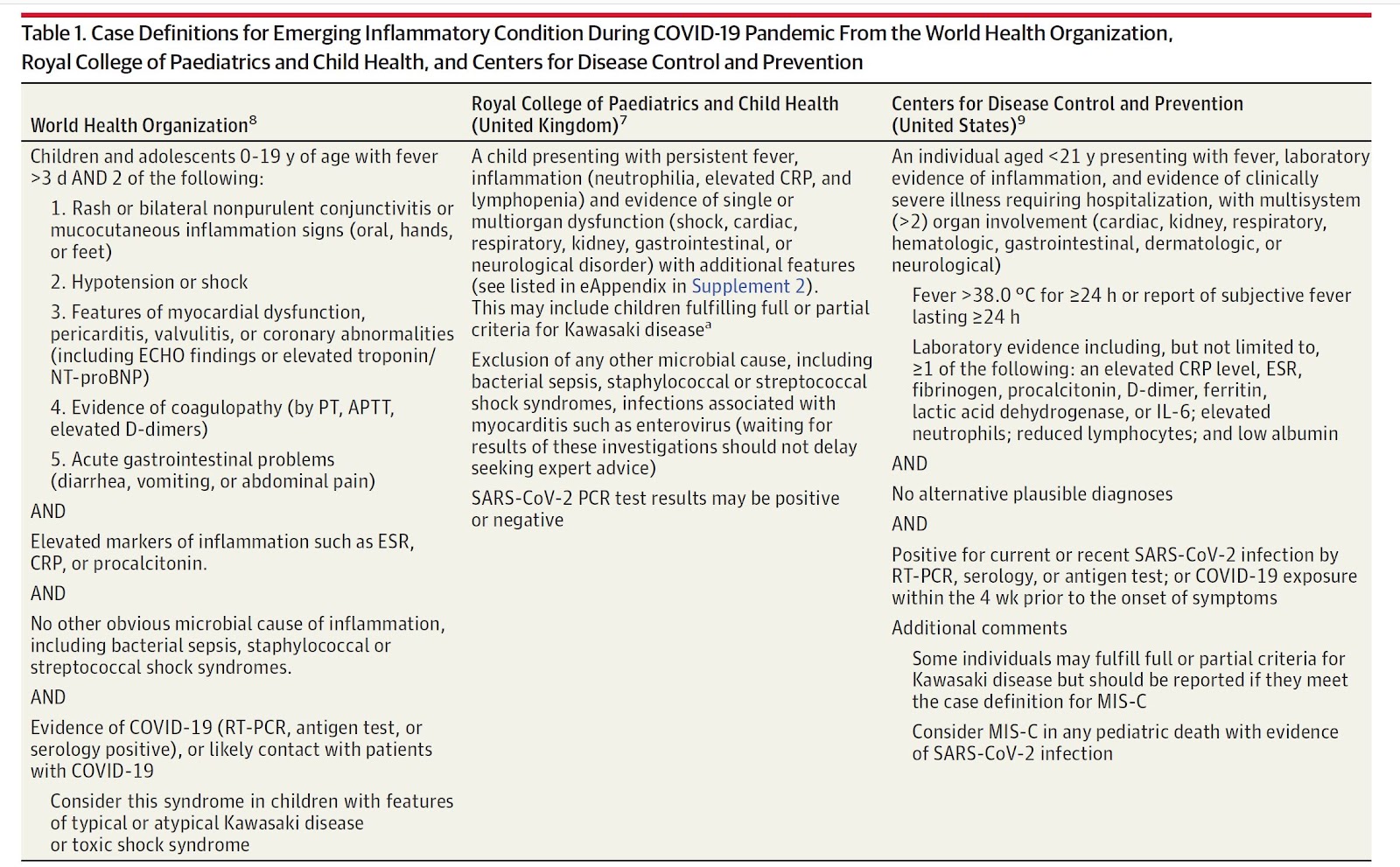
Whittaker E, Bamford A, Kenny J, et al. Clinical Characteristics of 58 Children With a Pediatric Inflammatory Multisystem Syndrome Temporally Associated With SARS-CoV-2. JAMA. 2020;e2010369. doi:10.1001/jama.2020.10369 PMID: 32511692
By now, I am sure that everyone has heard that children with COVID can get a “Kawasaki-like illness”. However, probably because it was initially described as “Kawasaki-like”, my understanding of this condition was completely wrong until I read this paper (and another very similar cohort). This is a chart review that looks at 58 children with PIMS or “Pediatric Inflammatory Multisystem Syndrome” in the United Kingdom. There is a full Rapid Review post on PIMS here, but I think the important point is that only a minority of these patients have classic Kawasaki symptoms. In fact, I cannot see anything that really differentiates PIMS from the presentations of severe COVID we are seeing in adults. There is significant inflammation and multi-organ involvement, temporarily related to a SARS-CoV-2 infection. You can look at the diagnostic criteria for yourself, but this just sounds like COVID to me. The big concern is that a significant number of these children develop coronary aneurysms (14% in this cohort), and the rate of aneurysm seems to be the same whether or not the patient has classic Kawasaki symptoms, so it will be a hard diagnosis to make. There is also a very high rate of myocarditis and this select group of pediatric patients is pretty sick. Again, you can read a little more detail about this condition in the main post.
Bottom line: Much like in adults, COVID has made the phrase “just a virus” even sillier than it normally is. It isn’t clear exactly which patients we need to be screening for coronary artery aneurysm and myocarditis, but we are going to need to catch a significantly wider net than we usually do. This is going to make for a very difficult RSV and flu season this year, and pediatric wards had better be planning for very high rates of occupancy. However, these children all seem pretty sick, so I wouldn’t necessarily go fishing for this in well appearing children with a few days of fever (even though some guidelines are already suggesting that).
Delayed antibiotics are dumb
Rowe TA, Linder JA. Delayed Antibiotic Prescriptions in Ambulatory Care: Reconsidering a Problematic Practice. JAMA. 2020;10.1001/jama.2020.2325. doi:10.1001/jama.2020.2325 PMID: 32297898
My full rant on this issue can be found here. It is easily summarized: Delayed antibiotics are dumb. Either a patient needs antibiotics or they don’t. If a patient needs antibiotics, a delayed prescription is harmful. If the patient doesn’t need antibiotics, a delayed prescription is harmful. Thus, delayed antibiotics are dumb.
Door to triage time: the hidden, dirty secret of busy emergency departments
Hansen B, Bonin D, Van Aarsen K, Dreyer J. Door-To-Triage Time in a Canadian Tertiary-Care Center. J Emerg Med. 2020 Sep 8:S0736-4679(20)30697-1. doi: 10.1016/j.jemermed.2020.07.015. PMID: 32917452
This is a neat little study looking at an under-appreciated problem in emergency medicine: door to triage time. This is the time that patients spend waiting in line before ever seeing a triage nurse. In this single centre prospective observational study of 935 walk in patients, they found a median door to triage time of 12 minutes, and that increased to 22 minutes on their busiest day (Monday). The range was massive, with a few unfortunate outliers waiting more than 75 minutes from the time they arrived at the hospital until they first saw a nurse. Even worse, somehow a CTAS 1 patient waited more than 45 minutes to be triaged! They don’t give us any details, but there is a reasonable chance that this was a patient who deteriorated while waiting in line. My guess is that these numbers are far worse in many hospitals, as the “Hawthorne effect” probably downplays the numbers in a study setting. This is an incredibly important metric, as it represents time in our emergency department where potentially critically ill patients are completely ignored by the medical system. (Of course, our nurses are great at “eyeballing” the line for people who look sicker, but frequently our line is so long that the triage nurses can’t see everyone in it.) In my mind, technological solutions should help a lot. Most patients should be able to self register, either on a phone, or at airport-like kiosks. The chief complaint they enter would then act as a sort of pre-triage, so that patients with complaints like chest pain could be pulled from the line while ankle sprains could wait longer. Perhaps more importantly, we need to unburden our triage nurses. This is the most hated position in every hospital I have ever worked in, and the hated parts have nothing to do with triage. We make our nurses ask endless streams of screening questions, check medications, and take histories that have nothing to do with the triage process. Screening for allergies may be important, but it can’t be a priority when there is a huge line of potentially critically ill patients who haven’t even been assessed. Triage needs to be fast and efficient. Chief complaint and vital signs should suffice. Once the patient is in the department, those other questions can be addressed on a secondary nursing assessment.
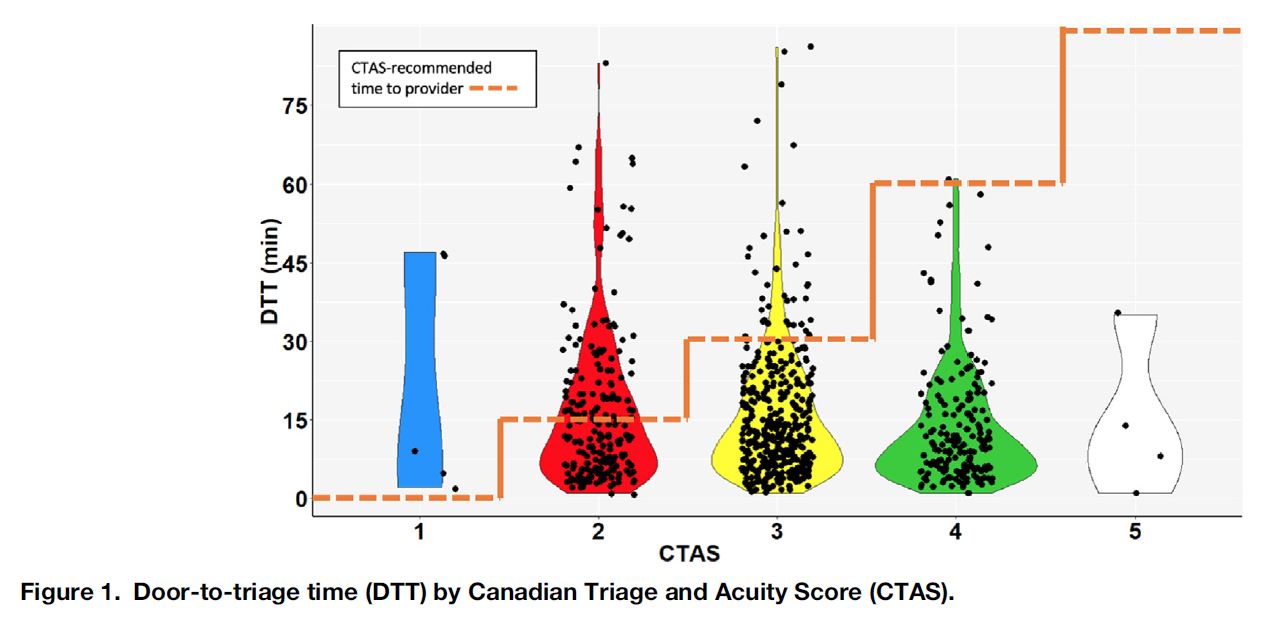
Bottom line: At most hospitals, there is a lot of work that needs to be done to unburden our triage nurses and fix this “door to triage” problem.
At the Intersection of Fear, Grief, and Love
Veal CT. At the Intersection of Fear, Grief, and Love. Ann Intern Med. 2020;10.7326/M20-4113. doi:10.7326/M20-4113 PMID: 32716704
This is just a great essay. Driving to medical school should not be an experience that makes anyone scared for their life. Not much else to say aside from I strongly recommend reading it. Full text available free here.
Squeezing out cellulitis
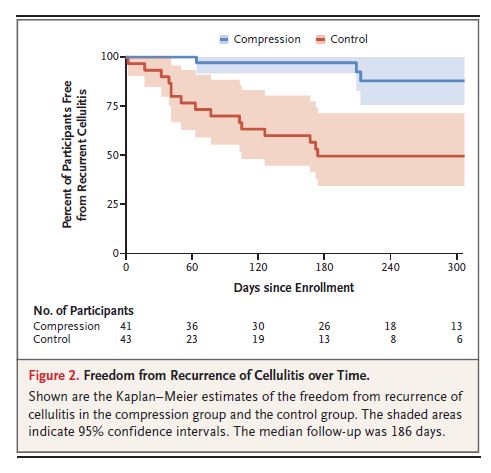
Webb E, Neeman T, Bowden FJ, Gaida J, Mumford V, Bissett B. Compression Therapy to Prevent Recurrent Cellulitis of the Leg. N Engl J Med. 2020 Aug 13;383(7):630-639. doi: 10.1056/NEJMoa1917197. PMID: 32786188
Emergency medicine is usually more about reaction than prevention, but we see so many patients with recurrent problems that knowing about preventative therapies is essential. Cellulitis is a relatively simple condition that we still frequently get wrong, whether it is the diagnosis of “bilateral cellulitis” or the insistence that IV antibiotics are somehow magically better than oral. Ignoring the factors that predispose patients to cellulitis may be yet another mistake. This is a single center, open-label RCT that randomized 84 patients with recurrent cellulitis (2 or more episodes in the same leg in the 2 years before the trial) and chronic leg edema to compression stockings or standard care. (The prescription of compression stockings was somewhat complex, and I would need some education or someone to refer to to operationalize this right now). The primary outcome was the recurrence of cellulitis, but cellulitis is never specifically defined, which could be a problem considering how often we misdiagnose this condition. However, those misdiagnoses would occur in real life as well, and so if we can prevent these patients from having hospital visits and extended courses of antibiotics, that is a valuable outcome whether or not the diagnosis was correct. The lack of blinding is a big problem in this trial, especially when the diagnosis was being influenced by “lymphedema specialists” who are very likely to think edema is a problem. The trial was stopped early, not based on a predefined end-point, but because these lymphedema specialists thought they noticed a big difference between the groups. And there was a pretty big difference. Recurrent cellulitis occurred in 15% of the compression group as compared to 40% of the controls (HR 0.23 95% CI 0.09-0.59). Hospitalization occurred in 7% of the compression group compared to 14% of controls. There was no difference in quality of life between the two groups, which would probably be the biggest concern about widely using compression stockings (but probably also indicates a trade off between the annoyance of an episode of cellulitis versus the annoyance of constantly wearing stockings.)
Bottom line: This trial has some significant limitations which severely limit our conclusions. I want to see stronger studies, but this is enough to at least discuss the benefits with patients I see in the ED.
Should Evidence Come with an Expiration Date?
Greene P, Prasad V, Cifu A. Should Evidence Come with an Expiration Date?. J Gen Intern Med. 2019;34(7):1356-1357. doi:10.1007/s11606-019-05032-4 PMID: 31062228
This editorial asks the question: does evidence have an expiry date in evidence based medicine? They frame their question around a new RCT that demonstrated no benefit from aspirin in primary prevention of cardiovascular disease. There were multiple old studies that demonstrated a benefit in a similar population, but they point out that over time the risk of coronary artery disease and MI has dropped significantly. Thus, they suggest the original trials were correct (there was a benefit at that time), but because the population has changed the new trial is also correct (there is no benefit now). External validity has always been an important part of science. We need to know if the people in the trial look like the patients we are going to treat. However, I don’t think we frequently consider the impacts that time has on external validity. There are many temporal trends that could impact medical evidence: smoking rates falling, STI rates increasing, etc. Old evidence may also “expire” in the light of new therapies. For example, does our evidence for thrombolytics in stroke really apply in a modern era of endovascular management? Long time readers will be familiar with my emphasis on repetition as a bedrock of science, but this article points out that even practices that seem to be based on solid evidence may need to have studies replicated if the baseline population has changed over time.
Sometimes it isn’t the evidence, but the concept that needs a expiration date
The STAND trial: Jaung R, Nisbet S, Gosselink MP, Di Re A, Keane C, Lin A, Milne T, Su’a B, Rajaratnam S, Ctercteko G, Hsee L, Rowbotham D, Hill A, Bissett I. Antibiotics Do Not Reduce Length of Hospital Stay for Uncomplicated Diverticulitis in a Pragmatic Double-Blind Randomized Trial. Clin Gastroenterol Hepatol. 2020 Mar 30:S1542-3565(20)30426-2. doi: 10.1016/j.cgh.2020.03.049. PMID: 32240832
We have covered this topic a number of times before in these research roundup write ups. This is another RCT demonstrating no difference between antibiotics and placebo in uncomplicated diverticulitis. The group included in this study confuses me a bit (you had to be sick enough to be admitted, but couldn’t have more than 1 SIRS criteria, which sort of defines you as not sick enough to be admitted). However, there has never been a trial demonstrating benefit from antibiotics, and this is the third RCT showing no benefit. The trials aren’t perfect, but it is becoming eminently clear that not all diverticulitis patients need antibiotics. The big remaining question is which patients should be treated.
Bottom line: Antibiotics aren’t needed in most patients with uncomplicated diverticulitis. It is unclear which patients, if any, need antibiotics.
Don’t just do something, stand there
Farrow GS, Delate T, McNeil K, et al. Vitamin K versus warfarin interruption alone in patients without bleeding and an international normalized ratio > 10. J Thromb Haemost. 2020;18(5):1133-1140. doi:10.1111/jth.14772 PMID: 32073738
Given that everyone prescribes DOACs these days instead of warfarin (for good or for bad), the question of what to do with an extremely elevated INR has become far less relevant. This used to be a weekly referral, which much like the asymptomatic hypertension patient, would simply get referred right back to their GP for management. I don’t think I have seen anyone referred in for an elevated INR in more than a year, but just in case it comes up, this chart review study reinforces what we already knew: as long as the patient isn’t bleeding, they don’t need treatment. These authors used the massive Kaiser database to identify 809 patients with an INR more than 10, and compared patients who were prescribed vitamin K to those who were not. The rate of subsequent bleeding that required either an ED visit or hospitalization was that same (5% with vitamin K and 7% without). The rate of major bleeding was also the same (3% vs 4%). All cause mortality was higher in the group that was prescribed vitamin K (15% vs 10%, p=0.03). Of course, this isn’t randomized data, and there are going to be confounders. The groups actually look very similar based on the demographics collected, but someone made the decision not to give vitamin K, and they made that decision for a reason. I doubt that vitamin K is actually causing an increase in mortality (although these patients are on warfarin for a reason and over-correcting it could be an issue), but this data certainly doesn’t support any benefit from treatment. For most patients, as long as they aren’t bleeding, I simply ask them to hold their warfarin and have the number rechecked in 3-4 days. I do take the opportunity to review the indication for warfarin, as a surprisingly high number of patients are on blood thinners without any indication.
Bottom line: Don’t just do something, stand there – even if the patient’s INR is “critically high” according to the lab.
NSAIDs and nonunion
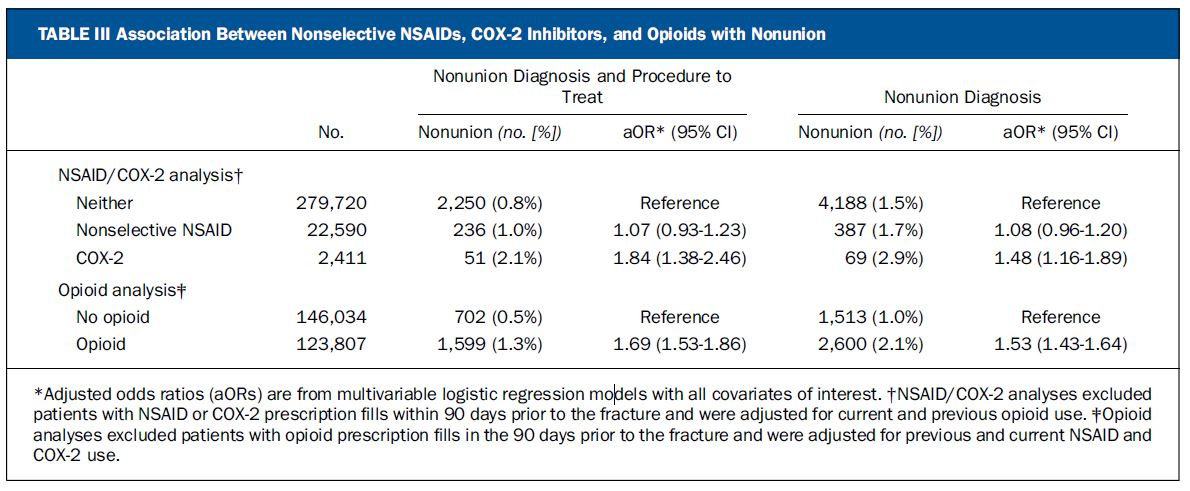
George MD, Baker JF, Leonard CE, Mehta S, Miano TA, Hennessy S. Risk of Nonunion with Nonselective NSAIDs, COX-2 Inhibitors, and Opioids. J Bone Joint Surg Am. 2020;10.2106/JBJS.19.01415. doi:10.2106/JBJS.19.01415 PMID: 32453106
Speaking of low quality retrospective data that refutes a commonly accepted medical myth, let’s talk NSAIDs and fractures. This is another big database study looking at the association between NSAIDs, COX-2 inhibitors, and opioids with nonunion after long bone fractures in adults. They identify a total of 339,864 fracture that fit their criteria, and the overall rate of nonunion requiring an intervention was 0.9%. They looked at whether these patients filled a prescription for any of the medications of interest, and compared that to nonunion rates. Nonselective NSAIDs had no difference on the nonunion rate (1.0% with vs 0.8% without), but COX-2 inhibitors did (2.1% vs 0.8%, adjusted OR 1.84, 95% CI 1.38-2.46). This is a statistical difference, but it is a really small clinical difference, and the number of confounders in this data make the conclusion far from certain. Opioids were also associated with a higher rate of nonunion, but I am less convinced of that data, as the difference seems to to come from a decrease in nonunion in the control group rather than in increase in the opioid group (0.5% vs 1.3%) when you compare to the NSAID numbers. I think the most concerning number in this study is that, presumably because of the myth that NSAIDs are bad, opioids are prescribed almost 5 times as often as NSAIDS. (However, we might have to be careful with this American data, because I recently saw another study that said that Americans prescribe more than 100 times the quantity of opioids postoperatively than any other country in the world.) Of course, this data is a bit of a mess. NSAIDs can be bought over the counter, and opioids are pretty easy to come by as well. Furthermore, there is probably a reason that some patients are given prescriptions for strong pain medications while others aren’t. (Worse fractures are probably more likely to get prescriptions, but will also have a higher rate of nonunion.) Overall, this study fits with basically all the human data on the topic: NSAIDs are fine, and should probably actually be preferred when managing pain from broken bones.
Bottom line: Broken bones hurt. Treat the pain. Like with all other pain, consider the side effects of the various analgesics, and choose the best options for the patient in front of you, but don’t worry too much about nonunion.
Good Samaritan App
Derkenne C, Jost D, Roquet F, et al. Mobile Smartphone Technology Is Associated With Out-of-hospital Cardiac Arrest Survival Improvement: The First Year “Greater Paris Fire Brigade” Experience. Acad Emerg Med. 2020 May 23. doi: 10.1111/acem.13987 PMID: 32445436
This is the paper we covered on the SGEM Hot off the Press series this week, so I won’t go into too much detail. It is a look at one of the apps that can be used to inform individuals trained in CPR about cardiac arrests near them, as well as map the locations of local AEDs. The idea is great, but as of yet relatively unproven. This is an observational study that claims there is an association between app use and survival from out of hospital cardiac arrest, but I am not convinced. They didn’t compare a group of patients in whom the app was available to a group of patients in whom the app was not available. Instead, they compared patients who received treatment to those who did not receive treatment. That comparison doesn’t actually demonstrate that the app helps, but just that CPR helps, which we already knew. Add that to the many confounders possible in this data, and I don’t think the study really demonstrates all that much.
Bottom line: Apps to direct first responders to patients in cardiac arrest make a lot of sense, and could be a really good use of smartphone technology, but we don’t know if they actually save lives, whether they might distract from other important interventions, or whether they are worth the cost. Thankfully, there is an RCT ongoing to answer some of those questions.
Remember, this is an SGEM HOP paper. Listen to the full critical appraisal on the SGEM, and then leave your comments and questions. The best questions and comments get published in Academic Emergency Medicine.
Cheesy Joke of the Month
Two guys walked into a bar. The third guy ducked.
Morgenstern, J. Research Roundup – October 2020, First10EM, October 26, 2020. Available at:
https://doi.org/10.51684/FIRS.49059


3 thoughts on “Research Roundup – October 2020”
Excellent blog
Thank you